
Abstract
Metabolomics is a post-genomics research field for analysis of low molecular weight compounds in biological samples and has shown great potentials for elucidating complex mechanisms associated with diseases. However, metabolomics studies on gastric cancer (GC), which is the second leading cause of cancer death worldwide, remain scarce, and the molecular mechanisms to metabolomics phenotypes are also still not fully understood. This study reports that the metabolic pathways can be exploited as biomarkers for diagnosis and treatment of GC progression as a case study. Importantly, the urinary metabolites and metabolic patterns were analyzed by high-throughput liquid chromatography mass spectrometry (LC-MS) metabolomics strategy coupled with chemometric evaluation. Sixteen metabolites (nine upregulated and seven downregulated) were differentially expressed and may thus serve as potential urinary biomarkers for human GC. These metabolites were mainly involved in multiple metabolic pathways, including citrate cycle (malic acid, succinic acid, 2-oxoglutarate, citric acid), cyanoamino acid metabolism (glycine, alanine), primary bile acid biosynthesis (glycine, taurine, glycocholic acid), arginine and proline metabolism (urea, l-proline), and fatty acid metabolism (hexadecanoic acid), among others. Network analysis validated close association between these identified metabolites and altered metabolic pathways in a variety of biological processes. These results suggest that urine metabolic profiles have great potential in detecting GC and may aid in understanding its underlying mechanisms. It provides insight into disease pathophysiology and can serve as the basis for developing disease biomarkers and therapeutic interventions for GC diseases.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Gastric cancer (GC) is one of the most common malignancies and the second cause of cancer-related death worldwide [1]. However, because of its asymptomatic properties, most patients are frequently misdiagnosed, leading to a poor prognosis of GC patients with a 5-year survival rate of less than 30 % [2]. Moreover, clinical surgical specimens are rarely obtained, and traditional biomarkers of GC are not very effective. Challenge tests in particular provide deeper insight into changes in human metabolism that is often not captured from GC. Many studies in the field of metabolomics have contributed to the discovery and establishment of powerful diagnostic tools in the management of cancer [3–5]. Diagnostic biomarkers of human GC could be useful for detecting cancer or assessing the efficacy of treatment. Lack of adequate screening methods has resulted in the majority of GC patients diagnosed at an advanced stage of the disease. Thus, a full understanding of the molecular mechanism of human GC and identification of biomarkers for the early diagnosis and effective treatment is crucial. The diagnosis of GC is detected mainly by direct endoscopy, and efforts have been made to develop biomarkers for GC using omics. Metabolomics offers the opportunity to understand the molecular mechanism and to aid in the identification of diagnosis biomarkers of human GC [6].
Recently, most investigations have been focused on identifying the altered genes and proteins that play a role in cancer progression. Urine has been shown to contain a wealth of metabolic information that may be altered due to underlying disease and do satisfy the criteria of minimal invasiveness [7, 8]. The markers acquired from urine are noninvasive and convenient, and the urinary metabolic profiling could be used to get metabolites as GC biomarkers [9]. Among the various techniques conventionally used for cancer metabolic profiling, LC-MS has been proven to be a robust metabolomic tool and is widely applied in metabolite identification and quantification based on its high sensitivity, peak resolution, and reproducibility [10–13].
The missing link between urine and phenotype can be established, which may provide information of GC, thus improving our understanding of the pathogenic mechanisms and metabolic phenotype of GC. Recently, metabolomics has been used to characterize the metabolic perturbation and identify potential biomarkers [14, 15]. Exploring the mechanism of GC and identifying the markers for early diagnosis is of significant importance and has a great potential to reduce the morbidity and mortality of GC. In the present study, we hypothesized that the distinct metabolic profiles are reflected in GC. To test this hypothesis, we utilized LC-MS metabolomics to fingerprint urine and to examine metabolite signatures changes and pathway analysis in GC using LC-MS tool combined with the pattern recognition methods.
Materials and Methods
Ethical Statement
The ethics committee of Heilongjiang University of Chinese Medicine approved the study protocol, and all patients provided written and informed consent. All clinical investigations were conducted according to the principles expressed in the Declaration of Helsinki.
Patient Recruitment and Sample Collection
Patients who suffered from GC at Hospital affiliated to Heilongjiang University of Chinese Medicine were included in the screening of metabolite biomarker cohort study. All patients (n = 13) aged from 35 to 46 were eligible for enrollment. The control group (n = 9) included healthy people that of no significantly different baseline compared with the GC group. The outcomes of health survey questionnaire in GC patients were assessed, and the related clinical information was also collected. Exclusion criteria are that patients (nonsmoker) had no other types of cancer, cardiac insufficiency, renal inadequacy, respiratory failure, alimentary tract hemorrhage, diabetes mellitus, renal failure, rheumatism, or other diseases that will affect the clinical observations and biological indicators. These GC patients had not taken any medicines or supplements before they collected urine samples.
Urine sample of was centrifuged at 5000 rpm for 20 min to remove any solid debris. Fractions (10 mL) of the urine supernatants were then stored at −20 °C until LC-MS analysis. Thawed urine samples were collected after centrifugation at 5000 rpm for 10 min at 4 °C, and the supernatant was then filtered through a 0.22-μm syringe filter, 5 μL of the supernatant was injected into the LC-MS.
Chemicals and Reagents
Acetonitrile was also purchased from Merck (Darmstadt, Germany); methanol (HPLC grade) was purchased from Fisher Scientific Corporation (Loughborough, UK); water was produced by a Milli-Q Ultra-pure water system (Millipore, Billerica, USA); formic acid was obtained from Honeywell Company (Morristown, New Jersey, USA); and leucine enkephalin was purchased from Sigma-Aldrich (St. Louis, MO, USA). All other reagents were HPLC grade.
Metabolomics Analysis
Ultra-performance Liquid Chromatography
Analysis was performed on an LC system (Waters Corp., Milford, USA), equipped with chromatography column with 0.17-μm stationary phase. The column temperature was maintained at 40 °C, and then gradient mobile phase was composed of phase a (water with 0.1 % formic acid) and phase b (acetonitrile containing 0.1 % formic acid). The gradient for the urine sample was as follows: 0–5 min, 1–25 % b; 5–9 min, 25–50 % b; 9.1–13 min, 50–99 % b. The injection volume was 5 μL, and the flow rate of the LC system was 0.5 mL/min. Each patient samples were followed by control samples, with an interval of control samples to avoid cross-contamination. All samples were maintained at 4 °C during the analysis.
Accurate Mass Spectrometry
MS system was operated using the ESI+ and ESI− mode, and the mass range was set at 50–1000 m/z in the full scan mode. Mass spectrometry was performed by using an accurate mass time-of-flight mass spectrometry system (Waters Corp., Milford, USA) equipped with an electrospray ionization source that operates in positive ionization mode (ESI+) and negative ionization mode (ESI−). The optimal capillary voltage was set at 3200 V and cone voltage at 35 V. The desolvation temperature was set at 280 °C and source temperature at 120 °C. Desolvation gas flow rate was set at 500 L/h, and cone gas flow was maintained at 50 L/h. Leucine enkephalin was used as the reference compound for accurate mass measurement. Data were collected at a rate of 1 MS spectrum per second with a scan time of 0.4 s, an inter-scan delay of 0.1 s, and a lock spray frequency of 10 s.
Metabolite Identification
The chemical structures of the candidate metabolites were determined as follows: first, the MassFragment™ application manager (Waters Corp., Milford, USA) was searched by mass weight and a list of candidates was obtained; then, tandem mass analysis was carried out, and according to the possible fragment mechanisms, items without characteristic mass fragment information were removed from the list, with the most probable metabolic indicators survived; finally, by comparing the retention times and mass spectra to the commercial standards, part of the related metabolites were structurally confirmed. The accurate mass and structure information of candidate metabolites were also matched with those of metabolites obtained from HMDB (www.hmdb.ca) and METLIN (metlin.scripps.edu/) databases.
Multivariate Data Processing and Statistical Analysis
Multivariate analyses of log-transformed and auto-scaled metabolome data were performed using MetaboAnalyst (www.metaboanalyst.ca), including principal component analysis (PCA), and partial least squares discriminant analysis (PLS-DA) as well as orthogonal partial least squares discriminant analysis (OPLS-DA). Here, this rigorous approach to a metabolomics workflow results in higher data fidelity for biomarker discovery while reducing bias caused by data over-fitting. PCA are displayed as score plots that represent the scatter of the samples, showing the similarity or difference among the groups. VIP plot of the OPLS-DA was carried out to select distinct variables as potential markers for distinguishing GC patients from healthy controls. Metabolic pathways were performed in MetaboAnalyst web portal. Pathway was performed on KEGG database source to identify and facilitate further biological interpretation. The metabolites and corresponding pathways were imported into the advanced Cytoscape software (v 2.8.2) for visualization and intersection of the network models. SPSS 17.0 using the Wilcoxon Mann-Whitney test for windows was used for the statistical analysis.
Results
Urine Metabolic Phenotypes of GC
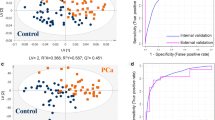
LC-MS system allows us to investigate all the processes of metabolites in healthy or diseased samples. A full-scan detection of urine metabolites was carried out by LC-MS, which involves discovering principal components that account for the majority of the differences in the data. Recently, unsupervised PCA is frequently used as a multivariate analysis in metabolomics studies to separate or determine the classes of known samples. For global profiling, PCA was performed to separate the disease and control groups. As shown in Figs. 1 and 2, we observed that PCA scores plot showed clear separation between the GC groups and healthy group in both positive (Fig. 1a) and negative ion modes (Fig. 2a).

Establishment of the metabolomic profiling of human gastric cancer patient and matched healthy control in positive ionization mode by using UPLC-MS system. PCA model results in positive mode (a). The PCA scores plot showed the different samples were scattered into two different regions. The normal group tended to cluster to the right region, while the GC group generally clustered to the left area. Loading plot of OPLS-DA of gastric cancer in positive mode (b). cThe combination of S- and VIP-score plots constructed from the supervised OPLS analysis of urine (ESI+ mode)

Metabolomic profiling of gastric cancer patient and matched healthy control in negative ionization mode. PCA model results in negative mode (a). PCA model demonstrated satisfactory modeling and achieved a fairly distinct separation between the metabolite profiles of the two groups. Loading plot of OPLS-DA of gastric cancer (b). cThe combination of S- and VIP-score plots constructed from the supervised OPLS analysis of urine (ESI− mode)
Discriminatory Markers Highlighted in Urine of GC Patients
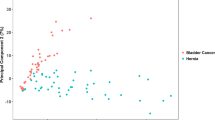
From the corresponding loading plots, the ions furthest away from the origin may be therefore regarded as the differentiating metabolites (Figs. 1b and 2b). The integration areas of the detected metabolites with high VIP values were first tested for the normality of the distribution. VIP plots from the OPLS analysis (Figs. 1c and 2c), LC-MS provided the retention time, precise molecular mass, and MS/MS data for the metabolites. For OPLS-DA, to identify which variables account for such a significant separation, VIP plot was initially used to preselect variables. As shown in Table 1, according to the criterion for VIP plot (VIP > 5.86) and p value below 0.05, among the low molecular weight endogenous metabolites, a total of 16 variables as displayed in Table 1 were obtained which contributed most toward discriminating the metabolic profiles between the two classes. Intriguingly, nine of the metabolites detected were found to be upregulated in GC, while seven were downregulated. Identification and statistic analysis revealed significant elevation of 2-oxoglutarate, alanine, citric acid, l-proline, malic acid, phenylacetylglycine, taurine, urea, and uric acid, while revealing significant reduction of succinic acid, glycocholic acid, glycine, hexadecanoic acid, hippurate, 4-deoxythreonic acid, and pyrimidine in GC. According to the identity check based on raw data and the features of peaks, the target masses of candidate metabolites identified in the profiling process were searched over a narrow ±5 ppm mass window in the HMDB and METLIN databases. Finally, potential biomarkers of significant contribution were listed in Table 1. Expression levels of marker metabolites altered in human GC subjects were also shown in Fig. 3.

Expression levels of marker metabolites altered in human gastric cancer subjects (1) and healthy controls (0)
Metabolic Pathway and Function Analysis
We observed that 2-oxoglutarate, alanine, citric acid, l-proline, malic acid, phenylacetylglycine, taurine, urea, and uric acid were at higher levels in the urine of GC group than those in control group. Furthermore, the decreased levels of succinic acid, glycocholic acid, glycine, hexadecanoic acid, hippurate, 4-deoxythreonic acid, and pyrimidine were found in the GC group as compared with the control group. The detailed analysis of the most relevant pathways of GC was performed by MetPA’s tool that is a mass translator into pathways. MetPA assigned a total of feature compounds in 30 pathways which were identified together are important for the host response to GC (Fig. 4a and Table S1). The main metabolic pathways associated with GC included citrate cycle (malic acid, succinic acid, 2-oxoglutarate, citric acid), cyanoamino acid metabolism (glycine, alanine), primary bile acid biosynthesis (glycine, taurine, glycocholic acid), arginine and proline metabolism (urea, l-proline), fatty acid metabolism (hexadecanoic acid), etc. The detailed construction of the predominant metabolism pathways of citrate cycle (Fig. 4b), taurine and hypotaurine metabolism (Fig. 4c), arginine and proline metabolism (Fig. 4d) did yield satisfactory results. These metabolic pathways of importance were disturbed in GC patients.

Construction of the altered metabolism pathways in human gastric cancer disease using MetPA analysis (a). The map was generated using the reference map by KEGG. CO represents entry number of compound. Citrate cycle (b); taurine and hypotaurine metabolism (c); arginine and proline metabolism (d)
Metabolic Network Visualization
In this study, we further characterized the expression patterns of human GC were compared by metabolomics analysis, and several important metabolic pathways associated with GC were identified. The metabolites and corresponding pathways were imported into Cytoscape for visualization of the network models. Altered metabolites from the merged dataset were mapped to KEGG reference pathways, and interaction networks were generated in Cytoscape. As seen in Fig. 5, association network of differentially expressed metabolites using Cytoscape was constructed. Modes of action are shown in different colors. It provides evidence that novel biomarkers are actively involved in multifunctional pathways, and these insights help us to better understand the mechanisms underlying GC. Our data suggest that this network clearly enhances the understanding molecular mechanisms of panel metabolite biomarkers.

Metabolites altered in gastric cancer subjects compared to healthy controls map to multiple biosynthetic pathways. Altered metabolites from the merged dataset were mapped to KEGG and SMPDB reference pathways, and interaction networks were generated in Cytoscape. The network nodes (green and red) represent pathways and related metabolites detected, respectively (details in Table S1)
Discussion
GC is the second most common cause of cancer-related deaths globally. Successful management of GC is hampered by lack of highly sensitive and specific biomarkers especially for early cancer detection. Although timely intervention is associated with better clinical outcome, early GC detection is frequently not possible given its asymptomatic nature. In view of this, there remains a need for more reliable noninvasive markers to decrease the need for GC. As such, sensitive and specific GC biomarkers are highly sought after as diagnostic surrogates that may replace invasive endoscopic and histological examinations. To address this gap, we performed a comparative study to clearly differentiate patients with GC from matched control subjects and identify the potential biomarkers using a combination of LC-MS-based urine metabolomics coupled with pattern recognition approach and network analysis. In this study, the TCA cycle intermediates such as malic acid, succinic acid, 2-oxoglutarate and citric acid were remarkably perturbed in GC, suggesting that enhanced glycolysis contributes to GC progression. With recent advances in metabolomics, biomarkers can now be identified by discovery strategies that are not limited by our existing biological knowledge. With this aim, we performed a pilot metabolomics study to assess this as a strategy for urine marker detection in patients suffering from GC.
Metabolomics is a post-genomic research field for analysis of low molecular weight compounds in biological systems [16, 17] and offers an analysis of metabolite level changes in biological samples. In recent years, it has been used in various diseases such as renal cancer, brain tumors, colorectal cancer, and lung cancer [18–20]. We expected that the potential metabolic biomarkers could be found for early diagnosis and screening of GC. To elucidate the underlying mechanisms of GC on global metabolic pathways, a total of 16 metabolites that were differentially regulated were detected. Nine metabolites were significantly increased, and seven metabolites decreased relative to control. It revealed significant elevation of 2-oxoglutarate, alanine, citric acid, l-proline, malic acid, phenylacetylglycine, taurine, urea, and uric acid, while revealing significant reduction of succinic acid, glycocholic acid, glycine, hexadecanoic acid, hippurate, 4-deoxythreonic acid, and pyrimidine in GC. Based on the findings of this study, it would appear that many different metabolic pathways are disrupted in response to GC, most notably included citrate cycle (2-oxoglutarate, malic acid, succinic acid, citric acid), cyanoamino acid metabolism (glycine, alanine), primary bile acid biosynthesis (glycine, taurine, glycocholic acid), arginine and proline metabolism (urea, l-proline), fatty acid metabolism (hexadecanoic acid), etc. Association network of differentially expressed metabolites using Cytoscape was constructed. It provides evidence that novel biomarkers are actively involved in multifunctional pathways, and these insights help us to better understand the mechanisms underlying GC, clearly enhances the understanding molecular mechanisms of panel metabolite biomarkers and several important metabolic pathways.
Wu and co-workers used the metabolomics method to study the gastric cancer patients [21]. Results showed that 18 metabolites were detected differently between the malignant tissues and the normal. Six of 18 metabolites including alanine, glycine, l-proline, malic acid, pyrimidine, and urea were consistent with our results. Consistent with a recent report that metabolites were significantly changed in GC [22], we also found alanine, glycine, urea, l-proline, citric acid, and uric acid as biomarker candidates. Biomarkers-associated GC had been identified by metabolic profiling, and diagnostic models for gastric cancer were constructed using OPLS-DA [23]. Eleven metabolites were identified and potentially revealed perturbations of glycolysis and of amino acid, fatty acid, cholesterol, and nucleotide metabolism of gastric cancer patients. Among which four metabolites such as alanine, hexadecanoic acid, l-proline, and glycine were consistent with our results.
Research on molecular mechanisms of GC plays an important role in diagnosing and treating gastric cancer was also discussed. Based on these results, we further analyzed the metabolites involved in GC, and the significantly changed metabolites have been found and used to explain the metabolic molecular mechanism. 2-oxoglutarate is a key intermediate in the Krebs cycle and an important nitrogen transporter in the metabolic pathways in biological processes. Succinic acid, a dicarboxylic acid, is a component of the citric acid cycle capable of donating electrons to the electron transfer chain. Succinate dehydrogenase plays an important role in the mitochondria, being both part of the respiratory chain and the Krebs cycle. Citric acid (citrate) is a weak acid that is formed in the tricarboxylic acid cycle. The urinary citrate excretion is a common tool in the differential diagnosis of kidney diseases [24]. The key regulatory enzymes directly associated with citrate production in the prostate cells are mitochondrial aspartate aminotransferase, pyruvate dehydrogenase, and mitochondrial aconitase. Malic acid, tart-tasting organic dicarboxylic acid, in its ionized form is malate, an intermediate of the TCA cycle along with fumarate. It can also be formed from pyruvate as one of the anaplerotic reactions. Glycocholic acid is an acyl glycine and a bile acid glycine conjugate. It is a secondary bile acid produced by the action of enzymes existing in the microbial flora of the colonic environment. More specifically, glycocholic acid, or cholylglycine, is a crystalline bile acid involved in the emulsification of fats. It occurs as a sodium salt in the bile of mammals. As the glycine conjugate of cholic acid, this compound acts as a detergent to solubilize fats for absorption and is itself absorbed. Taurine is a sulfur amino acid like methionine, cystine, cysteine, and homocysteine. Taurine has many diverse biological functions serving as a neurotransmitter in the brain, a stabilizer of cell membranes and a facilitator in the transport of ions such as sodium, potassium, calcium, and magnesium. Taurine, after GABA, is the second most important inhibitory neurotransmitter in the brain. Its inhibitory effect is one source of taurine’s anticonvulsant and antianxiety properties. Taurine has many important metabolic roles. Taurine increases bilirubin and cholesterol excretion in the bile and is critical to normal gallbladder function. It seems to inhibit the effect of morphine and potentiates the effects of opiate antagonists. Urea is a highly soluble organic compound formed in the liver from ammonia produced by the deamination of amino acids. It is the principal end product of protein catabolism and constitutes about one half of the total urinary solids. Urea is formed in a cyclic pathway known simply as the urea cycle. l-Proline is one of the 20 amino acids used in living organisms as the building blocks of proteins. It is an essential component of collagen and is important for proper functioning of joints and tendons. Alanine is a nonessential amino acid made in the body from the conversion of the carbohydrate pyruvate or the breakdown of DNA and the dipeptides carnosine and anserine. It is highly concentrated in muscle and is one of the most important amino acids released by muscle, functioning as a major energy source. Alanine is an important participant as well as regulator in glucose metabolism. Alanine, like GABA, taurine, and glycine, is an inhibitory neurotransmitter in the brain. Hexadecanoic acid is a hydroxylated fatty acid where the terminal carbon has been hydroxylated. Hippuric acid is an acyl glycine formed by the conjugation of benzoic acid with glycine. Hippuric acid is the most frequently used biomarker in the biological monitoring of occupational exposure to toluene. This product of solvent biotransformation may be also found in the urine of individuals who have not been exposed to the solvent. 4-Deoxythreonic acid is a normally occurring carboxylic acid in human. Metabolic profiling of urinary organic acids from patients with juvenile-onset diabetes mellitus has revealed significantly elevated levels of 4-deoxythreonic acid. Uric acid is a heterocyclic purine derivative that is the final oxidation product of purine metabolism. It is produced by the enzyme xanthine oxidase, which oxidizes oxypurines such as xanthine into uric acid. Phenylacetylglycine is an acyl glycine. Acyl glycines are normally minor metabolites of fatty acids. In certain cases, the measurement of these metabolites in body fluids can be used to diagnose disorders associated with mitochondrial fatty acid beta-oxidation. Pyrimidines serve essential functions in human metabolism as ribonucleotide bases in RNA (uracil and cytosine), and as deoxyribonucleotide bases in DNA (cytosine and thymine), and are linked by phosphodiester bridges to purine nucleotides in double-stranded DNA in both the nucleus and the mitochondria. Pyrimidine activated sugars are also involved in polysaccharide and phospholipid synthesis, glucuronidation in detoxification processes, and glycosylation of proteins and lipids.
In summary, LC-MS was used as a high-throughput screening platform for characterizing dynamic metabolomic responses to GC. PCA model derived from UPLC/MS urine metabolomics showed satisfactory and adequate separations between the GC and non-GC cohorts, indicating the diagnostic potential of UPLC/MS metabolic fingerprinting. Interestingly, 16 distinct metabolites were identified in GC subjects compared to controls, many are in various stages of progress at the GC and suggest a disrupted citrate cycle (malic acid, succinic acid, 2-oxoglutarate, citric acid), cyanoamino acid metabolism (glycine, alanine), primary bile acid biosynthesis (glycine, taurine, glycocholic acid), arginine and proline metabolism (urea, l-proline), fatty acid metabolism (hexadecanoic acid), etc. Differential metabolites identified from the metabolomics analysis would be helpful for the prevention and treatment, occurrence, and development of GC. More importantly, 30 metabolism pathways found that the most altered functional pathway is associated with GC. Mapping altered metabolites to KEGG pathways identified alterations in a variety of biological processes mediated through complex networks. In this study, we have given an illustrative example how to build, visualize, and analyze the metabolism pathway network, when working with high-throughput metabolic data. Key limitations of this study include that it did not examine large-scale study training to validate prognostic markers for GC.
Conclusions
Metabolomics using mass spectrometry has been used to profile many diseases. In this study, we focused on small-molecule metabolites to investigate the characteristics of GC. It revealed 16 metabolite markers have been selected, which constructed a diagnostic approach for distinguishing the GC and controls. Moreover, these marker metabolites were worth investigating in the future. Further functional and clinical sample analysis of the metabolic pathways is needed to demonstrate their role in GC. The metabolic pathways may be exploited as biomarkers for GC progression. These results suggest that urine metabolic profiles have great potential in detecting GC and may aid in understanding its underlying mechanisms. A preliminary interpretation of these results indicates that the strategy described in this study can be proposed as a general tool to facilitate biomarker identification and to understand the pathogenesis of Alzheimer’s disease.
References
Hou, Q., Tan, H. T., Lim, K. H., Lim, T. K., Khoo, A., Tan, I. B., Yeoh, K. G., & Chung, M. C. (2013). Identification and functional validation of caldesmon as a potential gastric cancer metastasis-associated protein. Journal of Proteome Research, 12(2), 980–990.
Aquino, P. F., Fischer, J. S., Neves-Ferreira, A. G., Perales, J., Domont, G. B., Araujo, G. D., Barbosa, V. C., Viana, J., Chalub, S. R., Lima de Souza, A. Q., Carvalho, M. G., Leão de Souza, A. D., & Carvalho, P. C. (2012). Are gastric cancer resection margin proteomic profiles more similar to those from controls or tumors? Journal of Proteome Research, 11(12), 5836–5842.
Courant, F., Antignac, J. P., Monteau, F., & Le Bizec, B. (2013). Metabolomics as a potential new approach for investigating human reproductive disorders. Journal of Proteome Research, 12(6), 2914–2920.
Blazquez, M., Carretero, A., Ellis, J. K., Athersuch, T. J., Cavill, R., Ebbels, T. M., Keun, H. C., Castell, J. V., Lahoz, A., & Bort, R. (2013). A combination of transcriptomics and metabolomics uncovers enhanced bile acid biosynthesis in HepG2 cells expressing CCAAT/enhancer-binding protein β (C/EBPβ), hepatocyte nuclear factor 4α (HNF4α), and constitutive androstane receptor (CAR). Journal of Proteome Research, 12(6), 2732–2741.
Manna, S. K., Krausz, K. W., Bonzo, J. A., Idle, J. R., & Gonzalez, F. J. (2013). Metabolomics reveals aging-associated attenuation of noninvasive radiation biomarkers in mice: potential role of polyamine catabolism and incoherent DNA damage-repair. Journal of Proteome Research, 12(5), 2269–2281.
Hu, J. D., Tang, H. Q., Zhang, Q., Fan, J., Hong, J., Gu, J. Z., & Chen, J. L. (2011). Prediction of gastric cancer metastasis through urinary metabolomic investigation using GC/MS. World Journal of Gastroenterology, 17(6), 727–734.
Wang, X., Zhang, A., Han, Y., Wang, P., Sun, H., Song, G., Dong, T., Yuan, Y., Yuan, X., Zhang, M., Xie, N., Zhang, H., Dong, H., & Dong, W. (2012). Urine metabolomics analysis for biomarker discovery and detection of jaundice syndrome in patients with liver disease. Molecular & Cellular Proteomics, 11(8), 370–380.
Zhang, A., Sun, H., Han, Y., Yuan, Y., Wang, P., Song, G., Yuan, X., Zhang, M., Xie, N., & Wang, X. (2012). Exploratory urinary metabolic biomarkers and pathways using UPLC-Q-TOF-HDMS coupled with pattern recognition approach. Analyst, 137(18), 4200–4208.
Wang, X., Wang, H., Zhang, A., Lu, X., Sun, H., Dong, H., & Wang, P. (2012). Metabolomics study on the toxicity of aconite root and its processed products using ultraperformance liquid-chromatography/electrospray-ionization synapt high-definition mass spectrometry coupled with pattern recognition approach and ingenuity pathways analysis. Journal of Proteome Research, 11(2), 1284–1301.
Sun, H., Ni, B., Zhang, A., Wang, M., Dong, H., & Wang, X. (2012). Metabolomics study on fuzi and its processed products using ultra-performance liquid-chromatography/electrospray-ionization synapt high-definition mass spectrometry coupled with pattern recognition analysis. Analyst, 137(1), 170–185.
Wu, W.,, & Chung, M. C. (2013). The gastric fluid proteome as a potential source of gastric cancer biomarkers. Journal of Proteomics.
Wang, X., Yang, B., Sun, H., & Zhang, A. (2012). Pattern recognition approaches and computational systems tools for ultra performance liquid chromatography-mass spectrometry-based comprehensive metabolomic profiling and pathways analysis of biological data sets. Analytical Chemistry, 84(1), 428–439.
Yang, B., Zhang, A., Sun, H., Dong, W., Yan, G., Li, T., & Wang, X. (2012). Metabolomic study of insomnia and intervention effects of suanzaoren decoction using ultra-performance liquid-chromatography/electrospray-ionization synapt high-definition mass spectrometry. Journal of Pharmaceutical and Biomedical Analysis, 58, 113–124.
Zhang, A., Sun, H., Wang, P., Han, Y., & Wang, X. (2012). Modern analytical techniques in metabolomics analysis. Analyst, 137(2), 293–300.
Dong, H., Zhang, A., Sun, H., Wang, H., Lu, X., Wang, M., Ni, B., & Wang, X. (2012). Ingenuity pathways analysis of urine metabolomics phenotypes toxicity of Chuanwu in Wistar rats by UPLC-Q-TOF-HDMS coupled with pattern recognition methods. Molecular BioSystems, 8(4), 1206–1221.
Zhang, A., Sun, H., Wang, P., Han, Y., & Wang, X. (2012). Recent and potential developments of biofluid analyses in metabolomics. Journal of Proteomics, 75(4), 1079–1088.
Wang, X., Sun, H., Zhang, A., Sun, W., Wang, P., & Wang, Z. (2011). Potential role of metabolomics approaches in the area of traditional Chinese medicine: as pillars of the bridge between Chinese and Western medicine. Journal of Pharmaceutical and Biomedical Analysis, 55(5), 859–868.
Wei, J., Xie, G., Ge, S., Qiu, Y., Liu, W., Lu, A., Chen, T., Li, H., Zhou, Z., & Jia, W. (2012). Metabolic transformation of DMBA-induced carcinogenesis and inhibitory effect of salvianolic acid b and breviscapine treatment. Journal of Proteome Research, 11(2), 1302–1316.
Zhang, A. H., Sun, H., Han, Y., Yan, G. L., Yuan, Y., Song, G. C., Yuan, X. X., Xie, N., & Wang, X. J. (2013). Ultraperformance liquid chromatography-mass spectrometry based comprehensive metabolomics combined with pattern recognition and network analysis methods for characterization of metabolites and metabolic pathways from biological data sets. Analytical Chemistry, 85, 7606–7612.
Zhang, A., Zhou, X., Zhao, H., Guan, Y., Zhou, S., Yan, G. L., Ma, Z., Liu, Q., & Wang, X. (2014). Rapidly improved determination of metabolites from biological data sets using the high-efficient TransOmics tool. Molecular BioSystems, 10, 160–165.
Wu, H., Xue, R., Tang, Z., Deng, C., Liu, T., Zeng, H., Sun, Y., & Shen, X. (2010). Metabolomic investigation of gastric cancer tissue using gas chromatography/mass spectrometry. Analytical and Bioanalytical Chemistry, 396(4), 1385–1395.
Ikeda, A., Nishiumi, S., Shinohara, M., Yoshie, T., Hatano, N., Okuno, T., Bamba, T., Fukusaki, E., Takenawa, T., Azuma, T., & Yoshida, M. (2012). Serum metabolomics as a novel diagnostic approach for gastrointestinal cancer. Biomedical Chromatography, 26(5), 548–558.
Song, H., Peng, J. S., Dong-Sheng, Y., Yang, Z. L., Liu, H. L., Zeng, Y. K., Shi, X. P., & Lu, B. Y. (2012). Serum metabolic profiling of human gastric cancer based on gas chromatography/mass spectrometry. Brazilian Journal of Medical and Biological Research, 45(1), 78–85.
Posada-Ayala, M., Zubiri, I., Martin-Lorenzo, M., Sanz-Maroto, A., Molero, D., Gonzalez-Calero, L., Fernandez-Fernandez, B., de la Cuesta, F., Laborde, C. M., Barderas, M. G., Ortiz, A., Vivanco, F., & Alvarez-Llamas, G. (2014). Identification of a urine metabolomic signature in patients with advanced-stage chronic kidney disease. Kidney International, 85, 103–111.
Acknowledgments
This work was supported by grants from the Key Program of Natural Science Foundation of State (Grant No. 81470196). The authors also thank BGI for the excellent technical assistance and are specifically grateful to Pro Aihua Zhang for many helpful discussions and suggestions.
Conflict of Interest
The authors declare that they have no competing interests.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOC 79 kb)
Rights and permissions
About this article

Cite this article
Liang, Q., Wang, C. & Li, B. Metabolomic Analysis Using Liquid Chromatography/Mass Spectrometry for Gastric Cancer. Appl Biochem Biotechnol 176, 2170–2184 (2015). https://doi.org/10.1007/s12010-015-1706-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12010-015-1706-z