
Abstract
Background
Increasing national expenditures and use associated with TKA have resulted in pressure to reduce costs through various reimbursement cuts. However, within the arthroplasty literature, few studies have examined the association of medical comorbidities on resource use and length of stay after joint arthroplasty.
Questions/purposes
The purpose of this study was to examine the association between individual patient characteristics (including demographic factors and medical comorbidities) on resource allocation and length of stay (LOS) after TKA.
Methods
We queried the 2009 Nationwide Inpatient Sample dataset for International Classification of Diseases, 9th Revision code, 81.54, for TKAs. An initial 621,029-patient cohort was narrowed to 516,745 after inclusion of elective TKAs on patients aged between 40 and 95 years. Using generalized linear models, we estimated the effect of comorbidities on resource use (using cost-to-charge conversions to estimate hospital costs) and the LOS controlling for patient and hospital characteristics. Across the 2009 national cohort with TKAs, 12.7% had no comorbidities, whereas 32.6% had three or more. The most common conditions included hypertension (67.8%), diabetes (20.0%), and obesity (19.8%). Mean hospital costs were USD 14,491 (95% confidence interval [CI], 14,455–14,525) and mean hospital LOS was 3.3 days (95% CI, 3.29–3.31) in this data set.
Results
Patients with multiple comorbidities were associated with increased resource use and LOS. Higher marginal costs and LOS were associated with patients who had an inpatient death (USD +8017 [95% CI, 8006–8028], +2.3 [CI, 2.15–2.44] days over baseline), patients with recent weight loss (USD +4587 [95% CI, 4581–4593], +1.5 [CI, 1.45–1.61) days], minority race (USD +1037 [95% CI, 1035–1038], +0.3 [CI, 0.28–0.33] days), pulmonary-circulatory disorders (USD +3218 [95% CI, 3214–3221], +1.3 [CI, 1.25–1.34] days), and electrolyte disturbances (USD +1313 [95% CI, 1312–1314], +0.6 [CI, 0.57–0.60] days). All p values were < 0.001.
Conclusion
Multiple patient comorbidities were associated with additive resource use and LOS after TKA. Current reimbursement may not adequately account for these patient characteristics. To avoid potential loss of access to care for sicker patients, payment needs to be adjusted to reflect actual resource use.
Level of Evidence
Level IV, economic and decision analysis. See the Instructions for Authors for a complete description of levels of evidence.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
TKA is a highly effective procedure and is widely used. Over 600,000 TKAs are performed yearly in the United States, and this number is expected to rise dramatically in the next several decades [11, 20]. However, TKA requires substantial investment of effort and expense, and there are major concerns about future economic sustainability.
Medicare hospital payments for primary TKA remain relatively fixed with a US average around USD 13,400 [21]. However, this level of reimbursement often fails to cover the cost of care. Historically, this concern has been most relevant to revision arthroplasty, for which Medicare reimbursed at the same level despite well-established differences in resource use [4]. The influence of individual patient factors on hospital costs has been less understood. Within the trauma literature, several studies have demonstrated greater hospital costs in the comorbid patient after hip fracture [6, 25]. Nikkel et al. [25] found that malnutrition and pulmonary-circulatory disorders had the largest individual effects on hospital costs after hip fracture and that the presence of multiple comorbidities had a compounding effect on costs and hospital length of stay (LOS). Similarly, Chen et al. [6] separately reported that the presence of multiple medical comorbidities, especially dementia, increased hospitalization costs for hip fractures. Within the arthroplasty literature, however, few studies have examined the impact of chronic medical disease on hospital costs [29].
We therefore sought to determine the influence of individual patient medical comorbidities and characteristics on resource use (as estimated by cost-to-charge ratios) and LOS with an emphasis on patients covered by Medicare. Our specific purpose was to examine the association between individual patient characteristics (including demographic factors and medical comorbidities) on resource allocation and LOS after TKA.
Patients and Methods
The 2009 Nationwide Inpatient Sample (NIS) data set was queried for all patients undergoing TKA. The NIS is the largest national all-payer database for inpatient hospital stays [14]. The NIS collects a 20% sample of deidentified patient information from discharges at the state and national levels that can be extrapolated to represent national estimates. As of 2009, the NIS captured data from 1050 hospitals located in 45 states, covering 96% of the US population and encompassing approximately eight million discharges annually. More than 100 variables are collected for each inpatient stay, encompassing patient demographic, medical comorbidities, morbidity outcomes, hospital characteristics, and financial information.
Using International Disease Classification, 9th Revision, Clinical Modification (ICD-9-CM) procedural code, 81.54, we queried the 2009 NIS data set for all patients undergoing a unilateral TKA. Only elective surgeries in patients between 40 and 95 years old were considered. Database-specific variables were used to exclude inpatient transfers, emergency department admissions, or patients undergoing nonelective surgery, bilateral TKA, or other secondary procedures. In total, 14,130 patients were excluded.
Patient and hospital characteristics were extracted directly from the NIS database. These included patient age, sex, race, income level, and discharge location. Patient comorbidities were identified and directly extracted from the NIS by applying algorithms developed by Elixhauser et al. [12]. All comorbidities were present preoperatively and defined dichotomously directly from the database. Inpatient hospital charges and LOS were assessed directly from the database files. Because direct measurement of hospital costs are impractical across the numbers of centers sampled by the NIS, the Healthcare Cost and Utilization A8 Project (HCUP) uses a formula to convert hospital charges to estimated costs. This likely does not provide a precise dollar-value measurement of true cost, but serves as an estimate of resource use that can be compared across sites and geographic regions. Accordingly, resource use was estimated using HCUP cost-to-charge ratio files. These files contain detailed all-payer inpatient cost and charge information that each hospital provides to CMS. The results are internally validated for consistency annually. Charges reported represent inpatient hospital charges only; charges for skilled nursing facility or rehabilitation care after discharge are not included. Hospital LOS was extracted directly from the database and defined discretely as time from postoperative admission to discharge.
In the 2009 NIS there were 102,446 unique patient records, which extrapolated to 516,745 patients undergoing TKA in the United States after exclusion. Mean hospital costs were USD 14,491 (95% confidence interval [CI], 14,455–14,525) and mean hospital LOS was 3.3 days (95% CI, 3.29–3.31). Patient demographics were analyzed categorically (Table 1). Most patients were between 60 and 79 years old (63.6%) followed by 26.1% between 40 and 59 years, and 10.3% between 80 and 95 years. Overall, 63.2% of patients were women. In the cohort, 83.8% of patients were white, 6.5% were black, 5.1% were Hispanic, and 4.6% were other. Patient income level was split nearly evenly between the quartiles of USD 0 to 25,000, 25,000 to 50,000, 50,000 to 75,000, and 75 to 100,000+ per year.
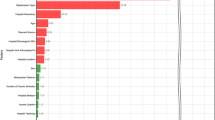
An aggregate analysis of the population cohort revealed that the most common conditions included hypertension (67.8%), diabetes (20.0%), and obesity (19.8%). Other notable comorbidities included chronic renal disease at 14.7%, depression at 11.8%, and electrolyte disturbances at 7.7%. Less common diseases including AIDS (0.02%), metastatic cancer (0.05%), and alcoholism (0.4%) also were present (Fig. 1). The number of comorbidities present in each patient was summed and only 12.7% of patients undergoing TKAs had no comorbidities, whereas 32.6% had three or more and 6% had five or more (Fig. 2).

The frequency of medical comorbidities among patients undergoing TKA is shown.

The number of individual medical comorbidities among individual patients is shown.
Separately, hospital cost and LOS estimates were fit to multivariate generalized linear models, assuming Poisson distribution and a log link function owing to plot skewness. This allowed us to estimate the marginal impact of the comorbidities on resource use and LOS while simultaneously adjusting for patient and hospital characteristics in these models. The reference patient in the models had the following personal/hospital characteristics: no comorbidity, 40 to 59 years old, white race, female with median household income quartiles 2 or 3, surgery performed at a northeast urban nonteaching medium bed size hospital, and then followed routine discharge. A Pearson correlation was assessed between hospital cost and LOS.
All data were analyzed using SAS Version 9.3 (SAS Institute, Cary, NC, USA). A p value < 0.05 was considered statistically significant.
Results
Resource Use
Patient age had a minor effect on resource use. When compared with the youngest group, patients 60 to 79 years and 80 to 95 years were associated with lower resource use (USD 350; 95% CI, 350–351; p < 0.01). Women incurred slightly lower costs (USD −193; 95% CI, 192–194; p < 0.01). Relative to white race, patients with Hispanic ethnicity (USD +1037; 95% CI, 1035–1038; p < 0.01) and black race (USD +996; 95% CI: 994–998; p < 0.01) were associated with higher costs. Income level did not consistently influence costs. Overall, higher hospital resource use did not necessarily correlate with hospital LOS; the Pearson correlation coefficient was 0.38.
Individual comorbidities were associated with increased hospital use (Appendix 1 [Supplemental material is available with the online version of CORR®.]).
Some of the conditions that had a higher marginal cost included: recent weight loss (USD +4587; 95% CI, 4581–4593; p < 0.01); pulmonary-circulatory disorders (USD +3218; 95% CI, 3214–3221; p < 0.01); AIDS (USD +2305; 95% CI, 2278–2332; p < 0.01); chronic heart failure (CHF) (USD +1656; 95% CI, 1654–1659; p < 0.01); coagulation disorders (USD +1598; 95% CI, 1596–1601; p < 0.01); and electrolyte disturbances (USD +1313; 95% CI, 1312–1314; p < 0.01). In-hospital mortality was associated with increased resource use (USD +8017; 95% CI, 8006–8028; p < 0.01) (Appendix 1). Patient disposition also influenced costs. In comparison to patients who had routine discharges, patients going to skilled nursing facilities, rehabilitation units, and receiving home health were associated with greater costs (USD 738; 95% CI, 737–739; p < 0.01).
The more comorbidities a patient had, the greater resource use. On average, the addition of each medical problem was associated higher inpatient costs (Fig. 3). For example, a patient with no comorbidities had a TKA with a cost of USD 13,768; a patient with three comorbidities with a cost of USD 14,185; and a patient with seven comorbidities with a cost of USD 17,765 (p < 0.01).

The incremental effect of each additional patient comorbidity on hospital resource use after TKA is shown. Line bars indicate 5th and 95th percentiles; colored box represents 25th and 75th percentile, horizontal line represents median, and asterisks are the mean cost.
Length of Stay
Patient age also had minimal effect on hospital LOS. When compared with the youngest group, patients 60 to 79 years and 80 to 95 years had a LOS that was longer (0.06 [95% CI, 0.05–0.08] and 0.2 days [95% CI, 0.17–0.21], p < 0.01). Hispanic ethnicity (+0.3 days; 95% CI, 0.28–0.33; p < 0.01) and black race (+0.2 days; 95% CI, 0.21–0.26; p < 0.01) were associated with longer LOS. Income level and gender also did not consistently influence LOS.
Individual comorbidities were associated with a higher LOS (Appendix 2 [Supplemental material is available with the online version of CORR®.]). The marginal effect on LOS of some common conditions included: recent weight loss (+1.53 days; 95% CI, 1.45–1.61; p < 0.01); pulmonary-circulatory disorders (+1.3 days; 95% CI, 1.25–1.34; p < 0.01); CHF (+0.6 days; p < 0.01); coagulation disorders (+0.4 days; p < 0.01); and electrolyte disturbances (+0.58 days; 95% CI, 0.57–0.60; p < 0.01). In-hospital mortality was associated with an increased LOS of 2.3 days (95% CI, 2.15–2.44; p < 0.01) (Appendix 2). Patient disposition also influenced LOS. In comparison to patients who had routine discharges, patients going to skilled nursing facilities, rehabilitation units, and receiving home health, had longer LOS (+0.40 days; 95% CI, 0.39–0.42; p < 0.01). Multiple comorbidities were associated with higher LOS. On average, the addition of each medical problem generated longer LOS (Fig. 4). For example, a patient with no comorbidities had a LOS of 2.9 days; a patient with three comorbidities had a LOS of 3.2 days; and a patient with seven comorbidities LOS of 4.7 days (p < 0.01).

The incremental effect of each additional patient comorbidities on hospital LOS after TKA is shown. Line bars indicate 5th and 95th percentiles, colored box represents 25th and 75th percentile, horizontal line represents median, and asterisks are the mean LOS.
Discussion
TKA represents a highly used and expensive intervention, and the number of procedures performed is expected to increase substantially in the next decades. However, current hospital reimbursement may not accurately reflect the cost of caring for patients undergoing TKA with chronic medical disease and diverse socioeconomic backgrounds. Few studies have evaluated the effect of patient comorbidities on hospital costs and LOS in the setting of TKA [25]. In this review of the 2009 NIS database, we found that over 85% of patients undergoing TKA in the United States had at least one comorbidity and that increasing numbers of medical comorbidities were associated with incremental increases in hospital resource use and LOS. Race, sex, and hospital characteristics also affected hospital costs and LOS.
Our study has some important limitations. Many of these limitations relate to the NIS database. Cost-to-charge ratios provide information about resource use but do not give sound estimates of actual dollar cost. For that, direct measurement is required but impractical in a survey this large. Readers should understand this major limitation of cost-to-charge ratios. In the same vein, data collection in the NIS database ends with inpatient discharge, but the cost of care during the postdischarge period is considerable and is not considered in analysis of NIS data. Thus, the true associated cost of medical comorbidities during the perioperative period may be underestimated. Additionally, our findings are associations rather than causations. The identified comorbidities did not necessarily cause higher cost or LOS but instead were associated with increased resource use or LOS. Also, the NIS is a stratified, 20% sample. Although the database maintains that the NIS is a representative sample, extrapolating rare events or comorbidities to the entire population may not truly represent prevalence. Finally, all patient data are extracted from discharge administrative claims data. It is possible that miscoding of the claims data may result in an inaccurate representation of the true morbidity burden [10]. Despite these limitations, we believe our findings give readers important information to start understanding the drivers of cost and LOS after TKA.
Our results indicate a high disease burden among patients undergoing TKA with at least 85% of patients having at least one comorbidity and 32.5% having three or more. Prior studies have demonstrated increased surgical risk in the patient with multiple comorbidities [27]. According to our findings, hospital costs and LOS after TKA rise with multiple patient comorbidities (Figs. 3, 4). Although each comorbidity has a unique association with resource use in our study and LOS, their combination is additive in our statistical models. The influence of multiple conditions on TKA inpatient costs has not been previously well described, although the influence of specific medical comorbidities on hospital resource consumption has been previously been reported in other medical conditions [25, 30]. Our findings allow for quantification of this effect. The five most costly comorbidities included recent weight loss (USD +4587), pulmonary-circulatory disease (USD +3218), AIDS (USD +2278), CHF (USD +1656), and coagulopathy (USD +1598). The most common comorbidities, obesity and diabetes, increased inpatient costs USD 390 and USD 212 to USD 775, respectively. These findings corroborate a recent Mayo Clinic study that found obesity (and every five-unit BMI increase over 30 kg/m2) increased hospital costs USD 500 and 90-day costs by USD 900 after THA [23]. Furthermore, the most costly comorbidities have been previously implicated as independent risk factors for complication after arthroplasty [3, 16, 22, 26]. The cause of higher costs in these multiply comorbid patients is likely multifactorial.
Prolonged hospital LOS can have detrimental effects on hospital resource consumption after elective arthroplasty. This may explain the dramatic decline in LOS after TKA over the last two decades [11, 18]. Our results demonstrate that recent weight loss (+1.5 days), pulmonary-circulatory disease (+1.3 days), and CHF (+0.6 days) all were associated with prolonged hospital LOS. These findings are consistent with previous studies that have implicated elevated American Society of Anesthesiologists class and significant medical disease in higher LOS [9, 13].
Other factors, that we could not quantify with the NIS, including aggressive use of blood transfusion and prolonged operative time, have also been associated with prolonged LOS [24]. Additionally, our findings of a low to moderate correlation between costs and LOS suggest that other more significant, yet unmeasurable drivers of cost may exist. Increasing implant costs have been recognized as one of the most significant contributors to hospital costs [15, 19, 28], and their variability has been well established. Ultimately, the interplay among costs, LOS, and new CMS initiatives to reduce readmissions remains complex and will continue to evolve.
According to our findings, hospital costs and LOS after TKA increase with multiple patient comorbidities (Figs. 3, 4). Although each comorbidity has a unique effect on costs and LOS, their combination is additive in our statistical models. The effect of multiple conditions on TKA inpatient costs has not been well described [25]. Many insurance reimbursement schemes allow for only a fixed payment upgrade whether a patient has one or several qualifying comorbidities or complications. In the Medicare system, these qualifiers are called CCs (Complications and Comorbid Conditions) and MCCs (Major CCs). In the current Medicare reimbursement strategies, hospitals are paid for a TKA based on relatively fixed (but regionally variable) diagnosis-related groups. According to analysis of data from the CMS, that number was approximately USD 13,400 in 2009 [21]. Hospitals can collect more by coding a complication or comorbid condition or major complication or comorbid condition, which may add up to 40% to the base payment (major comorbid condition or complication). Although hundreds of comorbidities are considered complications and major complications, the coding rules are complex and change often [8]. Some major complications and comorbid conditions coded at our hospital include AIDS, severe malnutrition, acute CHF exacerbation, cardiac arrest, and pulmonary embolism. Some common comorbid conditions and complications include dementia, CHF, obesity (BMI > 40 kg/m2), paraplegia, malnutrition, and venous thrombosis. Our data indicate that for many conditions or complications, these additional payments fall short of that required to cover added costs. According to our data, a patient with a history of metastatic cancer, electrolyte disturbances, or cardiopulmonary disorders may incur additional costs exceeding the payment to perform the TKA. Medicare has additional mechanisms for hospitals to recoup large financial losses called outlier payments but these are used in less than 1% of primary TKAs [2, 8, 21]. As the payments for arthroplasty continue to decline, policymakers should attempt to provide fair adjustments to hospitals and surgeons treating the comorbid.
The association of race and socioeconomic status on complications and resource use has been previously explored [1, 18, 27]. Furthermore, several studies have described racial disparities in access to care and to patient outcomes [5, 31]. Socioeconomic status and race have been implicated as significant risk factors for readmission [1, 18]. Our results corroborate many of these prior findings. In their risk adjustment models, the Medicare Readmissions Reduction program and public reporting does not currently incorporate these proven disparity generators [1, 7, 17]. Given this suspected association between race/socioeconomic status and hospital resource use, policymakers should consider incorporating socioeconomic factors in risk-adjustment and reimbursement models.
In conclusion, evaluation of this portion of the NIS database demonstrated that increasing numbers of patient comorbidities were associated with compounding increases in resource use (estimated hospital costs) and hospital LOS in patients who underwent TKA in 2009. Current government reimbursement schemes may not adequately compensate hospitals for care of the patient with multiple chronic diseases, thus potentially placing access to care at risk.
References
Atkinson JG. Flaws in the Medicare readmission penalty. N Engl J Med. 2012;367:2056–2057.
Baser O, Fan Z, Dimick JB, Staiger DO, Birkmeyer JD. Outlier payments for cardiac surgery and hospital quality. Health Aff (Millwood). 2009;28:1154–1160.
Bozic KJ, Lau E, Kurtz S, Ong K, Rubash H, Vail TP, Berry DJ. Patient-related risk factors for periprosthetic joint infection and postoperative mortality following total hip arthroplasty in Medicare patients. J Bone Joint Surg Am. 2012;94:794–800.
Bozic KJ, Rubash HE, Sculco TP, Berry DJ. An analysis of medicare payment policy for total joint arthroplasty. J Arthroplasty. 2008;23:133–138.
Cai X, Cram P, Vaughan-Sarrazin M. Are African American patients more likely to receive a total knee arthroplasty in a low-quality hospital? Clin Orthop Relat Res. 2012;470:1185–1193.
Chen LT, Lee JA, Chua BS, Howe TS. Hip fractures in the elderly: the impact of comorbid illnesses on hospitalisation costs. Ann Acad Med Singapore. 2007;36:784–787.
CMS. CMS dry run hospital-specific report for hospital-wide all-cause unplanned readmission (HWR) Measure. 2012. Available at: www.cms.gov. Accessed October 1, 2013.
CMS. Acute Care hospital inpatient prospective payment system. Centers For Medicare and Medicaid Services. 2013. Available at: http://www.cms.gov/Medicare/Medicare-Fee-For-Service-Payment/AcuteInpatientPPS. Accessed October 1, 2013.
Collins TC, Daley J, Henderson WH, Khuri SF. Risk factors for prolonged length of stay after major elective surgery. Ann Surg. 1999;230:251–259.
Cram P, Ibrahim SA, Lu X, Wolf BR. Impact of alternative coding schemes on incidence rates of key complications after total hip arthroplasty: a risk-adjusted analysis of a national data set. GeriatriOrthop Surg Rehabil. 2012;3:17–26.
Cram P, Lu X, Kates SL, Singh JA, Li Y, Wolf BR. Total knee arthroplasty volume, utilization, and outcomes among Medicare beneficiaries, 1991–2010. JAMA. 2012;308:1227–1236.
Elixhauser A, Steiner C, Harris DR, Coffey RM. Comorbidity measures for use with administrative data. Med Care. 1998;36:8–27.
Gruskay JA, Fu MC, Bohl DD, Webb ML, Grauer JN. Factors affecting length of stay following elective posterior lumbar spine surgery: a multivariate analysis. Spine J. 2013 Nov 1. pii: S1529-9430(13)01617-3. doi: 10.1016/j.spinee.2013.10.022 [Epub ahead of print].
HCUP. Overview of the National Inpatient Sample (NIS). Agency for Healthcare Research and Quality. Available at: http://www.hcup-us.ahrq.gov/nisoverview.jsp. Accessed April 14, 2013.
Ho DM, Huo MH. Are critical pathways and implant standardization programs effective in reducing costs in total knee replacement operations? J Am Coll Surg. 2007;205:97–100.
Huang R, Greenky M, Kerr GJ, Austin MS, Parvizi J. The effect of malnutrition on patients undergoing elective joint arthroplasty. J Arthroplasty. 2013;28:21–24.
Joynt KE, Jha AK. Thirty-day readmissions—truth and consequences. N Engl J Med. 2012;366:1366–1369.
Joynt KE, Orav EJ, Jha AK. Thirty-day readmission rates for Medicare beneficiaries by race and site of care. JAMA. 2011;305:675–681.
Kelly MP, Bozic KJ. Cost drivers in total hip arthroplasty: effects of procedure volume and implant selling price. Am J Orthop (Belle Mead NJ). 2009;38:E1–4.
Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89:780–785.
Li Y, Lu X, Wolf BR, Callaghan JJ, Cram P. Variation of Medicare Payments for Total Knee Arthroplasty. J Arthroplasty. 2013;28:1513–1520.
Lin CA, Takemoto S, Kandemir U, Kuo AC. Mid-term outcomes in HIV-positive patients after primary total hip or knee arthroplasty. J Arthroplasty. 2014;29:277–282.
Maradit Kremers H, Visscher SL, Kremers WK, Naessens JM, Lewallen DG. Obesity increases length of stay and direct medical costs in total hip arthroplasty. Clin Orthop Relat Res. 2014;472:1232–1239.
Monsef JB, Della Valle AG, Mayman DJ, Marx RG, Ranawat AS, Boettner F. The impact of blood management on length of stay after primary total knee arthroplasty. Open Orthop J. 2014;8:108–113.
Nikkel LE, Fox EJ, Black KP, Davis C, Andersen L, Hollenbeak CS. Impact of comorbidities on hospitalization costs following hip fracture. J Bone Joint Surg Am. 2012;94:9–17.
Norian JM, Ries MD, Karp S, Hambleton J. Total knee arthroplasty in hemophilic arthropathy. J Bone Joint Surg Am. 2002;84:1138–1141.
Pugely AJ, Martin CT, Gao Y, Mendoza-Lattes S, Callaghan JJ. Differences in short-term complications between spinal and general anesthesia for primary total knee arthroplasty. J Bone Joint Surg Am. 2013;95:193–199.
Robinson JC, Pozen A, Tseng S, Bozic KJ. Variability in costs associated with total hip and knee replacement implants. J Bone Joint Surg Am. 2012;94:1693–1698.
Shah AN, Vail TP, Taylor D, Pietrobon R. Comorbid illness affects hospital costs related to hip arthroplasty: quantification of health status and implications for fair reimbursement and surgeon comparisons. J Arthroplasty. 2004;19:700–705.
Shwartz M, Iezzoni LI, Moskowitz MA, Ash AS, Sawitz E. The importance of comorbidities in explaining differences in patient costs. Med Care. 1996;34:767–782.
Singh JA, Lu X, Rosenthal GE, Ibrahim S, Cram P. Racial disparities in knee and hip total joint arthroplasty: an 18-year analysis of national Medicare data. Ann Rheum Dis. 2013 18 Sep [Epub ahead of print].
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she, or a member of his or her immediate family, has no funding or commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
The study examined inpatient admissions in 2009 using the National Inpatient Sample (NIS) Database, Healthcare Cost and Utilization Project (HCUP), Agency for Healthcare Research and Quality. The HCUP and the hospitals participating in the NIS Program are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved or waived approval for the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
Electronic supplementary material
Below is the link to the electronic supplementary material.
About this article

Cite this article
Pugely, A.J., Martin, C.T., Gao, Y. et al. Comorbidities in Patients Undergoing Total Knee Arthroplasty: Do They Influence Hospital Costs and Length of Stay?. Clin Orthop Relat Res 472, 3943–3950 (2014). https://doi.org/10.1007/s11999-014-3918-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-014-3918-x