
Abstract
Background
There are several treatment options for calcifying tendinitis of the shoulder. The next step treatment after conservative treatment fails is still a matter of dispute. Extracorporeal shock wave therapy (ESWT) has been shown to be a good alternative to surgery, but the best treatment intensity remains unknown. High-energy ESWT is much more painful, more expensive, and usually is done in an inpatient setting, whereas low-energy ESWT can be performed in an outpatient setting by a physical therapist.
Questions/purposes
A systematic review and meta-analysis of randomized trials was performed to answer two clear research questions: (1) Is there a greater increase in the Constant-Murley score in patients treated with high-energy ESWT compared with those treated with low-energy ESWT by 3 months and by 6 months? (2) Is there a greater chance of complete resorption of the calcifications in patients treated with high-energy ESWT compared with those treated with low-energy ESWT by 3 months and by 6 months?
Methods
Five relevant electronic online databases, Medline (through PubMed), EMBASE (through OVID), Cinahl (through EBSCO), Web of Science, and the Cochrane Central Register of Controlled Trials, were systematically searched. We also crosschecked the reference lists of articles and reviews for possible relevant studies. Eligible for inclusion were all randomized controlled trials (RCTs) that compared high-energy ESWT (> 0.28 mJ/mm2) with low-energy ESWT (< 0.08 mJ/mm2). One author examined titles and abstracts of each identified study to assess study eligibility. Two reviewers independently extracted data and assessed the risk of bias and study quality. The primary outcome measure, the Constant-Murley score, was assessed by comparing mean functional outcome scores between the groups. Secondary outcomes were assessed using odds ratios, when appropriate data were pooled. Based on this process, five RCTs (359 participants) were included.
Results
All five RCTs showed greater improvement in functional outcome (Constant-Murley score) in patients treated with high-energy ESWT compared with patients treated with low-energy ESWT at 3 and 6 months. The 3-month mean difference was 9.88 (95% CI, 9.04–10.72, p < 0.001; 6-month data could not be pooled). Furthermore, high-energy ESWT more often resulted in complete resorption of the deposits at 3 months. The corresponding odds ratio was 3.40 (95% CI, 1.35–8.58) and p = 0.009 (6-month data could not be pooled).
Conclusion
When shock wave therapy is chosen, high-energy shock wave therapy is more likely to result in improved Constant-Murley score and resorption of the deposits compared with low-energy therapy.
Level of Evidence
Level I, therapeutic study. See the Instructions for Authors for a complete description of levels of evidence.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Calcifying tendinitis of the shoulder is a common disease of the rotator cuff muscles that results in pain and decreased ROM. The disease mainly affects individuals between 30 and 50 years old, and males and females are equally affected. The calcific material consists of a collection of calcium hydroxyapatite in crystalline or amorphous form [5, 8, 14]. Approximately 80% the calcium deposits are located in the tendon of the supraspinatus, 15% are in the infraspinatus, and approximately 5% are in the subscapularis tendon. In the supraspinatus tendon, the most affected location is 1.5 to 2.0 cm away from its insertion at the greater tuberosity [5, 8, 11, 23]. The etiology of the calcium deposits in the rotator cuff is disputed [9, 20, 23]. It has been suggested that it is related to decreased local oxygen tension or hypoxia [5, 8]. The calcifications can be subdivided using the classification of Gärtner and Heyer [8]. Their classification is used to describe the radiologic aspect of the calcifications. It subdivides the calcifications into three groups: type I, clearly circumscribed and dense; type II, clearly circumscribed, translucent, cloudy, or dense; and type III, cloudy and translucent.
The disease is at first treated nonoperatively, including use of antiinflammatory drugs, ice therapy, physiotherapy, corticosteroid injections, and/or needling. However, when this fails, extracorporeal shock wave therapy (ESWT) can be a good and less-invasive treatment option before surgery [10, 12]. The exact mechanisms of action of the ESWT are largely unknown; Loew et al. [17] postulated that the shock waves lead to a three-way mechanism of action: (1) mechanical effect resulting in deposit fragmentation; (2) molecular effect resulting in deposit phagocytosis; and (3) analgesic effect resulting in denervation of pain receptors. Shock wave therapy can be divided into three categories based on its energy levels: low-energy (< 0.08 mJ/mm2), middle-energy (0.08–0.28 mJ/mm2), and high-energy (> 0.28 mJ/mm2) [1, 15, 20]. High-energy ESWT can induce fragmentation and destruction of solid bodies. For example, high-energy ESWT has a physical effect on kidney stones, gallstones, and bony tissue, causing physical and histologic changes. By contrast it is believed that the therapeutic effect of low-energy ESWT is based on neurophysiologic mechanisms [18, 22]. Moreover, different devices are needed to apply different energy intensities. Devices that can generate high-energy ESWT are more expensive than the devices needed for low-energy ESWT. High-energy ESWT is more painful than low-energy and more often requires (intravenous) analgesia. This is why it often is done in an inpatient setting. Low-energy ESWT, on the contrary, usually is performed in an outpatient setting by a physical therapist [1, 9].
However, regarding the functional and radiologic outcomes, the optimal therapeutic intensity has to be set and a dose-response relation has to be found [18].
We therefore performed a meta-analysis of randomized trials comparing high- with low-energy ESWT for calcifying tendinitis of the shoulder. We specifically sought to determine (1) if there a greater increase in Constant-Murley score in patients treated with high-energy ESWT compared with those treated with low-energy ESWT in the short term (3 months) and at midterm (6 months), and (2) if there is a greater chance of complete resorption of the calcifications in patients treated with high-energy ESWT compared with those treated with low-energy ESWT in the short term (3 months) and at midterm (6 months)?
Materials and Methods
Search Strategy
This review was performed and reported following the principles of the QUORUM statement [7, 19].
We systematically searched five relevant electronic online databases: Medline (through PubMed), EMBASE (through OVID), Cinahl (through EBSCO), Web of Science, and the Cochrane Central Register of Controlled Trials. In addition, the reference lists of articles and reviews were crosschecked for possible relevant studies. The search was set up using the PICO (patient [or disease], intervention [a drug or test], comparison [another drug, placebo or test], and outcome) format, and various medical terms were used for the search (Table 1).
Eligible for inclusion were all randomized controlled trials (RCTs) that compared high-energy ESWT (> 0.28 mJ/mm2) with low-energy ESWT (< 0.08 mJ/mm2).
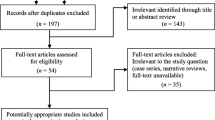
This literature search identified 194 potentially relevant studies; 108 studies were excluded after screening the titles and another 73 studies were excluded after reading the abstracts. Reasons for exclusion were that the studies were not RCTs or not concerning the shoulder. After reading the full-text articles, another eight studies were excluded, mainly because the comparison between the groups was not of our interest. The remaining five studies were eligible and are included in this systematic review. For the meta-analysis, the data of three studies was used. The results of the functional and radiologic outcomes after 3 months was pooled (Fig. 1).

The flowchart shows the results of the systematic search, including the number of articles identified and excluded at each juncture.
Data Management
The data were independently extracted by two of the authors (FUV, NidK) and crosschecked for accuracy. The authors were blinded to the authors of the included articles, their institutions, and the journals in which they were published. Data from each study were extracted in a standardized way using an extraction form specifically designed for this study. Extracted data included inclusion and exclusion criteria, inclusion period, the individual study groups, methods of randomization, blinding, type and brand of shock wave generator, intensities and frequencies of the shocks waves, primary and secondary outcome measurements, statistics used, baseline characteristics, and results (Appendix 1. Supplemental material is available with the online version of CORR). Discrepancies between the authors were resolved by scrutinizing the original article until a consensus was reached. Authors of the articles of the included studies were contacted for missing information.
Study Quality
The risk of bias and quality of the individual articles were independently assessed by two of the authors (FUV, NidK) using the criteria of Furlan et al. [7] (Tables 2 and 3). Disagreements were resolved by consensus; a third author (JWM) was consulted if necessary.
Three of the five studies qualified as high-quality RCTs. The high-quality studies were those of Albert et al. [1], Gerdesmeyer et al. [9], and Pleiner et al. [21]. The low-quality studies were those of Loew et al. [17] and Rompe et al. [22].
Characteristics of Included Studies
The total study population from five RCTs of low-versus high-energy ESWT consisted of 359 participants (Table 4). All patients were treated with conservative measures for at least 4 months before considering ESWT. No local anesthetics or corticosteroids were used with the ESWT. The patients were followed up for a minimum of 3 months and a maximum of 12 months. The primary functional outcome measure in all studies was the Constant-Murley score. The Constant-Murley score is used to assess function of the shoulder [4]. This score combines physical tests with subjective evaluations by the patients, for which 35 and 65 points respectively, can be assigned; resulting in a score between 0 (worst) and 100 (most favorable) [2–4]. The secondary outcome measures reported in the five studies were more diverse, including the VAS for pain, radiologic outcome, complication rate, and other therapies used.
Radiologic resorption of the calcium deposits was subdivided by four studies [1, 17, 21, 22] into complete disappearance, partial disappearance, and no change in the calcific deposits. Gerdesmeyer et al. [9] described the change in calcification in actual mm2 decrease, thus we did not include this article in the quantitative analysis.
Heterogeneity
The extracted data for the increase in the Constant-Murley score after 3 months showed moderate heterogeneity [7]. A random effects model was used to pool the data for the functional outcome after 3 months. The data for the increase in the Constant-Murley score after 6 months could not be pooled because the extracted data were incomplete and owing to the diversity in the timing of the final outcome moment (range, 24–30 weeks), therefore it is presented narratively.
The chance of complete resorption after 3 months showed no heterogeneity and therefore could be pooled using a fixed effect model. The data for the chance of complete resorption after 6 months could not be pooled because the extracted data were incomplete. With only three studies selected for the meta-analysis, we could not perform a meaningful funnel plot analysis to assess for publication bias.
Statistical Analysis
The Cochrane Collaboration’s Review Manager (RevMan, http://tech.cochrane.org/revman) was used to pool the data [11]. Mean difference and 95% CIs were calculated to pool the functional outcome.
For the chance of complete resorption, the pooled odds ratio with 95% CI was calculated. For the data that could not be pooled because of heterogeneity and incomplete data in the articles, the results are narratively reported.
Results
Constant-Murley Scores in Patients Treated With High- and Low-energy ESWT
Constant-Murley scores at 3 months improved to a greater degree in patients treated with high-energy ESWT than in patients treated with low-energy ESWT (Fig. 2). Pooled analysis [1, 9, 17] of the 216 patients showed that patients in the high-energy group improved by a mean of 25.82 points (SD, 10.26 points), compared with 15.94 points (SD, 6.59 points) in the low-energy group (Fig. 3). The mean difference was 9.88 (25.82 versus 15.94, 95% CI, 9.04–10.72; p < 0.001). The difference in increase in Constant-Murley scores between high-energy and low-energy ESWT ranged from 16 points [1] to 33 points [17] (Table 5).

This graph shows the data with the greater increase in Constant-Murley score after 3 months for patients treated with high-energy ESWT compared with those treated with low-energy ESWT.

The pooled results of the Constant-Murley scores after 3 months are shown.
For functional outcome after 6 months, three of the five included studies reported results similar to those after 3 months; all individual studies concluded that high-energy showed a greater increase in the functional outcome measured by the Constant-Murley score after 6 months (Fig. 4). This difference in Constant-Murley scores between high-energy and low-energy ESWT ranged from 15 points [22] to 71 points [21] (Table 4). However, these data could not be pooled because the extracted data were incomplete and owing to diversity in the timing of the final outcome moment (range, 24–30 weeks).

This graph shows the data for greater increase in Constant-Murley scores after 6 months in patients treated with high-energy ESWT compared with those treated with low-energy ESWT.
Resorption of the Calcifications
The chance of complete resorption of the calcifications at 3 months was greater in patients treated with high-energy ESWT than in patients treated with low-energy ESWT (Fig. 5). Pooled analysis [1, 17, 21] of the 163 patients showed those in the high-energy group had a greater chance of complete resorption compared with patients in the low-energy group (odds ratio, 3.40; 95% CI, 1.35–8.58; p = 0.009) (Fig. 6). The results of each study showed that high-energy ESWT results in a greater chance of resorption after 3 months. The difference in the rate of complete resorption across the different studies in patients treated with high-energy ESWT versus low-energy ESWT ranged from 10% [1, 21] to 35% [17] (Table 6).

This graph shows the data for a greater chance of complete resorption after 3 months in patients treated with high-energy ESWT compared with those treated with low-energy ESWT.

The pooled results of the chance of complete resorption after 3 months are shown.
Two studies [21, 22] showed a greater chance of complete resorption in patients treated with high-energy ESWT compared with those treated with low-energy ESWT after 6 months. The extracted data for the chance of complete resorption after 6 months could not be pooled because of the large amount of incomplete extracted data. The differences in the chance of complete resorption between patients treated with high-energy ESWT and those treated with low-energy ESWT were 11.64% [21] and 6% [22] (Fig. 7).

The data showed the greater chance of complete resorption after 6 months in patients treated with high-energy ESWT compared with those treated with low-energy ESWT.
Discussion
ESWT has been proven to be an effective treatment option after failed nonoperative treatment of calcifying tendinitis for at least 4 months [20]. It is a safe treatment option. It has few adverse events and minor side effects such as bruising and hematoma often are short-lived [9, 22]. Two cases of humeral head osteonecrosis have been reported [6]. In one case the causative relationship was questionable and in the second case the indication for ESWT was questionable [6]. There are high- and low-energy options, but the best treatment intensity has not been set yet [20, 24]. High-energy ESWT is much more painful and more expensive, and usually is done in an inpatient setting, whereas low-energy ESWT can be performed in an outpatient setting by a physical therapist [9, 21]. Therefore, we hoped to answer two research questions by a systematic review and meta-analysis. We asked whether patients treated with high-energy ESWT showed a greater increase in Constant-Murley score compared with patients treated with low-energy ESWT at 3 months and at 6 months. We also asked whether there was a greater chance of complete resorption in patients treated with high-energy ESWT compared with patients treated with low-energy ESWT at 3 and at 6 months.
This meta-analysis has some limitations; one is that the functional outcome (Constant-Murley score) after 3 and 6 months showed moderate heterogeneity, and we investigated the possible causes for this. One possible explanation could be that energy levels of the different studies were not equivalent and the devices used were not the same (Table 4). Although the comparisons were for high-energy ESWT versus low-energy ESWT, the intensity was always either more than 0.28 mJ/mm2 or less than 0.08 mJ/mm2. Another explanation could be that the included studies had different Constant-Murley scores before treatment, although they did not differ much (range, high-energy ESWT, 39.0–60.0; low-energy, ESWT, 39.4–62.7). Another limitation of the current review is use of the Constant-Murley score. Although it is a simple method to assess function of the shoulder and it has high intraobserver and interobserver reliability, the minimal clinically important difference and minimal detectable difference for patients with calcifying tendinitis has not been set yet. The minimal clinically important difference has been set for patients with a rotator cuff tear [16]. However, an increase of 9.88 points on a scale of 1 to 100 is likely to be clinically important. The reason for choosing a followup of 6 months as an end point in the included articles is because at this point the effect of the ESWT is expected but the natural self-limiting course of the disease is not yet expected [9].
High-energy ESWT resulted in a better functional outcome compared with low-energy ESWT in the short-term and mid-term. Constant-Murley scores at 3 months improved to a greater degree in patients treated with high-energy ESWT than in patients treated with low-energy ESWT (Fig. 2). Pooled analysis [1, 9, 17] showed that patients in the high-energy group improved by a mean of 25.82 points, compared with 15.94 points in the low-energy group (Fig. 3). The mean difference was 9.88 (25.82 versus 15.94, 95% CI, 9.04–10.72; p < 0.001). These findings are in line with those of Huisstede et al. [13] and Vavken et al. [24]. Huisstede et al. [13] performed a systematic review on the effectiveness of ESWT on calcific and noncalcific rotator cuff tendinitis and two studies [1, 9] were included and presented narratively that compared high-energy ESWT with low-energy ESWT. Vavken et al. [24] performed a meta-analysis in which they chose a new, nonevidence-based, cutoff point (0.20 mJ/mm2). Less than this intensity was labeled low-energy and greater than 0.20 mJ/mm2 was considered high-energy. Because of this new classification of ESWT, their included studies differed substantially from those in our study. They studied only the results 6 months after treatment. Even with these differences, the conclusions by Vavken et al. [24] are similar to those in our study.
High-energy ESWT resulted in a greater chance of complete resorption calcium deposits when compared with low-energy ESWT. The chance of complete resorption of the calcifications at 3 months was greater in patients treated with high-energy ESWT than in patients treated with low-energy ESWT (Fig. 5). Pooled analysis [1, 17, 21] showed patients in the high-energy group had a greater chance of complete resorption compared with patients in the low-energy group (odds ratio = 3.40; 95% CI, 1.35–8.58; p = 0.009) (Fig. 6). These findings are in line with the findings of Ioppolo et al. [15] and Vavken et al. [24]. Ioppolo et al. [15] performed a meta-analysis on the clinical improvement and resorption of calcifications after shock wave therapy compared with sham treatment. Vavken et al. [24] used a different cutoff point of 0.20 mJ/mm2. They also found a greater chance of complete resorption after 6 months.
Based on our meta-analysis we believe that high-energy ESWT is more effective than low-energy ESWT in terms of functional outcome (Constant-Murley score) and radiographic resorption (chance of complete resorption) of the deposits after 3 months. However there is still a need for high-quality RCTs to discover the exact dose-response relation. In our opinion, this future research should focus on high-energy ESWT because current available evidence indicates that high-energy ESWT is more effective than low-energy ESWT regarding the functional and radiologic outcomes in the short term and midterm. It also would be interesting to compare (high-energy) ESWT with other treatment modalities for conservative treatment-resistant calcifying tendinitis of the shoulder such as surgery or needling/ barbotage of the calcific deposits.
References
Albert JD, Meadeb J, Guggenbuhl P, Marin F, Benkalfate T, Thomazeau H, Chalès G. High-energy extracorporeal shock-wave therapy for calcifying tendinitis of the rotator cuff: a randomised trial. J Bone Joint Surg Br. 2007;89:335–341.
Conboy VB, Morris RW, Kiss J, Carr AJ. An evaluation of the Constant-Murley shoulder assessment. J Bone Joint Surg Br. 1996;78:229–232.
Constant CR, Gerber C, Emery RJ, Sojbjerg JO, Gohlke F, Boileau P. A review of the Constant score: modifications and guidelines for its use. J Shoulder Elbow Surg. 2008;17:355–361.
Constant CR, Murley AH. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res. 1987;214:160–164.
Diehl P, Gerdesmeyer L, Gollwitzer H, Sauer W, Tischer T. [Calcific tendinitis of the shoulder] [in German]. Orthopade. 2011;40:733–746.
Durst HB, Blatter G, Kuster MS. Osteonecrosis of the humeral head after extracorporeal shock-wave lithotripsy. J Bone Joint Surg Br. 2002;84:744–746.
Furlan AD, Pennick V, Bombardier C, van Tulder M; Editorial Board, Cochrane Back Review Group. 2009 updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine (Phila Pa 1976). 2009;34:1929–1941.
Gartner J, Heyer A. [Calcific tendinitis of the shoulder] [in German]. Orthopade. 1995;24:284–302.
Gerdesmeyer L, Wagenpfeil S, Haake M, Maier M, Loew M, Wortler K, Lampe R, Seil R, Handle G, Gassel S, Rompe JD. Extracorporeal shock wave therapy for the treatment of chronic calcifying tendonitis of the rotator cuff: a randomized controlled trial. JAMA. 2003;290:2573–2580.
Gosens T, Hofstee DJ. Calcifying tendinitis of the shoulder: advances in imaging and management. Curr Rheumatol Rep. 2009;11:129–134.
Higgins JP, Green S, eds. Cochrane Handbook for Systematic Reviews of Interventions. The Cochrane Collaboration; 2011. Available at: http://handbook.cochrane.org. Accessed January 4, 2014.
Hofstee DJ, Gosens T, Bonnet M, De Waal Malefijt J. Calcifications in the cuff: take it or leave it? Br J Sports Med. 2007;41:832–835.
Huisstede BM, Gebremariam L, van der Sande R, Hay EM, Koes BW. Evidence for effectiveness of Extracorporal Shock-Wave Therapy (ESWT) to treat calcific and non-calcific rotator cuff tendinosis: a systematic review. Man Ther. 2011;16:419–433.
Hurt G, Baker CL Jr. Calcific tendinitis of the shoulder. Orthop Clin North Am. 2003;34:567–575.
Ioppolo F, Tattoli M, Di Sante L, Venditto T, Tognolo L, Delicata M, Rizzo G, Di Tanna G, Santilli V. Clinical improvement and resorption of calcifications in calcific tendinitis of the shoulder after shock wave therapy at 6 months’ follow-up: a systematic review and meta-analysis. Arch Phys Med Rehabil. 2013;94:1699–1706.
Kukkonen J, Kauko T, Vahlberg T, Joukainen A, Aärimaa V. Investigating minimal clinically important difference for Constant score in patients undergoing rotator cuff surgery. J Shoulder Elbow Surg. 2013;22:1650–1655.
Loew M, Daecke W, Kusnierczak D, Rahmanzadeh M, Ewerbeck V. Shock-wave therapy is effective for chronic calcifying tendinitis of the shoulder. J Bone Joint Surg Br. 1999;81:863–867.
Loew M, Jurgowski W, Mau HC, Thomsen M. Treatment of calcifying tendinitis of rotator cuff by extracorporeal shock waves: a preliminary report. J Shoulder Elbow Surg. 1995;4:101–106.
Moher D, Cook DJ, Eastwood S, Olkin I, Rennie D, Stroup DF. Improving the quality of reports of meta-analyses of randomized controlled trials: the QUOROM statement. QUOROM Group. Br J Surg. 2000;87:1448–1454.
Mouzopoulos G, Stamatakos M, Mouzopoulos D, Tzurbakis M. Extracorporeal shock wave treatment for shoulder calcific tendonitis: a systematic review. Skeletal Radiol. 2007;36:803–811.
Pleiner J, Crevenna R, Langenberger H, Keilani M, Nuhr M, Kainberger F, Wolzt M, Wiesinger G, Quittan M. Extracorporeal shockwave treatment is effective in calcific tendonitis of the shoulder: a randomized controlled trial. Wien Klin Wochenschr. 2004;116:536–541.
Rompe JD, Burger R, Hopf C, Eysel P. Shoulder function after extracorporal shock wave therapy for calcific tendinitis. J Shoulder Elbow Surg. 1998;7:505–509.
Speed CA, Hazleman BL. Calcific tendinitis of the shoulder. N Engl J Med. 1999;340:1582–1584.
Vavken P, Holinka J, Rompe JD, Dorotka R. Focused extracorporeal shock wave therapy in calcifying tendinitis of the shoulder: a meta-analysis. Sports Health. 2009;1:137–144.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she, or a member of his or her immediate family, has no funding or commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Electronic supplementary material
Below is the link to the electronic supplementary material.
About this article

Cite this article
Verstraelen, F.U., in den Kleef, N.J.H.M., Jansen, L. et al. High-energy Versus Low-energy Extracorporeal Shock Wave Therapy for Calcifying Tendinitis of the Shoulder: Which is Superior? A Meta-analysis. Clin Orthop Relat Res 472, 2816–2825 (2014). https://doi.org/10.1007/s11999-014-3680-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-014-3680-0