
Abstract
Background
Surgical site infection (SSI) ranges from 1.9% to 5.5% in most large series. Minimally invasive surgery (MIS) has been postulated to reduce SSI rates.
Questions/purposes
(1) Is MIS associated with a lower incidence of SSI compared with open spinal surgery? (2) Are there other independent risk factors associated with SSI? (3) What bacteria are most common in spinal SSI?
Methods
Medical records of 2299 patients who underwent transforaminal lumbar interbody fusion, laminectomy, or discectomy were analyzed and selected for a nested case-control analysis. Twenty-seven cases with SSI were matched with 162 control subjects without SSI stratified based on procedure performed within 28 days of the case’s date of surgery. Patients were identified from an institutional database at a tertiary care hospital. MIS involved spinal procedures performed through a tubular retractor system. Univariate and multivariate analyses were performed.
Results
Patients undergoing open spinal surgery were 5.77 times more likely to develop SSI compared with MIS approaches (odds ratio [OR], 5.77; 95% confidence interval [CI], 1.0–32.7; p = 0.048). Also, from the multivariate regression model, diabetes (OR, 4.7; 95% CI, 1.3–17.0; p = 0.018), number of levels operated on (OR, 3.5; 95% CI, 1.6–7.5; p = 0.001), and body mass index (OR, 1.2; 95% CI, 1.0–1.3; p = 0.010) were predictive of an increased risk in SSI. Staphylococcus aureus was most frequently identified, being present in 12 of 21 (52.4%) patients in whom positive cultures were obtained. Four of the 12 patients had methicillin-resistant S aureus infection.
Conclusions
In our series, MIS has a lower incidence of SSI. The risk factors predictive of SSI should be further evaluated in well-designed prospective trials.
Level of Evidence
Level III, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Surgical site infection (SSI) is a serious complication after spinal surgery with significant morbidity and mortality. The rate of SSI in most large series after open spinal surgery ranges from 1.9% to 5.5% depending on a variety of risk factors [11, 13, 19, 22].
Treatment for SSI can be challenging often requiring revision surgery, long-term antibiotics, and prolonged hospitalization. The accurate identification of risk factors is thus important in the development of strategies to prevent these potentially devastating infections.
Traditional open spinal surgery requires a large midline incision and extensive muscle dissection and retraction for adequate exposure to the tips of the transverse process bilaterally. This is to facilitate accurate pedicle screw insertion in transforaminal lumbar interbody fusion (TLIF) and good exposure of the lamina in laminectomy and discectomy. The morbidity related to the iatrogenic effects of soft tissue dissection has been established [6, 18]. Minimally invasive spinal surgery (MIS), which involves a less traumatic approach while maintaining comparable surgical results to open spinal surgery, is gaining popularity. Anecdotally, infection rates after MIS have also been shown to be lower than open spinal surgery [10]. However, because MIS surgery is technically challenging and associated with a steep learning curve, longer operating time and increased complications may occur during its initial implementation [17].
We conducted a retrospective review to analyze the incidence of SSI in patients who had undergone open or MIS TLIF for spondylolisthesis, laminectomy, or laminotomy for spinal stenosis or discectomy for a prolapsed intervertebral disc. These surgeries were chosen because they could be performed in either an open or minimally invasive approach. In this study, we specifically asked whether the MIS approach is associated with (1) decreased incidence of SSI when compared with open spinal surgery; (2) also, are there other independent risk factors associated with SSI? (3) Lastly, what is the most common bacterial cause of infection among patients with SSI?
Patients and Methods
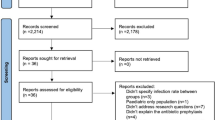
We performed a retrospective nested case-control analysis of all patients who had undergone open or MIS TLIF, laminectomy, or laminotomy and discectomy electively at our tertiary care university-affiliated hospital from January 2004 to May 2010 after approval from our hospital’s ethics committee. A total of 2299 patients were reviewed and those who developed a postoperative SSI were identified. Patients were identified from the hospital’s electronic computerized database registry and from the patients’ medical records. Inclusion criteria included all patients with the International Classification of Disease, 9th Revision, Clinical Modification (ICD-9-CM) procedure codes for TLIF (81.08), laminectomy (03.02 and 03.09), and discectomy (80.50 and 80.51). Implants were only used in patients who underwent TLIF. Exclusion criteria were patients who on admission had the ICD-9-CM diagnosis code for SSI (998.5, 998.51, and 998.59), osteomyelitis (730.08, 730.18, and 730.28), or intraspinal abscess (324.1).
The diagnosis of a SSI was based on the ICD-9-CM diagnosis codes for all 2299 patients who met our inclusion criteria. The ICD-9-CM codes are shown in parentheses for SSI (998.5, 998.51, and 998.59), cellulitis (628.1, 628.2, and 682.6), osteomyelitis (730.08, 730.18, and 730.28), wound dehiscence (998.3, 998.32), or intraspinal abscess (324.1). The electronic medical records of these patients encompassing both clinical and laboratory findings were checked for documentation of postoperative SSI. This was then correlated to the Centers for Disease Control and Prevention (CDC)/National Nosocomial Infections Surveillance (NNIS) guidelines [9]. SSI included involved incision SSI or organ space SSI. Incisional SSI was characterized by skin, subcutaneous tissue (superficial incisional SSI) involvement, or fascia and muscle (deep incisional SSI) involvement. Organ space SSI included infections involving any anatomical components excluding the skin incision, fascia, or muscle layers that were manipulated during surgery. These include osteomyelitis, meningitis, or empyema. These SSIs should have an onset within 30 days from time of operation or within 1 year in instances in which an implant was used. This was in concordance with the CDC/NNIS definition for SSI to ensure that the reported rate of SSI remains consistent and accurate.
There were a total of 27 cases of SSI from the study population (Table 1). We conducted a nested case-control study whereby 162 control subjects from our cohort of 2299 patients were compared with the 27 incident cases of SSI. This was used because the prevalence of SSI is low in spinal surgery and comparing this number against 2299 patients makes little statistical sense. Each patient who met our inclusion criteria was matched with six randomly selected control subjects (case-control) with the use of a random number generator based on predetermined matching criteria. The matching criteria were patients who underwent a similar procedure, under an elective setting, performed by surgeons of similar seniority within a 28-day window from the case patient’s date of surgery. We aimed to minimize selection bias with the use of a nested case-control study design. This is in line with what is suggested by Wacholder et al. [21] who suggested nesting case-controls within cohort studies to ensure that the control subjects are drawn from the same source population as the case series. Similar procedure refers to MIS or open TLIF cases (ie, patients with SSI) that were matched with either MIS or open TLIF control subjects (ie, patients without SSI). This was repeated for those patients with SSI who had undergone laminectomies and discectomies. No other matching variables were used so as to allow for analysis of a wide range of factors as potential risk factors for SSI. Of the 189 patients selected for the case-control analysis, there were no cases of revision surgery and hence this was not analyzed as a risk factor. In addition, none of these patients required conversion from an MIS procedure to an open procedure.
Numerous operative, patient, and anesthetic risk factors were investigated and the compiled data set was divided into discrete and continuous variables for statistical analysis. The incidence of SSI was crosstabulated against the surgical approach to evaluate if the MIS technique contributed to a lower incidence of SSI. MIS was defined as any spinal procedure performed through a tubular retractor system. Discrete variables studied included type of surgery, race, sex, number of surgical assistants (two or less or more than two), use of allograft, use of instrumentation, L5/S1 involvement, presence of diabetes, use of alcohol, consumption of corticosteroids, smoker, presence of preoperative incontinence or preoperative urinary tract infections, suboptimal antibiotics induction, American Society of Anesthesiologists score, and SSI risk stratification index (0–3). Suboptimal induction of preoperative antibiotics was defined as the administration of cefazolin or vancomycin greater than 60 minutes before incision or any antibiotics first given after incision. Continuous variables analyzed includes patient’s age, body mass index (BMI), length of operation, duration of hospitalization, number of intervertebral levels operated on, preoperative glucose levels, and estimated blood loss. These risk factors were chosen based on the previous literature evaluating SSI in spinal surgeries [7, 10, 11, 16].
Stepwise statistical analysis of the compiled data set was done to investigate for a significant correlation between potential risk factors and SSI. A univariate analysis was first performed for all risk factors. Discrete variables were analyzed using the chi-square test and the continuous variables analyzed using the independent sample two-sided t-test. After univariate analysis, variables found to have a significant correlation (p < 0.05) with SSI were put through a multivariate logistic regression. The final model consisted of the odds ratio, p value, and the 95% confidence interval, which were used to identify statistically significant independent risk factors. All statistical analyses were performed using SPSS statistical software (Version 12.0; SPSS, Chicago, IL, USA).
Results
The MIS approach was associated with a lower risk of infection than observed in patients treated with open spinal surgery. From our univariate analysis, surgical approach (MIS versus open spinal surgery, p = 0.004) was noted to be associated with a lower incidence of SSI. In addition, when the data were run through the multivariate logistic regression model, surgical approach (MIS versus open spinal surgery, p = 0.048) continued to show significance with an odds ratio of 5.77 and a confidence interval of 1.0 to 32.7.
Diabetes, number of surgical levels, and BMI were the most important prognostic variables identified with infection. The initial univariate analysis of discrete (Table 2) and continuous variables (Table 3) identified a number of significant factors (p < 0.05) that were then tested in a multivariate model (Table 4). This included the surgical approach (MIS versus open spinal surgery), type of surgery, diabetes mellitus, preoperative incontinence, preoperative urinary tract infection, suboptimal antibiotics induction, SSI risk stratification index, duration of hospital stay, number of intervertebral levels operated on, and patient’s BMI. Length of operation, which was a factor analyzed, was found not to be a significant prognostic variable (p = 0.063). From the final logistic regression model, presence of diabetes mellitus (p = 0.018), number of intervertebral levels operated on (p = 0.001), and patient’s BMI (p = 0.010) continued to show significance (Table 4).
The most common pathogen identified among patients with positive cultures was Staphylococcus aureus. Tissue culture returned positive for 21 of 27 (77.8%) patients and was primarily monomicrobial with S aureus being present in 12 of 21 (52.4%) patients. Of these 12 patients, four patients were infected with methicillin-resistant S aureus. Only two patients had three or more organisms identified. Other pathogens include Staphylococcus lugdunensis, Enterobacter species, Proteus mirabilis, Escherichia coli, Acinetobacter baumannii, Klebsiella, and Morganella morganii. Postoperatively, 25 of 27 (92.6%) patients had SSI within a minimum of 2 days and a maximum of 29 days. The median time to detection of SSI was 15 days. The two other patients had SSI at 39 and 334 days postoperatively, respectively. All 27 patients were treated with intravenous antibiotics and 13 of 27 (48.1%) patients required a repeat operation (p < 0.001).
Discussion
SSI ranges from 1.9% to 5.5% in most large series [11, 13, 14, 19, 22]. MIS has been postulated to reduce SSI rates [10]. However, the steep learning curve associated with the development of a MIS surgery skill set may lead to increased complications in its initial implementation [17]. Accordingly, we sought to determine whether the MIS approach is associated with a lower risk of spinal SSI and to identify other independent risk factors for the development of SSI in spinal surgery. Finally, we sought to identify the most common infecting organisms in spinal surgery performed at a tertiary care setting.
However, we acknowledge the presence of a few limitations in our study. First, we analyzed the data using a nested case-control model instead of analyzing the entire cohort. We used this because the nested case-control model is an efficient design for investigating risk factors for SSI, which is a rare but serious complication after spinal surgery. This study model allows the importance of individual risk factors causing SSI to be evaluated in the setting of a low-frequency event (there were only 27 infections in the series). Although we identified the MIS approach as having a lower risk of infection than did open approaches, the confidence intervals for this finding were wide and approached a no-difference finding on the low end. This borderline significance, in the context of a study that described a relatively uncommon event, suggests that even a few additional events in one group or another might have resulted in a conclusion of no difference in infection between the MIS and other treatment groups. Because followup was less than 100%, one has to consider this issue carefully, and because of it, we believe our findings on this point need to be validated in large, multicenter, comparative studies.
Second, we acknowledge the potential for selection bias in our study. Because our study aimed to evaluate potential risk factors for SSI, a wide array of variables had to be analyzed and hence the cases identified were matched to control subjects for only a few variables. We tried to minimize risk of selection bias in our study design by using a nested case-control model. All cases were carefully identified from our cohort of 2299 patients and control subjects selected from patients at risk at the time each case of SSI occurred. As such, all cases were matched with control subjects within a 28-day period in case of operating room contamination. Also, control subjects have had to undergo a similar procedure under an elective setting and performed by a surgeon of similar seniority.
Third, we acknowledged that a stepwise statistical analysis of data with a p value of < 0.05 does not always equate to a more accurate predictive model as compared with one that includes all potential risk factors [20]. However, we chose this model because it would provide us with a clear framework on how to use our data. This allows for easy application of results to the clinical setting.
It is worth noting that the MIS technique itself has some limitations. MIS approaches can be technically challenging [3]. The working surgical field is significantly smaller compared with open surgery. Additionally, MIS instruments have a longer lever arm and hence are more difficult to manipulate. Lastly, surgeons have to acquire the proficiency in mentally mapping their three-dimensional surgical position using two-dimensional intraoperative image guidance. During the learning curve, longer operative time and increased rates of complication may be expected [17].
We found a lower rate of infection in the MIS group compared with patients treated using traditional open approaches. The infection rates in our series were similar to those found in the literature [10, 12, 19]. In a recent large multicenter retrospective review of a prospectively collected database, SSI was noted in 2.9% of patients (181 of 6241) who underwent open TLIF versus 1.3% of patients (11 of 848) who underwent MIS TLIF (p = 0.005) [19]. In addition, when they analyzed MIS versus the open spinal surgery approach based on all 108,419 procedures, SSI in the MIS approach was 0.5% (78 of 14,301) compared with 2.4% (2280 of 94,115) using the open spinal approach (p < 0.001) [19]. These findings together with our results suggest that the MIS approach is indeed clinically superior in reducing postoperative SSI.
In this study, we found an increased risk for SSI in patients who received the open approach compared with the MIS approach to TLIF, laminectomy, or laminectomy and discectomy. However, although the effect size seems large, the confidence intervals were wide and the statistical significance only borderline. In the context of a clinical series that included a relatively small number of events such as ours, this suggests that even a few more infections in one group (which might have occurred, and not been detected, given that there was some loss to followup) would have resulted in a finding that was not statistically significant [3, 10]. MIS with the use of a tubular retractor system theoretically minimizes tissue injury and may have contributed to lowered rates of postoperative SSI. Additionally, MIS ensures that deeper tissues are less exposed to potential pathogens as a result of a more restricted surgical field [10]. This was demonstrated by Smith et al. who showed that the MIS approach significantly lowered rates of postoperative wound infection, especially deep wound infection, as compared with open spinal surgery [19]. Lastly, disturbance of the skin and skin flora is reduced because they are guarded by fixed tubes [10]. The potential dead space that results from the open surgical technique is significantly minimized, thus perhaps decreasing the risk of postoperative hematomas or seromas that may be subsequently infected.
In our study, we also found diabetes, obesity, and number of intervertebral levels operated on to be the other significant independent risk factors for postoperative SSI. This has been attributed to the poor oxygenation in the surgical wound site in patients with diabetes and the increase in dead space after wound closure in obese patients [1, 5, 8, 14]. With more levels operated on, operating time, size of surgical site exposed, blood loss, and length of hospitalization are expected to increase predisposing one to postoperative SSI.
We found that S aureus was the most common primary monomicrobial pathogen cultured. This finding was similar to that found in the literature where S aureus was noted to occur in more than 50% of postoperative spine infection [2, 4, 15]. In our series, all patients were managed conservatively with intravenous antibiotics and only 13 patients required additional surgical intervention. Hong et al. notes that early diagnosis and treatment with sensitive antibiotics are essential for the successful conservative treatment of acute postoperative spinal infections [4]. In our center, methicillin-resistant S aureus infection is still relatively low affecting 14.8% (four of 27) of our patients. As such, patients diagnosed to have SSI were empirically started on intravenous cloxacillin rather than intravenous vancomycin because overuse can bring about increased incidence of vancomycin-resistant pathogens.
Our study suggests that surgical approach is an independent risk factor for postoperative SSI, but although the effect size was large, the confidence intervals were wide, and statistical significance of this finding was borderline. As such, this finding needs to be confirmed by further comparative trials. Our analysis also supports previous reports that presence of diabetes, increased number of intervertebral level operated on, and patient’s BMI are independent risk factors and that S aureus is the most common pathogen identified in these infections. Although the incidence of SSI cannot be totally eliminated, controlling accurately identified independent risk factors may further reduce the likelihood of postoperative SSI.
References
Choban PS, Heckler R, Burge JC, Flancbaum L. Increased incidence of nosocomial infections in obese surgical patients. Am Surg. 1995;61:1001–1005.
Fang A, Hu SS, Endres N, Bradford DS. Risk factors for infection after spinal surgery. Spine. 2005;30:1460–1465.
Gejo R, Matsui H, Kawaguchi Y, Ishihara H, Tsuji H. Serial changes in trunk muscle performance after posterior lumbar surgery. Spine. 1999;24:1023–1028.
Hong HS, Chang MC, Liu CL, Chen TH. Is aggressive surgery necessary for acute postoperative deep spinal wound infection? Spine. 2008;33:2473–2478.
Kabon B, Nagele A, Reddy D, Eagon C, Fleshman JW, Sessler DI, Kurz A. Obesity decreases perioperative tissue oxygenation. Anesthesiology. 2004;100:274–280.
Kawaguchi Y, Matsui H, Tsuji H. Back muscle injury after posterior lumbar spine surgery. A histologic and enzymatic analysis. Spine. 1996;21:941–944.
Koutsoumbelis S, Hughes AP, Girardi FP, Cammisa FP Jr, Finerty EA, Nguyen JT, Gausden E, Sama AA. Risk factors for postoperative infection following posterior lumbar instrumented arthrodesis. J Bone Joint Surg Am. 2011;93:1627–1633.
LaVan FB, Hunt TK. Oxygen and wound healing. Clin Plast Surg. 1990;17:463–472.
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. Am J Infect Control. 1999;27:97–132; quiz 133–134; discussion 196.
O’Toole JE, Eichholz KM, Fessler RG. Surgical site infection rates after minimally invasive spinal surgery. J Neurosurg. 2009;11:471–476.
Olsen MA, Nepple JJ, Riew KD, Lenke LG, Bridwell KH, Mayfield J, Fraser VJ. Risk factors for surgical site infection following orthopaedic spinal operations. J Bone Joint Surg Am. 2008;90:62–69.
Parker SL, Adogwa O, Witham TF, Aaronson OS, Cheng J, McGirt MJ. Post-operative infection after minimally invasive versus open transforaminal lumbar interbody fusion (TLIF): literature review and cost analysis. Minim Invasive Neurosurg. 2011;54:33–37.
Picada R, Winter RB, Lonstein JE, Denis F, Pinto MR, Smith MD, Perra JH. Postoperative deep wound infection in adults after posterior lumbosacral spine fusion with instrumentation: incidence and management. J Spinal Disord. 2000;13:42–45.
Pullter Gunne AF, Cohen DB. Incidence, prevalence, and analysis of risk factors for surgical site infection following adult spinal surgery. Spine. 2009;34:1422–1428.
Schimmel JJ, Horsting PP, de Kleuver M, Wonders G, van Limbeek J. Risk factors for deep surgical site infections after spinal fusion. Eur Spine J. 2010;19:1711–1719.
Schuster JM, Rechtine G, Norvell DC, Dettori JR. The influence of perioperative risk factors and therapeutic interventions on infection rates after spine surgery: a systematic review. Spine. 2010;35:S125–137.
Schwender JD, Foley KT, Holly LT, Transfeldt EE. Minimally invasive posterior surgical approaches to the lumbar spine. In: Rothman RH, Simeone FA, Herkowitz HN, eds. The Spine. 5th ed. Philadelphia, PA, USA: Saunders/Elsevier; 2006:333–341.
Sihvonen T, Herno A, Paljarvi L, Airaksinen O, Partanen J, Tapaninaho A. Local denervation atrophy of paraspinal muscles in postoperative failed back syndrome. Spine. 1993;18:575–581.
Smith JS, Shaffrey CI, Sansur CA, Berven SH, Fu KM, Broadstone PA, Choma TJ, Goytan MJ, Noordeen HH, Knapp DR Jr, Hart RA, Donaldson WF 3rd, Polly DW Jr, Perra JH, Boachie-Adjei O. Rates of infection after spine surgery based on 108,419 procedures: a report from the Scoliosis Research Society Morbidity and Mortality Committee. Spine. 2011;36:556–563.
Steyerberg EW, Eijkemans MJ, Harrell FE Jr, Habbema JD. Prognostic modeling with logistic regression analysis: in search of a sensible strategy in small data sets. Med Decis Making. 2001;21:45–56.
Wacholder S, Silverman DT, McLaughlin JK, Mandel JS. Selection of controls in case-control studies. II. Types of controls. Am J Epidemiol. 1992;135:1029–1041.
Weinstein MA, McCabe JP, Cammisa FP Jr. Postoperative spinal wound infection: a review of 2,391 consecutive index procedures. J Spinal Disord. 2000;13:422–426.
Acknowledgments
We thank Bennet Ong, Dr Vinaykumar M. Siddaraju, and Dr Ian Cheung for their assistance in data acquisition.
Author information
Authors and Affiliations
Corresponding author
Additional information
One of the authors (WMY) certifies that he is a consultant to Medtronic (Singapore) and has received payment of benefits during the study period an amount of USD 10,000 to USD 100,000. Also he is a consultant to DePuy-Synthes (Singapore) and has received payment of benefits during the study period, an amount of less than USD 10,000. In addition, he receives fellowship support from Medtronic of an amount of USD 10,000 to USD 100,000 and fellow support from Depuy-Synthes of an amount of USD 10,000 to USD 100,000. Also, he has received a research grant from Medtronic for an unrelated topic of an amount of USD 10,000 to USD 100,000.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
About this article
Cite this article
Ee, W.W.G., Lau, W.L.J., Yeo, W. et al. Does Minimally Invasive Surgery Have a Lower Risk of Surgical Site Infections Compared With Open Spinal Surgery?. Clin Orthop Relat Res 472, 1718–1724 (2014). https://doi.org/10.1007/s11999-013-3158-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-013-3158-5