
Abstract
Background
Obese children reportedly have an increased risk of sustaining musculoskeletal injuries compared with their normal-weight peers. Obese children are at greater risk for sustaining fractures of the forearm, particularly from low-energy mechanisms. Furthermore, obesity is a risk factor for sustaining an extremity fracture requiring surgery. However, it is unclear what role obesity plays in fractures about the distal humerus.
Questions/purposes
We therefore asked whether (1) children who sustain lateral condyle (LC) fractures have a higher body mass index (BMI) as compared with those with supracondylar (SC) humerus fractures; and (2) children with a higher BMI sustain more severe fractures regardless of fracture pattern.
Methods
We retrospectively reviewed 992 patients: 230 with LC injuries and 762 with SC fractures. We determined BMI and BMI-for-age percentiles. Fracture types were classified by the systems proposed by Weiss et al. (LC fractures) and Wilkins (SC fractures).
Results
The LC group had both a higher mean BMI and BMI-for-age percentile than the SC group as well as had more obese patients (37% versus 19%). Within the LC group, children with Type 3 fractures had a higher BMI that those with Type 1 fractures (19 versus 17). There was a higher percentage of obese patients with Type 3 LC fractures compared with Type 1 and 2 fractures (44% versus 27% and 26%). Among patients with SC fractures, there was no difference among the BMI, BMI-for-age percentiles, or percentage of obese children when analyzed by fracture subtype.
Conclusions
Obesity places a child at greater risk for sustaining a LC fracture and when these fractures occur, they are often more severe injuries compared with those in nonobese children.
Level of Evidence
Level II, prognostic study. See the Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Childhood obesity continues to be a growing epidemic in the United States [7, 15]. The most recent data from the Centers of Disease Control and Prevention indicate that 16.9% of children and adolescents are obese, defined as a body mass index (BMI)-for-age > 95th percentile [17], and there is evidence that the prevalence of obesity among children will reach 30% by 2030 [27]. Childhood obesity is a risk factor for greater morbidity later in life, including diabetes, coronary artery disease, musculoskeletal problems, and increased mortality [2, 4, 7, 15, 19, 25, 32].
The relationship between pediatric obesity and overall injury risk is well documented [4, 7, 8, 25]. Previous studies have demonstrated obese children have an increased risk of sustaining an injury compared with their normal-weight peers (OR 1.51) [9] and increased weight status has been associated with a 1.7 times increased fracture risk [3], particularly for fractures incurred from low-energy mechanisms [3]. Furthermore, when fractures do occur in obese children, they have been associated with a higher prevalence of complications including decubitus ulcers (1% versus 0.2%) [20], deep vein thrombosis (0.7% versus 0%) [20], and other postoperative complications, including refracture, wound infection, and wound dehiscence [14].
Upper extremity fractures occur frequently in the pediatric population with 7% to 9% involving the elbow region [13]. Among fractures around the elbow in the pediatric population, supracondylar humerus fractures are the most common, representing approximately 65% of these fractures followed in frequency by lateral humeral condyle fractures [13, 18]. Previous studies have examined the association between pediatric obesity and other common pediatric fractures, including those of the forearm [3, 9–11, 23, 24] and femur [14], and have shown that obese children are at greater risk for sustaining these injuries. However, it unclear whether there is any relationship between obesity and elbow fractures.
We therefore asked whether (1) children who sustained lateral condyle fractures would have a higher BMI as compared with those with supracondylar humerus fractures; and (2) children with a higher BMI would sustain more severe fractures regardless of fracture pattern.
Patients and Methods
From our three centers we retrospectively identified and reviewed all 1345 patients with lateral condyle (LC) (n = 302) or supracondylar (SC) (n = 1043) fractures treated from 2006 to 2011 at two sites and 2009 to 2011 at the third (height data were not routinely recorded before 2009). Of these, 353 were excluded because they lacked height or weight data. This left 992 patients: 230 with LC injuries and 762 with SC (Fig. 1). We obtained institutional review board approval at all three centers.

The illustration shows how patients were selected. fxs = fractures.
For all patients who met the inclusion criteria, we performed a chart review and demographic data (age, laterality, height, weight, and BMI) was extracted. All BMI values were converted to BMI-for-age percentiles for children age 2 years and older, because this is the standard means by which BMI is interpreted in the pediatric and adolescent population [17, 19]. The two fracture groups were similar (p = 0.92) with respect to mean age (LC: 5 years; SC: 5 years).
Two of us (EF, MS), neither of whom was a treating surgeon, independently reviewed all radiographs to confirm the fracture type and classification, which had been previously recorded in the clinical record. Before analyzing all the radiographs, we reviewed images of the individual fracture types with our senior authors to ensure uniformity in our review. For SC humerus fractures, we used the Wilkins’ modification [31] to the Gartland classification [6]. The Wilkins’ modification subclassifies the Type 3 fractures into those that are displaced posteromedially or posterolaterally. For data analysis purposes, we classified flexion-type injuries as Type 4 fractures. For LC fractures, we used the system proposed by Weiss et al. [29] and Wilkins [31] who classified the fractures based on fracture displacement and articular congruity. Type 1 fractures have less than 2 mm of displacement; Type 2 fractures have > 2 mm displacement and congruity of the articular surface; Type 3 fractures have > 2 mm of displacement and lack of articular congruity. Their work demonstrated that the postoperative complication rate was directly related to severity of displacement.
Data are summarized with descriptive statistics; continuous data are presented as mean ± SD, whereas categorical variables are presented as percentages. Comparisons of continuous data were performed using analysis of variance and differences in proportions were analyzed using chi square tests. We performed an analysis between the SC and LC groups with regard to BMI and BMI percentile. We also subdivided the patients into three groups based on their BMI percentile-for-age (normal, < 85th percentile; overweight, 85th–95th percentile; obese, > 95th percentile) and used chi square analysis to compare the percentages of patients within each group with their fracture pattern. Finally, we conducted two similar analyses within each fracture group (one for the SC and one for the LC) to compare the BMI and BMI percentile-for-age as they related to the fracture subtypes. Tests were two-sided.
Results
The LC group had a higher (p ≤ 0.001) mean BMI than the SC group: 18.5 versus 16.9 kg/m2, respectively. Similarly, the mean BMI-for-age percentile was higher (p ≤ 0.001) in the LC group compared with the SC group (69% versus 58%) (Table 1). The analysis of the three BMI percentile-for-age groups (normal, overweight, obese) revealed 23% of the children included in this study were classified as obese. The LC group had more (p < 0.001) obese patients than the SC group (37% versus 19%) (Table 2).
Within the LC group, there was a difference (p = 0.026) between the BMI of children with Type 3 fractures compared with Type 1 fractures (Table 3). There was also a trend for a higher (p = 0.06) BMI in the Type 3 fractures compared with the Type 2 fractures (Table 3). There was also a higher (p = 0.05) percentage of obese patients with LC Type 3 fractures (44%) compared with Type 1 (26%) and 2 (27%) fractures (Table 4). Within the SC group, there was no difference (p > 0.05) between the BMI or BMI-for-age percentiles of the children when analyzed by fracture subtype (Table 5). There was also no difference in the percentage of obese and nonobese patients in each SC fracture subgroup (Table 6).
Discussion
Childhood obesity is an ongoing epidemic in the United States [7, 15] as well as around the world [15]. Nationally, 17% of children and adolescents are obese [17]. In our population, the obesity rate was 23%. Unlike adults, in whom obesity has some protective effects [30], a greater risk of fracture is well documented in obese children [30]. It is unclear, however, whether childhood obesity influences the risk of type or severity of fractures around the elbow. Therefore, we determined whether children who sustain LC fractures have a higher BMI compared with those with SC humerus fractures and whether obese children sustain more severe fractures compared with their nonobese counterparts.
There are several limitations of our study. First, this study is retrospective in nature and the accuracy of the data is determined by accurate recording of patient height and weight in the clinical or operative settings. Although our sample size was large, we excluded a number of patients as a result of incomplete documentation. We believed this was justified because BMI is the gold standard for measuring obesity. Second, we did not evaluate patient functional recovery or complications, which ultimately will be necessary to confirm that obesity places these children at higher risk for more postinjury complications and greater long-term disability.
We found patients with LC fractures had a higher BMI than those with SC fractures. Furthermore, the average BMI-percentile-for-age was higher for the LC group and there were more obese patients in the LC cohort compared with the SC cohort. Previous authors, including Rana et al. [20] and Leet et al. [14], have shown that childhood obesity alone is a risk factor for an increased number of both nonoperative and operative complications. LC fractures are intraarticular physeal injuries with a higher incidence of complications, including problems with nonunion, growth arrest with subsequent malunion, angular deformities, and early arthritis compared with SC humerus fractures, and a high number of LC fractures necessitates open surgical intervention [22].
The question remains why obese children are at an increased risk of fracture in the first place. Children who are overweight or obese may fall with more force and in a more awkward manner than children who are of normal weight. Davidson et al. [3] reported that overweight male adolescents had poorer balance than healthy weight adolescents. They suggested that the poorer balance of boys with high adiposity may increase their risk for falling during daily activities, impede their ability to halt their forward progress once they begin to fall, and subsequently raise their risk for sustaining fractures [3]. Other factors have been associated with increased fracture risk. Skaggs et al. [24] showed that girls who sustained forearm fractures from minimal trauma had increased body mass and a smaller cross-sectional area in their bones, which put them at a distinct biomechanical disadvantage and higher risk of fracture. Low bone mineral density, which may arise from low levels of physical activity, also appears to play a distinct role. Weiler et al. [28] showed that increased body fat has a negative effect on attaining peak bone mass and bone mineral content. Further work by Goulding et al. [8–11] also determined that obese children have decreased bone mineral density, bone mass, and bone accrual, which placed them at increased risk for fractures.
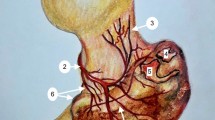
Regardless of their BMI, all of the children included in our study sustained a fracture. The question that remains unanswered is why the obese children in our study population sustained a greater number of LC fractures over SC fractures. It is our belief that this has to do with both their increased weight status as well as the mechanism of injury that leads to this fracture pattern (Fig. 2). Jakob et al. [12] demonstrated these fractures are caused by a varus force during a fall onto an extended elbow with the forearm supinated and the resulting pull of the extensor tendons and lateral collateral ligament results in avulsion of the lateral condyle. Other authors contend these fractures are the result of a upward and outward force transmitted along the radius to the capitellum [16]. The most likely cause is a combination of both these pull-off and push-off mechanisms [26]. This is in contrast to the mechanism of SC humerus fractures, which are usually higher energy injuries secondary to falls from heights onto an outstretched arm [5]. Thus, our hypothesis is that because of their known difficulties with mobility and balance, obese children are at greater risk for falling from low heights and have greater difficultly bracing their falls on a fully extended arm. This results in an increased weight-related force across the lateral aspect of their elbows during such falls, thus making them more likely to sustain a LC fracture (Fig. 2). Further studies of pediatric elbow fractures that included a collection of information on the weight of the patient as well as specifics on the exact mechanism of injury and height of the fall would help validate this hypothesis.

Proposed mechanisms of lateral condyle fractures versus supracondylar fractures. (A) Lateral condyle fracture: obese child sustaining a low-velocity injury as a result of a fall from a standing height. As a result of their increased weight status, the obese child is unable to fully extend their arm to get their center of mass over their outstretched arm. This results in a varus moment about the elbow resulting in a lateral condyle fracture. (B) Supracondylar humerus fracture: normal-weight child sustaining a higher velocity injury resulting from a fall from a height. This child sustained a supracondylar humerus fracture as a result of their ability to get their center of mass over their fully extended outstretched arm most commonly resulting in an extension-type elbow injury.
Our study adds to the growing body of literature on the detrimental effects childhood obesity has on the musculoskeletal system. The short-term and long-term consequences have a tremendous impact on both individual well-being and contribute to increased societal, workplace, and healthcare costs [15, 21]. Efforts need to continue on a national level to raise awareness of this epidemic in the pediatric population so that early intervention can be instituted and patients and their families can be properly counseled on the increased risk obesity poses to them [1, 4, 7, 14, 15, 30].
References
Bostman OM. Body mass index of patients with elbow and ankle fractures requiring surgical treatment. J Trauma. 1994;37:62–65.
Chan G, Chen CT. Musculoskeletal effects of obesity. Curr Opin Pediatr. 2009;21:65–70.
Davidson PL, Goulding A, Chalmers DJ. Biomechanical analysis of arm fracture in obese boys. J Paediatr Child Health. 2003;39:657–664.
Deckelbaum RJ, Williams CL. Childhood obesity: the health issue. Obes Res. 2001;9(Suppl 4):239S–243S.
Farnsworth CL, Silva PD, Mubarak SJ. Etiology of supracondylar humerus fractures. J Pediatr Orthop. 1998;18:38–42.
Gartland JJ. Management of supracondylar fractures of the humerus in children. Surg Gynecol Obstet. 1959;109:145–154.
Gettys FK, Jackson JB, Frick SL. Obesity in pediatric orthopaedics. Orthop Clin North Am. 2011;42:95–105, vii.
Goulding A. Risk factors for fractures in normally active children and adolescents. Med Sport Sci. 2007;51:102–220.
Goulding A, Cannan R, Williams SM, Gold EJ, Taylor RW, Lewis-Barned NJ. Bone mineral density in girls with forearm fractures. J Bone Miner Res. 1998;13:143–148.
Goulding A, Grant AM, Williams SM. Bone and body composition of children and adolescents with repeated forearm fractures. J Bone Miner Res. 2005;20:2090–2096.
Goulding A, Jones IE, Taylor RW, Williams SM, Manning PJ. Bone mineral density and body composition in boys with distal forearm fractures: a dual-energy x-ray absorptiometry study. J Pediatr. 2001;139:509–515.
Jakob R, Fowles JV, Rang M, Kassab MT. Observations concerning fractures of the lateral humeral condyle in children. J Bone Joint Surg Br. 1975;57:430–436.
Kasser J, Beaty J. The elbow region: general concepts in the pediatric patient. In: Beaty J, Kasser J, eds. Fractures in Children. 6th ed. Philadelphia, PA, USA: Lippincott Williams & Wilkins; 2006:529–530.
Leet AI, Pichard CP, Ain MC. Surgical treatment of femoral fractures in obese children: does excessive body weight increase the rate of complications? J Bone Joint Surg Am. 2005;87:2609–2613.
Maffeis C, Tato L. Long-term effects of childhood obesity on morbidity and mortality. Horm Res. 2001;55(Suppl 1):42–45.
Milch H. Fractures and fracture dislocations of the humeral condyles. J Trauma. 1964;4:592–607.
Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity and trends in body mass index among US children and adolescents, 1999–2010. JAMA. 2012;307:483–490.
Otsuka NY, Kasser JR. Supracondylar fractures of the humerus in children. J Am Acad Orthop Surg. 1997;5:19–26.
Pollak P. The impact of childhood obesity on bones. AAOS Now. 2008;2:17–20.
Rana AR, Michalsky MP, Teich S, Groner JI, Caniano DA, Schuster DP. Childhood obesity: a risk factor for injuries observed at a level-1 trauma center. J Pediatr Surg. 2009;44:1601–1605.
Russell GV, Pierce CW, Nunley L. Financial implications of obesity. Orthop Clin North Am. 2011;42:123–127, vii.
Rutherford A. Fractures of the lateral humeral condyle in children. J Bone Joint Surg Am. 1985;67:851–856.
Ryan LM, Teach SJ, Searcy K, Singer SA, Wood R, Wright JL, Chamberlain JM. Epidemiology of pediatric forearm fractures in Washington, DC. J Trauma. 2010;69(Suppl):S200–205.
Skaggs DL, Loro ML, Pitukcheewanont P, Tolo V, Gilsanz V. Increased body weight and decreased radial cross-sectional dimensions in girls with forearm fractures. J Bone Miner Res. 2001;16:1337–1342.
Taylor ED, Theim KR, Mirch MC, Ghorbani S, Tanofsky-Kraff M, Adler-Wailes DC, Brady S, Reynolds JC, Calis KA, Yanovski JA. Orthopedic complications of overweight in children and adolescents. Pediatrics. 2006;117:2167–2174.
Tejwani N, Phillips D, Goldstein RY. Management of lateral humeral condylar fracture in children. J Am Acad Orthop Surg. 2011;19:350–358.
Wang Y, Beydoun MA, Liang L, Caballero B, Kumanyika SK. Will all Americans become overweight or obese? estimating the progression and cost of the US obesity epidemic. Obesity (Silver Spring). 2008;16:2323–2330.
Weiler HA, Janzen L, Green K, Grabowski J, Seshia MM, Yuen KC. Percent body fat and bone mass in healthy Canadian females 10 to 19 years of age. Bone. 2000;27:203–207.
Weiss JM, Graves S, Yang S, Mendelsohn E, Kay RM, Skaggs DL. A new classification system predictive of complications in surgically treated pediatric humeral lateral condyle fractures. J Pediatr Orthop. 2009;29:602–605.
Whiting SJ. Obesity is not protective for bones in childhood and adolescence. Nutr Rev. 2002;60:27–30.
Wilkins K. Fractures and dislocations of the elbow region. In: Rockwood C, Wilkins K, King R, eds. Fractures in Children. 4th ed. Philadelphia, PA, USA: JB Lippincott; 1984:680–681.
Wills M. Orthopedic complications of childhood obesity. Pediatr Phys Ther. 2004;16:230–235.
Acknowledgments
We thank Eli Adhoot for his help with data collection and J. D. Bomar for his assistance in producing the illustrations.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she, or a member of their immediate family, has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation and that all investigations were conducted in conformity with ethical principles of research.
This study was performed at Rady Children’s Hospital and Health Center, San Diego, CA, USA; Children’s Hospital of Orange County, Orange, CA, USA; and Riverside County Regional Medical Center, Moreno Valley, CA, USA.
About this article
Cite this article
Fornari, E.D., Suszter, M., Roocroft, J. et al. Childhood Obesity as a Risk Factor for Lateral Condyle Fractures Over Supracondylar Humerus Fractures. Clin Orthop Relat Res 471, 1193–1198 (2013). https://doi.org/10.1007/s11999-012-2566-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-012-2566-2