
Abstract
Background
Several available compositional MRIs seem to detect early osteoarthritis before radiographic appearance. Delayed gadolinium-enhanced MRI of cartilage (dGEMRIC) has been most frequently used in clinical studies and reportedly predicts premature joint failure in patients undergoing Bernese periacetabular osteotomies (PAOs).
Questions/Purposes
We asked, given regional variations in biochemical composition in dysplastic hips, whether the dGEMRIC index of the anterior joint would better predict premature joint failure after PAOs than the coronal dGEMRIC index as previously reported.
Methods
We retrospectively reviewed 43 hips in 41 patients who underwent Bernese PAO for hip dysplasia. Thirty-seven hips had preserved joints after PAOs and six were deemed premature failures based on pain, joint space narrowing, or subsequent THA. We used dGEMRIC to determine regional variations in biochemical composition. Preoperative demographic and clinical outcome score, radiographic measures of osteoarthritis and severity of dysplasia, and dGEMRIC indexes from different hip regions were analyzed in a multivariable regression analysis to determine the best predictor of premature joint failure. Minimum followup was 24 months (mean, 32 months; range, 24–46 months).
Results
The two cohorts were similar in age and sex distribution. Severity of dysplasia was similar as measured by lateral center-edge, anterior center-edge, and Tönnis angles. Preoperative pain, joint space width, Tönnis grade, and coronal and sagittal dGEMRIC indexes differed between groups. The dGEMRIC index in the anterior weightbearing region of the hip was lower in the prematurely failed group and was the best predictor.
Conclusions
Success of PAO depends on the amount of preoperative osteoarthritis. These degenerative changes are seen most commonly in the anterior joint. The dGEMRIC index of the anterior joint may better predict premature joint failure than radiographic measures of hip osteoarthritis and coronal dGEMRIC index.
Level of Evidence
Level II, prognostic study. See Instructions for Authors for a complete description of levels of evidence.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Osteoarthritis (OA) causes pain and disability for the aging population and has considerable impact on healthcare costs [9]. Hip and knee arthroplasties have become two of the most common surgical procedures performed today, and the numbers of hip and knee arthroplasties performed are expected to double from 2000 to 2020 [22]. How OA develops is not well understood, but it is now accepted that biomechanical abnormalities in the joint that result in repetitive joint injury can initiate and accelerate the disease process. Such is the case with developmental dysplasia of the hip (DDH) and femoroacetabular impingement (FAI), with their characteristic abnormal morphologies of the hips. By some estimates, 20% to 40% of hips requiring arthroplasties may be due to secondary OA from DDH [3, 26, 64]. The smaller area of anterolateral acetabular coverage in DDH increases mechanical stress in the cartilage, which results in cartilage damage [28]. FAI with variable anatomic abnormalities of the acetabulum and/or femoral head is also a more recently recognized contributor to OA by mechanical impingement leading to direct stress to the articular cartilage or via damage to the labrum [5, 71].
Traditionally, the diagnosis of OA is made using radiographs, which indirectly assess cartilage damage by measuring apparent joint space loss (distance between acetabular and femoral subchondral plates) or bony reaction to the arthritis. However, radiographs cannot detect early cartilage injuries [21]. Conventional MRI allows direct visualization of the morphology of cartilage, including fissuring or partial- to full-thickness cartilage loss as a result of OA. With higher field strength magnets, improved visualization of morphologic changes in cartilage is possible, but detection of compositional changes, which usually precede morphologic changes, is not possible with conventional MRI.
Mature hyaline cartilage is composed of relatively few chondrocytes (2%) and the rest is composed of extracellular matrix comprised of water (70%) and macromolecules, predominately Type II collagen fibers and proteoglycan molecules. Early OA is characterized by loss of proteoglycans, which is followed by loss of collagen and changes in collagen orientation [74]. These biochemical properties in cartilage can deteriorate with mechanical overload without any radiographic changes. To improve our understanding of the natural history of OA development and to detect more sensitive and rapid outcome measures of pharmacologic and surgical interventions, recent studies have focused on using proteoglycan, collagen, and/or water content in hyaline cartilage as biomarkers for quantifying early OA and its progression.
Several compositional technique MRIs are available: T2 mapping, T1ρ, diffusion-weighted imaging, sodium MRI, and delayed gadolinium-enhanced MRI of cartilage (dGEMRIC) (Appendix 1). These MRI techniques have the potential to become valid imaging biomarkers that may affect the management of clinical therapies. At present, the best validated and commonly utilized technique for the hip is dGEMRIC. dGEMRIC utilizes a negatively charged gadolinium-based contrast agent, which acts as a probe to measure the negative charge density of cartilage. It is a specific measure of glycosaminoglycan content of cartilage. dGEMRIC has been validated against histology in vitro and ex vivo and clinically in hips and knees [4, 10, 15, 31, 42, 51, 61, 68]. The dGEMRIC index reportedly correlates with hip pain and degree of hip dysplasia [31]. Similar findings were also seen in patients with FAI, where dGEMRIC correlated with pain and alpha angle [29]. Additionally, dGEMRIC mapping of hips with history of slipped capital femoral epiphysis demonstrated differences between hips with normal and severe offsets [79].
Bernese periacetabular osteotomy (PAO) is effective for mild to severe hip dysplasia in relieving hip pain and improving joint biomechanics. This osteotomy may slow the progression of secondary OA and delay the need for salvage surgery, arthrodesis, or arthroplasty [11, 16, 17, 27, 50, 55, 57, 62, 65, 73]. In general, early reconstructive osteotomies performed on younger patients who have little radiographic evidence of OA by Tönnis grades are regarded the best candidates for this procedure [16, 33, 41, 47, 50, 73]. We expect hips that fail prematurely after osteotomy would have more evidence of OA on radiographs. In our initial study [15], we demonstrated the coronal dGEMRIC index best predicted pain improvement and lack of radiographic disease progression and avoidance of arthroplasty after PAO. We initially utilized just the coronal MRI cuts in our dGEMRIC assessment; however, we now recognize regional variations in the mechanical stress in the hip should lead to nonuniform degenerative changes. Since the damage is most severe in the anterior part of the joint, selective sagittal cuts may be a more sensitive predictor of outcome after PAO. Based on previous dGEMRIC studies, the coronal and sagittal slice dGEMRIC values would correlate to one another; however, we predict the anterior dGEMRIC index, which would have the most amount of damage, would best predict premature joint failure after osteotomy.
We therefore asked whether the regional variations in biochemical composition in cartilage in dysplastic hips predict failure based on pain and function, progression of apparent joint space loss, and subsequent THA after PAOs.
Patients and Methods
We retrospectively analyzed a subset of a cohort from a previously published prospective study [15]. The initial cohort consisted of 207 hips from 171 patients with DDH who underwent Bernese PAO procedures from October 1999 to November 2002. Inclusion criteria for the patients selected for this study were as follows. All patients were offered Bernese PAO, a redirectional PAO, for activity-related hip pain and radiographic evidence of acetabular dysplasia [12, 23]. Patients with only primary acetabular osteotomies were included. However, if patients previously had open reduction and intertrochanteric osteotomies before or at the time of the primary acetabular osteotomy, they were included. At the time of the surgery, all patients in the cohort were at least near skeletally maturity with closed triradiate cartilage. They needed to have hip flexion of greater than 90° and radiographic evidence of acetabular dysplasia, defined as a lateral center-edge angle (LCE) of less than 20°. Patients were excluded if they had an incongruous hip as seen on abduction/internal rotation pelvic radiographs or if there was evidence of arthritis of greater than Tönnis Grade 3 [70] on radiographs. Any hip dysplasia caused by neuromuscular disorder or skeletal dysplasia was also excluded. Of 52 hips from 47 patients who met the inclusion criteria for the previous study, only the hips with both preoperative coronal and sagittal dGEMRIC scans before undergoing Bernese PAO were included in this study [15]. The cohort for this study consisted of 43 hips from 41 patients (36 female, five male). Clinical and radiographic images were obtained before and after the PAO. The minimum followup was 24 months (mean, 32 months; range, 24–46 months). No patients were lost to followup. No patients were recalled specifically for this study; all data were obtained from medical records and radiographs. Our institutional review board approved this study, and the patients or their parents provided informed consent for the surgery.
Preoperative clinical assessments were made using WOMAC index [6] questionnaires. Pain score for each hip was the sum of the scores for the five questions in the pain assessment section.
Preoperatively, all patients had standing AP and false-profile radiographs obtained of the affected joint and a supine AP view of the pelvis with the hip maximally abducted and internally rotated. During postoperative followup scheduled for at least 6 months after the surgery, only the standing AP pelvis and false-profile views of the affected joint were obtained. On the AP pelvic film, two of us (SDK, RJ) measured the joint space width (JSW) as the minimum radial distance between the subchondral bone of the acetabulum and the femoral head in the weightbearing area [14]. The LCE angle was measured as the angle formed by a vertical line drawn through the center of the femoral head and a line drawn along the edge of the acetabulum on the AP pelvic radiograph [77]. Tönnis grade and Tönnis angle were measured on AP pelvic radiographs [70]. Joint subluxation was defined as a break in Shenton’s line of 5 mm or more [13]. Anterior center-edge (ACE) angle was measured using the false-profile view [34]. The von Rosen view (maximal abduction, internal rotation) was used to assess joint congruency preoperatively and postoperatively with AP pelvic radiographs using the classification of Yasunaga et al. [78]. The morphologic measurements are associated with high inter- and intrareader reliability with intraclass correlation coefficients ranging from 0.9 to 0.97 [18]. The JSW measurements are associated with inter- and intrareader intraclass coefficients of 0.68 to 0.86 [7].
The dGEMRIC scans were performed as described previously, but the current study included analysis of the multislice fast spin echo (FSE) sagittal slices with saturation recovery technique. The dGEMRIC scans were performed using a GE 1.5-T clinical scanner (General Electric Corp, Milwaukee, WI, USA). A double dose (0.4 mL/kg) of Magnevist® (gadolinium diethylene triamine pentaacetic acid [Gd-DTPA2−]; Bayer HealthCare, Wayne, NJ, USA) was injected intravenously. The patients were required to walk for 30 minutes before the scan to ensure full penetration of the gadolinium into the articular cartilage. The following imaging parameters were used: echo time of 14 milliseconds and repetition times of 300, 500, 750, 1000, 1500, and 2000 milliseconds [15, 31]. T1 value was calculated using custom Matlab® software (Mathworks, Natick, MA, USA) to perform a pixel-by-pixel fit of the image intensity of the six FSE image data to a rising exponential equation. Four coronal slices with 4-mm slice thickness and 1-mm spacing were obtained. Two to three sagittal slices were obtained with 3-mm thickness, 1-mm spacing, and in-plane resolution of ~ 0.7 mm. The T1 values of the femoral and acetabular cartilages were averaged to calculate the dGEMRIC index. On the coronal slices, the coronal dGEMRIC index of the weightbearing cartilage was calculated as the average T1 value of the femoral and acetabular cartilages from the lateral edge of the bony acetabulum to the edge of the acetabular fossa. On the sagittal slices, the anterior sagittal dGEMRIC index was calculated as the average T1 value of the femoral and acetabular cartilages from the anterior edge of the bony acetabulum to a vertical line going through the center of the head. The posterior sagittal dGEMRIC index was the average T1 value of the femoral and acetabular cartilages from the vertical line going through the center of the femoral head to an equal arc used to calculate the anterior sagittal dGEMRIC index. The sagittal dGEMRIC index was the average of the anterior and posterior sagittal dGEMRIC indexes.
Our routine clinical followups were performed at 1, 2, 3, 6, and 12 months and then yearly after the osteotomy. At each visit, an AP pelvic radiograph was obtained. Usually at either the 3- or 6-month visit, false-profile radiographs were obtained to assess the acetabular correction. At the 6-month and yearly visits, WOMAC score and detailed clinical hip ROM and examination were obtained. For longer-term followups, nine patients were interviewed over the telephone by trained research assistants or filled out the WOMAC questionnaires sent to them by mail. Additionally, some plain radiographs were obtained locally and sent to us for analysis.
The surgical intervention was deemed a failure if the patient required a THA during the followup period, had persistent postoperative WOMAC pain scores of greater than 10 points, or had minimal JSWs decreased to less than 3 mm. Among the 43 hips, five hips eventually required a THA during the followup period, and one hip had a decrease in JSW to less than 3 mm. The final study cohort consisted of two groups, one with 37 hips that underwent a successful pelvic osteotomy and the other with six hips for which the operation was deemed a failure (Table 1). All six patients whose osteotomy failed were women with a mean (± SD) age of 34 ± 7 years, compared to the patient population who had not failed by the criteria above (32 female, five male) with a mean age of 28 ± 11 years (p = 0.21) (Table 1). The mean differences between the PAO satisfactory and PAO failure groups were 5.9 years (95% CI, 2.0–13.0 years) for age, 5.4 points (95% CI, 2.0–9.0 points) for WOMAC pain score, −1.9 mm (95% CI, −1.0 to −3.0 mm) for JSW, −201 milliseconds (95% CI, −116 to −286 milliseconds) for coronal dGEMRIC index, and −261 milliseconds (95% CI, −154 to −367 milliseconds) for sagittal weightbearing dGEMRIC index.
We used Student’s t-test to assess differences in age, WOMAC scores, JSW, Tönnis angle, and dGEMRIC indexes measured preoperatively for patients whose hips were preserved at the time of last followup and those who failed. The nonparametric Mann-Whitney U test was used to compare LCE and ACE angles since these radiographic measurements did not follow a normal distribution and medians and interquartile ranges are reported. We used the Pearson chi-square test to compare ordinal data between the two groups including joint congruency and Tönnis grade and Fisher’s exact test to compare sex and left versus right side. Correlation between the coronal and sagittal dGEMRIC index values was measured using the Pearson product-moment correlation coefficient (r) with a fitted linear regression line and 95% CI for individual hips. In preparation for a multivariate analysis, a univariate analysis was performed to identify the relevant variables. Univariate analysis demonstrated preoperative pain, JSW, Tönnis grade, and coronal and sagittal dGEMRIC indexes were different between failed and preserved hips (Table 1). We used multivariable logistic regression analysis with backward stepwise selection to assess the influence of WOMAC pain, JSW, Tönnis grade, and different permutations of dGEMRIC indexes to control for confounding, with the goal of identifying independent predictors of failure after PAO using the likelihood ratio test (LRT) to assess level of significance. Receiver operating characteristic (ROC) curve analysis was utilized to evaluate the quality of outcome prediction using the dGEMRIC index with area under the curve (AUC) as a measure of accuracy and to determine an optimal cutoff value. We performed data analysis using the SPSS® package (Version 19.0; SPSS Inc, Chicago, IL, USA). Two-tailed values of p < 0.05 were considered significant.
Results
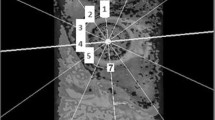
The mean dGEMRIC indexes of coronal images correlated (r = 0.742, r2 = 0.551, p < 0.001) with those of the sagittal images (Fig. 1). The mean dGEMRIC indexes of the average coronal (p < 0.001) and sagittal (p < 0.001) planes and their individual slices were lower in the prematurely failed group (Table 2). The sagittal slices were divided further into anterior and posterior weightbearing regions. The mean dGEMRIC indexes for both the anterior and posterior weightbearing regions also differed between the two groups, but the difference was greater in the posterior weightbearing region (Table 2). In particular, the posterior weightbearing region in the failed group had one of the lowest dGEMRIC indexes.

Sample (A) coronal and (B) sagittal dGEMRIC images are shown. (C) A graph shows the correlation of the average sagittal dGEMRIC index with the average coronal dGEMRIC index.
WOMAC pain (LRT = 5.28, p = 0.022) and sagittal anterior dGEMRIC index (LRT = 20.45, p < 0.0001) independently predicted failure after PAO. The other covariates tested provided no additional value in predicting failure (all p > 0.20). The predictive value of dGEMRIC can be best depicted by a graph showing the increased probability of failure after PAO with shorter sagittal anterior weightbearing dGEMRIC times (Fig. 2). For example, the theoretical probability of failure for a hip with a dGEMRIC of 250 milliseconds is 96% (95% CI, 63%–99%). ROC analysis revealed the sagittal anterior weightbearing dGEMRIC provided excellent discrimination between hips that failed after PAO and those having a satisfactory outcome with an AUC of 0.977 (95% CI, 0.938–1.000) (Fig. 3). The optimal cutoff value based on ROC analysis was 370 milliseconds, which was associated with a sensitivity of 100% (all six failures had values ≤ 370 milliseconds) and a specificity of 95% (35 of the 37 satisfactory outcomes were in hips with an average value > 370 milliseconds).

A graph shows the calculated theoretical probability of failure after PAO using the average sagittal anterior weightbearing dGEMRIC index. The probability of a failed PAO decreases sharply with increasing dGEMRIC time as illustrated by the curve. The dashed curves represent the 95% CI as an indication of precision of the estimated probability.

An ROC curve shows excellent discrimination of the average sagittal anterior weightbearing dGEMRIC in predicting failures (sensitivity) and nonfailures (specificity) after PAO. The optimal cutoff value is 370 milliseconds.
Discussion
At present, several different compositional MRIs are available, of which some have been validated in the clinical setting to detect early OA. dGEMRIC has been most frequently used in clinical studies, and we previously reported it predicts the need for early joint arthroplasty after Bernese PAOs. In this study, we presumed regional variations in mechanical stress in a dysplastic hip would lead to degenerative changes that are nonuniform. We believed identifying areas with the earliest cartilage damage could be used as an improved predictor over the dGEMRIC index on coronal slices and plain radiographic measure of OA.
Our study is associated with a number of limitations. First, our sample size was limited and especially the number of failures was small. In our prior study, the number of failures was larger; however, many did not have sagittal dGEMRIC scans and therefore were not used. This may explain why joint subluxation was no longer a predictor of premature joint failure. Similarly, the small number of failures will limit the validity of a multivariable analysis. Therefore, we would interpret our results as preliminary and encourage further work. Second, the length of followup in this study was short. We believe dGEMRIC is certainly a valuable predictor of short-term premature joint failure after PAO; however, further study is necessary to see whether dGEMRIC is a useful predictor of long-term joint preservation. Third, dGEMRIC is a new MRI technique unfamiliar to most imaging centers. To replicate our findings, familiarity with this imaging technique and the potential technical limitations is recommended.
Regional variations in biochemical content of cartilage have been described in other papers. In FAI, global arthritic changes were noted in pincer-type hips and more anterior and central in cam-type hips [38]. In patients with FAI, with or without symptoms of impingement, higher alpha angle correlated with reduced dGEMRIC index on the anterosuperior aspect of the hip and more globally in patients with FAI with signs of impingement [58]. Additionally, we know, in dysplastic hips, often the articular cartilage damage first occurs in the anterior portion of the acetabulum [66]. Our analysis of the individual slices of coronal and sagittal dGEMRIC indexes demonstrated the amount of degeneration in these individual areas correlated with overall lower dGEMRIC indexes. However, the damage was most noticeable in the anterior portion of the sagittal cuts, consistent with previously reported findings [53].
Given there is more extensive damage in the anterior portion of the acetabulum, we sought to know whether the dGEMRIC index in this region would best predict early joint failure after PAO. It was interesting, despite the facts that the posterior part of the joint had a larger difference in dGEMRIC index between the failed and successful group and that coronal and sagittal dGEMRIC values correlated to each other, multiple logistic regression models comparing these indexes revealed the sagittal anterior weightbearing region dGEMRIC index best predicted early joint failure. One explanation for this result could be the anteversion of the femoral head causing greater mechanical load in the anterior region of a dysplastic hip. Murphy et al. [48] reported variable amounts of acetabular deficiency in patients with dysplasia, with some having more global dysplasia and others with regional dysplasia. Additionally, the mechanical load and stressors of each individual’s hip are unique depending on the amount of version of the acetabulum and femoral head and the congruity. Perhaps even after acetabular redirection, the anterior part of the joint is still under higher mechanical load and hence excessive damage in this part of joint will lead to continued degeneration.
In summary, biochemical imaging can show early damage in the hip consistent with what we understand from the pathomechanics of hip deformity. In surgical correction of acetabular dysplasia, it appears dGEMRIC may have a role in selecting the right patient for treatment. Further work is needed to see whether other biochemical imaging techniques will have the same clinical value, especially in conditions such as FAI. The promise of a biochemical imaging technique is its potential to demonstrate, early after treatment, changes in cartilage health that may indicate a procedure may help preserve a joint for decades to come. Ultimately, that is the goal of joint preservation surgeries.
References
Akella SV, Regatte RR, Gougoutas AJ, Borthakur A, Shapiro EM, Kneeland JB, Leigh JS, Reddy R. Proteoglycan-induced changes in T1rho-relaxation of articular cartilage at 4T. Magn Reson Med. 2001;46:419–423.
Apprich S, Mamisch TC, Welsch GH, Stelzeneder D, Albers C, Totzke U, Trattnig S. Quantitative T2 mapping of the patella at 3.0T is sensitive to early cartilage degeneration, but also to loading of the knee. Eur J Radiol. 2012;81:e438–e443.
Aronson J. Osteoarthritis of the young adult hip: etiology and treatment. Instr Course Lect. 1986;35:119–128.
Bashir A, Gray ML, Hartke J, Burstein D. Nondestructive imaging of human cartilage glycosaminoglycan concentration by MRI. Magn Reson Med. 1999;41:857–865.
Beck M, Kalhor M, Leunig M, Ganz R. Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip. J Bone Joint Surg Br. 2005;87:1012–1018.
Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15:1833–1840.
Bittersohl B, Steppacher S, Haamberg T, Kim YJ, Werlen S, Beck M, Siebenrock KA, Mamisch TC. Cartilage damage in femoroacetabular impingement (FAI): preliminary results on comparison of standard diagnostic vs delayed gadolinium-enhanced magnetic resonance imaging of cartilage (dGEMRIC). Osteoarthritis Cartilage. 2009;17:1297–1306.
Broderick LS, Turner DA, Renfrew DL, Schnitzer TJ, Huff JP, Harris C. Severity of articular cartilage abnormality in patients with osteoarthritis: evaluation with fast spin-echo MR vs arthroscopy. AJR Am J Roentgenol. 1994;162:99–103.
Brooks PM. Impact of osteoarthritis on individuals and society: how much disability? Social consequences and health economic implications. Curr Opin Rheumatol. 2002;14:573–577.
Burstein D, Velyvis J, Scott KT, Stock KW, Kim YJ, Jaramillo D, Boutin RD, Gray ML. Protocol issues for delayed Gd(DTPA)(2−)-enhanced MRI (dGEMRIC) for clinical evaluation of articular cartilage. Magn Reson Med. 2001;45:36–41.
Clohisy JC, Barrett SE, Gordon JE, Delgado ED, Schoenecker PL. Periacetabular osteotomy for the treatment of severe acetabular dysplasia. J Bone Joint Surg Am. 2005;87:254–259.
Clohisy JC, Barrett SE, Gordon JE, Delgado ED, Schoenecker PL. Periacetabular osteotomy in the treatment of severe acetabular dysplasia: surgical technique. J Bone Joint Surg Am. 2006;88(suppl 1 pt 1):65–83.
Cooperman DR, Wallensten R, Stulberg SD. Acetabular dysplasia in the adult. Clin Orthop Relat Res. 1983;175:79–85.
Croft P, Cooper C, Wickham C, Coggon D. Defining osteoarthritis of the hip for epidemiologic studies. Am J Epidemiol. 1990;132:514–522.
Cunningham T, Jessel R, Zurakowski D, Millis MB, Kim YJ. Delayed gadolinium-enhanced magnetic resonance imaging of cartilage to predict early failure of Bernese periacetabular osteotomy for hip dysplasia. J Bone Joint Surg Am. 2006;88:1540–1548.
Dagher F, Ghanem I, Abiad R, Haykal G, Kharrat K, Phares A. [Bernese periacetabular osteotomy for the treatment of the degenerative dysplasic hip] [in French]. Rev Chir Orthop Reparatrice Appar Mot. 2003;89:125–133.
de Kleuver M, Kooijman MA, Pavlov PW, Veth RP. Triple osteotomy of the pelvis for acetabular dysplasia: results at 8 to 15 years. J Bone Joint Surg Br. 1997;79:225–229.
Dudda M, Kim YJ, Zhang Y, Nevitt MC, Xu L, Niu J, Goggins J, Doherty M, Felson DT. Morphologic differences between the hips of Chinese women and white women: could they account for the ethnic difference in the prevalence of hip osteoarthritis? Arthritis Rheum. 2011;63:2992–2999.
Dunn TC, Lu Y, Jin H, Ries MD, Majumdar S. T2 relaxation time of cartilage at MR imaging: comparison with severity of knee osteoarthritis. Radiology. 2004;232:592–598.
Duvvuri U, Reddy R, Patel SD, Kaufman JH, Kneeland JB, Leigh JS. T1rho-relaxation in articular cartilage: effects of enzymatic degradation. Magn Reson Med. 1997;38:863–867.
Felson DT. Validating markers in osteoarthritis. Acta Orthop Scand Suppl. 1995;266:205–207.
Felson DT, Zhang Y. An update on the epidemiology of knee and hip osteoarthritis with a view to prevention. Arthritis Rheum. 1998;41:1343–1355.
Ganz R, Klaue K, Vinh TS, Mast JW. A new periacetabular osteotomy for the treatment of hip dysplasias: technique and preliminary results. Clin Orthop Relat Res. 1988;232:26–36.
Gillis A, Bashir A, McKeon B, Scheller A, Gray ML, Burstein D. Magnetic resonance imaging of relative glycosaminoglycan distribution in patients with autologous chondrocyte transplants. Invest Radiol. 2001;36:743–748.
Gold GE, Thedens DR, Pauly JM, Fechner KP, Bergman G, Beaulieu CF, Macovski A. MR imaging of articular cartilage of the knee: new methods using ultrashort TEs. AJR Am J Roentgenol. 1998;170:1223–1226.
Harris WH. Etiology of osteoarthritis of the hip. Clin Orthop Relat Res. 1986;213:20–33.
Hasegawa Y, Iwase T, Kitamura S, Yamauchi Ki K, Sakano S, Iwata H. Eccentric rotational acetabular osteotomy for acetabular dysplasia: follow-up of one hundred and thirty-two hips for five to ten years. J Bone Joint Surg Am. 2002;84:404–410.
Hipp JA, Sugano N, Millis MB, Murphy SB. Planning acetabular redirection osteotomies based on joint contact pressures. Clin Orthop Relat Res. 1999;364:134–143.
Jessel RH, Zilkens C, Tiderius C, Dudda M, Mamisch TC, Kim YJ. Assessment of osteoarthritis in hips with femoroacetabular impingement using delayed gadolinium enhanced MRI of cartilage. J Magn Reson Imaging. 2009;30:1110–1115.
Keenan KE, Besier TF, Pauly JM, Han E, Rosenberg J, Smith RL, Delp SL, Beaupre GS, Gold GE. Prediction of glycosaminoglycan content in human cartilage by age, T1rho and T2 MRI. Osteoarthritis Cartilage. 2011;19:171–179.
Kim YJ, Jaramillo D, Millis MB, Gray ML, Burstein D. Assessment of early osteoarthritis in hip dysplasia with delayed gadolinium-enhanced magnetic resonance imaging of cartilage. J Bone Joint Surg Am. 2003;85:1987–1992.
Koff MF, Amrami KK, Kaufman KR. Clinical evaluation of T2 values of patellar cartilage in patients with osteoarthritis. Osteoarthritis Cartilage. 2007;15:198–204.
Kralj M, Mavcic B, Antolic V, Iglic A, Kralj-Iglic V. The Bernese periacetabular osteotomy: clinical, radiographic and mechanical 7–15-year follow-up of 26 hips. Acta Orthop. 2005;76:833–840.
Lequesne M, de Séze S. [False profile of the pelvis: a new radiographic incidence for the study of the hip. Its use in dysplasias and different coxopathies] [in French]. Rev Rhum Mal Osteoartic. 1961;28:643–652.
Li X, Benjamin Ma C, Link TM, Castillo DD, Blumenkrantz G, Lozano J, Carballido-Gamio J, Ries M, Majumdar S. In vivo T(1rho) and T(2) mapping of articular cartilage in osteoarthritis of the knee using 3 T MRI. Osteoarthritis Cartilage. 2007;15:789–797.
Li X, Cheng J, Lin K, Saadat E, Bolbos RI, Jobke B, Ries MD, Horvai A, Link TM, Majumdar S. Quantitative MRI using T1rho and T2 in human osteoarthritic cartilage specimens: correlation with biochemical measurements and histology. Magn Reson Imaging. 2011;29:324–334.
Mamisch TC, Dudda M, Hughes T, Burstein D, Kim YJ. Comparison of delayed gadolinium enhanced MRI of cartilage (dGEMRIC) using inversion recovery and fast T1 mapping sequences. Magn Reson Med. 2008;60:768–773.
Mamisch TC, Kain MS, Bittersohl B, Apprich S, Werlen S, Beck M, Siebenrock KA. Delayed gadolinium-enhanced magnetic resonance imaging of cartilage (dGEMRIC) in femoacetabular impingement. J Orthop Res. 2011;29:1305–1311.
Mamisch TC, Menzel MI, Welsch GH, Bittersohl B, Salomonowitz E, Szomolanyi P, Kordelle J, Marlovits S, Trattnig S. Steady-state diffusion imaging for MR in-vivo evaluation of reparative cartilage after matrix-associated autologous chondrocyte transplantation at 3 tesla–preliminary results. Eur J Radiol. 2008;65:72–79.
Mamisch TC, Trattnig S, Quirbach S, Marlovits S, White LM, Welsch GH. Quantitative T2 mapping of knee cartilage: differentiation of healthy control cartilage and cartilage repair tissue in the knee with unloading—initial results. Radiology. 2010;254:818–826.
Matheney T, Kim YJ, Zurakowski D, Matero C, Millis M. Intermediate to long-term results following the Bernese periacetabular osteotomy and predictors of clinical outcome. J Bone Joint Surg Am. 2009;91:2113–2123.
McKenzie CA, Williams A, Prasad PV, Burstein D. Three-dimensional delayed gadolinium-enhanced MRI of cartilage (dGEMRIC) at 1.5T and 3.0T. J Magn Reson Imaging. 2006;24:928–933.
Menezes NM, Gray ML, Hartke JR, Burstein D. T2 and T1rho MRI in articular cartilage systems. Magn Reson Med. 2004;51:503–509.
Mosher TJ, Dardzinski BJ. Cartilage MRI T2 relaxation time mapping: overview and applications. Semin Musculoskelet Radiol. 2004;8:355–368.
Mosher TJ, Dardzinski BJ, Smith MB. Human articular cartilage: influence of aging and early symptomatic degeneration on the spatial variation of T2—preliminary findings at 3 T. Radiology. 2000;214:259–266.
Multanen J, Rauvala E, Lammentausta E, Ojala R, Kiviranta I, Hakkinen A, Nieminen MT, Heinonen A. Reproducibility of imaging human knee cartilage by delayed gadolinium-enhanced MRI of cartilage (dGEMRIC) at 1.5 Tesla. Osteoarthritis Cartilage. 2009;17:559–564.
Murphy S, Deshmukh R. Periacetabular osteotomy: preoperative radiographic predictors of outcome. Clin Orthop Relat Res. 2002;405:168–174.
Murphy SB, Kijewski PK, Millis MB, Harless A. Acetabular dysplasia in the adolescent and young adult. Clin Orthop Relat Res. 1990;261:214–223.
Nag D, Liney GP, Gillespie P, Sherman KP. Quantification of T(2) relaxation changes in articular cartilage with in situ mechanical loading of the knee. J Magn Reson Imaging. 2004;19:317–322.
Nakamura S, Ninomiya S, Takatori Y, Morimoto S, Umeyama T. Long-term outcome of rotational acetabular osteotomy: 145 hips followed for 10–23 years. Acta Orthop Scand. 1998;69:259–265.
Neuman P, Tjornstrand J, Svensson J, Ragnarsson C, Roos H, Englund M, Tiderius CJ, Dahlberg LE. Longitudinal assessment of femoral knee cartilage quality using contrast enhanced MRI (dGEMRIC) in patients with anterior cruciate ligament injury–comparison with asymptomatic volunteers. Osteoarthritis Cartilage. 2011;19:977–983.
Nishii T, Kuroda K, Matsuoka Y, Sahara T, Yoshikawa H. Change in knee cartilage T2 in response to mechanical loading. J Magn Reson Imaging. 2008;28:175–180.
Nishii T, Tanaka H, Sugano N, Miki H, Takao M, Yoshikawa H. Disorders of acetabular labrum and articular cartilage in hip dysplasia: evaluation using isotropic high-resolutional CT arthrography with sequential radial reformation. Osteoarthritis Cartilage. 2007;15:251–257.
Nishii T, Tanaka H, Sugano N, Sakai T, Hananouchi T, Yoshikawa H. Evaluation of cartilage matrix disorders by T2 relaxation time in patients with hip dysplasia. Osteoarthritis Cartilage. 2008;16:227–233.
Nozawa M, Shitoto K, Matsuda K, Maezawa K, Kurosawa H. Rotational acetabular osteotomy for acetabular dysplasia: a follow-up for more than ten years. J Bone Joint Surg Br. 2002;84:59–65.
Parker DA, Beatty KT, Giuffre B, Scholes CJ, Coolican MR. Articular cartilage changes in patients with osteoarthritis after osteotomy. Am J Sports Med. 2011;39:1039–1045.
Pogliacomi F, Stark A, Wallensten R. Periacetabular osteotomy: good pain relief in symptomatic hip dysplasia, 32 patients followed for 4 years. Acta Orthop. 2005;76:67–74.
Pollard TC, McNally EG, Wilson DC, Wilson DR, Madler B, Watson M, Gill HS, Carr AJ. Localized cartilage assessment with three-dimensional dGEMRIC in asymptomatic hips with normal morphology and cam deformity. J Bone Joint Surg Am. 2010;92:2557–2569.
Regatte RR, Akella SV, Borthakur A, Kneeland JB, Reddy R. Proteoglycan depletion-induced changes in transverse relaxation maps of cartilage: comparison of T2 and T1rho. Acad Radiol. 2002;9:1388–1394.
Regatte RR, Akella SV, Lonner JH, Kneeland JB, Reddy R. T1rho relaxation mapping in human osteoarthritis (OA) cartilage: comparison of T1rho with T2. J Magn Reson Imaging. 2006;23:547–553.
Roos EM, Dahlberg L. Positive effects of moderate exercise on glycosaminoglycan content in knee cartilage: a four-month, randomized, controlled trial in patients at risk of osteoarthritis. Arthritis Rheum. 2005;52:3507–3514.
Schramm M, Pitto RP, Bar K, Meyer M, Rohm E, Hohmann D. Prophylaxis of secondary osteoarthrosis with spherical osteotomy in residual acetabular dysplasia. Analysis of predictive factors of success. Arch Orthop Trauma Surg. 1999;119:418–422.
Smith HE, Mosher TJ, Dardzinski BJ, Collins BG, Collins CM, Yang QX, Schmithorst VJ, Smith MB. Spatial variation in cartilage T2 of the knee. J Magn Reson Imaging. 2001;14:50–55.
Solomon L. Patterns of osteoarthritis of the hip. J Bone Joint Surg Br. 1976;58:176–183.
Steppacher SD, Tannast M, Ganz R, Siebenrock KA. Mean 20-year followup of Bernese periacetabular osteotomy. Clin Orthop Relat Res. 2008;466:1633–1644.
Tamura S, Nishii T, Shiomi T, Yamazaki Y, Murase K, Yoshikawa H, Sugano N. Three-dimensional patterns of early acetabular cartilage damage in hip dysplasia; a high-resolutional CT arthrography study. Osteoarthritis Cartilage. 2012;20:646–652.
Tiderius CJ, Jessel R, Kim YJ, Burstein D. Hip dGEMRIC in asymptomatic volunteers and patients with early osteoarthritis: the influence of timing after contrast injection. Magn Reson Med. 2007;57:803–805.
Tiderius CJ, Olsson LE, Leander P, Ekberg O, Dahlberg L. Delayed gadolinium-enhanced MRI of cartilage (dGEMRIC) in early knee osteoarthritis. Magn Reson Med. 2003;49:488–492.
Tiderius CJ, Svensson J, Leander P, Ola T, Dahlberg L. dGEMRIC (delayed gadolinium-enhanced MRI of cartilage) indicates adaptive capacity of human knee cartilage. Magn Reson Med. 2004;51:286–290.
Tönnis D. Congenital Dysplasia and Dislocation of the Hip in Children and Adults. New York, NY: Springer; 1987.
Tönnis D, Heinecke A. Acetabular and femoral anteversion: relationship with osteoarthritis of the hip. J Bone Joint Surg Am. 1999;81:1747–1770.
Trattnig S, Welsch GH, Juras V, Szomolanyi P, Mayerhoefer ME, Stelzeneder D, Mamisch TC, Bieri O, Scheffler K, Zbyn S. 23Na MR imaging at 7 T after knee matrix-associated autologous chondrocyte transplantation preliminary results. Radiology. 2010;257:175–184.
Trousdale RT, Ekkernkamp A, Ganz R, Wallrichs SL. Periacetabular and intertrochanteric osteotomy for the treatment of osteoarthrosis in dysplastic hips. J Bone Joint Surg Am. 1995;77:73–85.
Venn M, Maroudas A. Chemical composition and swelling of normal and osteoarthrotic femoral head cartilage. I. Chemical composition. Ann Rheum Dis. 1977;36:121–129.
Welsch GH, Trattnig S, Domayer S, Marlovits S, White LM, Mamisch TC. Multimodal approach in the use of clinical scoring, morphological MRI and biochemical T2-mapping and diffusion-weighted imaging in their ability to assess differences between cartilage repair tissue after microfracture therapy and matrix-associated autologous chondrocyte transplantation: a pilot study. Osteoarthritis Cartilage. 2009;17:1219–1227.
Wheaton AJ, Casey FL, Gougoutas AJ, Dodge GR, Borthakur A, Lonner JH, Schumacher HR, Reddy R. Correlation of T1rho with fixed charge density in cartilage. J Magn Reson Imaging. 2004;20:519–525.
Wiberg G. Studies on dysplastic acetabula and congenital subluxation of the hip joint: with special reference to the complication of osteo-arthritis. Acta Chir Scand. 1939;83(suppl 58):5–135.
Yasunaga Y, Takahashi K, Ochi M, Ikuta Y, Hisatome T, Nakashiro J, Yamamoto S. Rotational acetabular osteotomy in patients forty-six years of age or older: comparison with younger patients. J Bone Joint Surg Am. 2003;85:266–272.
Zilkens C, Miese F, Bittersohl B, Jager M, Schultz J, Holstein A, Kim YJ, Millis MB, Mamisch TC, Krauspe R. Delayed gadolinium-enhanced magnetic resonance imaging of cartilage (dGEMRIC), after slipped capital femoral epiphysis. Eur J Radiol. 2011;79:400–406.
Acknowledgments
We thank Cathy Matero for her assistance in organizing the data and contacting the patients.
Author information
Authors and Affiliations
Corresponding author
Additional information
The institution of one or more of the authors (RJ, MBM, YJK) has received, during the study period, funding from the Orthopaedic Research and Education Foundation (Rosemont, IL, USA).
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
Appendix 1
Appendix 1
MRI Techniques for Cartilage
Biochemical or compositional MRI techniques for cartilage hold the promise of detecting cartilage damage before irreversible structural damage occurs. At present, there are five techniques designed to probe different macromolecular components of the cartilage matrix: dGEMRIC, sodium MRI, diffusion-weighted imaging, T2 mapping, and T1ρ. Each technique has its own advantages and challenges to practical clinical application. The following is a brief synopsis of the most relevant biochemical imaging techniques for cartilage.
dGEMRIC is a contrast-based technique designed to specifically detect the loss of sulfated glycosaminoglycan (GAG) of articular cartilage. The MRI is performed after an intravenous or intraarticular injection of an anionic contrast agent chelate Gd-DTPA2−. This contrast agent is allowed sufficient time to partition into the cartilage before imaging is started. Because the contrast agent is negatively charged, it will partition into the articular cartilage in an inversely proportional manner. By quantitating the amount of contrast agent in cartilage using MRI, the charge density of cartilage can be calculated or inferred. This technique is highly specific for GAG loss in cartilage, mainly due to the use of a negatively charged contrast agent. However, the need for contrast injection poses challenges, which include the need for delay between contrast injection and imaging, need for a specific exercise protocol to facilitate contrast penetration into cartilage, and the risk of contrast reaction. Recently, concern has been raised with the use of contrast agents in patients with poor renal function due to the risk of developing nephrogenic systemic sclerosis, which is a rare and sometimes fatal syndrome. Despite these challenges, if the issues regarding timing of the scan after contrast administration [67] and exercise protocol [46] are respected, reproducible quantitative results can be obtained with a root-mean-square average coefficient of variation of less than 10%. Additionally, validated fast T1 mapping sequences are available so imaging times around 5 minutes are now feasible [37]. In addition to the hip studies outlined previously, multiple clinical studies have been performed using dGEMRIC, demonstrating the effect of exercise on knee cartilage [69], reconstitution of a more normal cartilage after autologous chondrocyte transplantation [24], and perhaps preservation of cartilage after high tibial osteotomy for knee osteoarthritis [56].
The main advantage of dGEMRIC is its specificity for assessing cartilage charge density. Similar specificity is possible but without the need for contrast injection using sodium MRI. In sodium MRI, instead of using gadolinium as the probe, sodium itself is used as the probe to measure charge density. Unlike the typical proton MRI, the nuclear spin momentum of the positively charged sodium ions is used to generate the MRI signal. However, due to the fact that there are far fewer sodium atoms in the body than water, sodium MRI requires minimum 3-T or higher field strength magnets, specialized hardware, and radiofrequency coils. At present, its use has been limited to strictly research purposes, although use of sodium MRI at 7 T was recently published and correlated with dGEMRIC after matrix-associated autologous chondrocyte transplantation [72]. In the future, widespread availability of high-field scanners may make this technique practical.
Some of the other noncontrast MRI techniques include diffusion-weighted MRI, which measures the diffusion characteristics of water molecules in tissue. The diffusivity of water is affected by intracellular and extracellular barriers and is most commonly utilized to detect early central nervous system cell necrosis. It can also provide information regarding the macromolecular environment, which includes GAG and collagen, as well as tissue ultrastructure. It is an attractive technique in the clinical setting because images can be obtained without contrast injection and scan times are relatively quick. However, it is sensitive to motion artifacts, and it is demanding to get absolute quantitative measurements. It has been utilized for evaluation of patients after matrix-associated autologous chondrocyte transplantation to show distinction between healthy cartilage and cartilage repair tissue, but it has had limited use in other clinical settings to evaluate cartilage [39, 75].
T2 mapping, like diffusion-weighted imaging, does not require contrast injection and scan times are relatively short. It assesses interactions between water and collagen fibers to quantify water content and collagen anisotropy [44]. High anisotropy of highly organized collagen will lead to shortened T2 relaxation times. Hence, T2 relaxation times vary from low in the deep layers to higher values in the transitional layers of cartilage due to anisotropy of collagen fibers, which in the deep layers is high with dense collagen matrix and low in the transitional layers [45, 63]. Additionally, disruption of collagen fiber matrices and increase in water content as a result of cartilage damage will increase T2 relaxation times [19, 25]. Areas of high T2 relaxation times in osteoarthritic knees correlate with findings by arthroscopy [8]. However, there are concerns that there is no linear relationship of T2 mapping with severity of osteoarthritis [32]. Nishii et al. [54] compared T2 values and distribution in normal volunteers and patients with hip dysplasia; graded plain radiographs into normal, prearthritic, and mildly arthritic hips; and found no difference in T2 relaxation times among the different radiographic grades. T2 mapping is also sensitive to the loading state of the joint, which may alter T2 signal independent of cartilage damage if joint unloading before scanning is not controlled [2, 40, 49, 52]. Finally, T2 values are sensitive to the orientation of the collagen fibers relative to the B0 magnetic field due to the magic angle effect. In a spherical structure such as the hip, this will need to be taken into account when interpreting the T2 mapping data.
The T1ρ technique is a noncontrast technique that detects low-frequency interactions between water molecules and macromolecular protons. This may allow T1ρ maps in cartilage to be more specific than T2 in assessing GAG loss; however, there is debate and conflicting data regarding this characteristic of T1ρ measurement in cartilage. Some studies have shown T1ρ is sensitive to both proteoglycan and/or collagen content [1, 20, 43]. T1ρ relaxation times have been shown in vivo to correlate with severity of radiographic and MR grading of osteoarthritis [35]. Other studies have shown T1ρ is specific to GAG loss [36, 59, 76]. The most recent study by Keenan et al. [30] found T2 and T1ρ values correlated, and when T2 effects were isolated by looking at tissue only with T2 within normal range, T1ρ correlated with GAG content. They concluded T2 relaxation time should be incorporated into a predictive model when using T1ρ data to estimate GAG content. Comparing T1ρ with T2 mapping, Regatte et al. [60] suggested T1ρ had higher dynamic range, which allowed greater accuracy than T2 mapping. Disadvantages of T1ρ mapping include the length of time required to obtain the multiple data sets and the requirement for the spin lock pulse may increase the specific absorption rate. Although to a lesser extent than T2 mapping, the magic angle effect is also observed in T1ρ [36].
At present, many of these biochemical MRI techniques hold the promise of improving diagnostics and patient management for clinical problems. Although each technique has its own challenges and limitations, the true value of these techniques will not be known until well-performed clinical studies demonstrate their value in the clinical setting.
About this article
Cite this article
Kim, S.D., Jessel, R., Zurakowski, D. et al. Anterior Delayed Gadolinium-enhanced MRI of Cartilage Values Predict Joint Failure After Periacetabular Osteotomy. Clin Orthop Relat Res 470, 3332–3341 (2012). https://doi.org/10.1007/s11999-012-2519-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-012-2519-9