
Abstract
Background
Carpal tunnel syndrome (CTS) is a common complication in patients receiving long-term hemodialysis. In the short-term however, these patients are less likely to have pain relief and restoration of function after carpal tunnel release. However, it is unclear whether patients who have release for hemodialysis-associated CTS have differing persisting relief of symptoms compared with patients with idiopathic CTS.
Questions/purposes
We therefore compared (1) the severity of pain and level of function in patients who had release for hemodialysis-associated CTS with scores of patients who had release for idiopathic CTS, and (2) the operation-related complications.
Methods
We retrospectively reviewed 36 patients with CTS who were receiving hemodialysis and 54 patients with idiopathic CTS. Control subjects were matched for age, gender, and symptom severity. We obtained Boston Carpal Tunnel Questionnaire (BCTQ) scores preoperatively and at each followup. The minimum followup was 24 months (mean, 44.3 months; range, 24–90 months), although all comparisons were made at 2 years.
Results
Two years after carpal tunnel release, the mean BCTQ-symptom (S) /BCTQ-function (F) scores improved from 3.3/2.1 to 2.1/2.1 in the hemodialysis-associated CTS group and from 3.2/2.3 to 1.4/1.4 in the idiopathic CTS group. All but six patients receiving hemodialysis had lower (better) BCTQ-S scores than their initial scores. Four patients had complications, all with hemodialysis-associated CTS: two had revision carpal tunnel releases and two had delayed wound healing. We observed no arteriovenous fistula-related complication.
Conclusions
Patients with hemodialysis-associated CTS seem to remain impaired, unlike patients with idiopathic CTS, but the majority of them might have much improved CTS-related symptoms at 2 years after carpal tunnel release.
Level of Evidence
Level III, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
CTS is a common complication in patients undergoing long-term hemodialysis [5, 6, 8–10, 18]. The prevalence of CTS correlates with the duration of hemodialysis [5, 8], and CTS reportedly affects 32% to 50% of patients more than 10 years after the start of hemodialysis [8, 14] and 80% over 30 years [14]. The reasons why patients receiving long-term hemodialysis have CTS develop are unclear. Several factors have been suggested to play a role in inducing CTS in patients receiving long-term hemodialysis, including venous hypertension distal to the sites of vascular access, increased extracellular fluid volume, thickening of the transverse retinacular ligament, flexor tenosynovitis, β2 microglobulin amyloid deposition, and arterial steal syndrome [5–7, 10, 13].
Surgical release of the transverse carpal ligament is commonly performed in patients with severe symptoms of hemodialysis-associated CTS [6, 9, 13, 15–18]. Approximately 5% of patients receiving hemodialysis have reported a history of carpal tunnel release [16]. Several studies showed that patients with hemodialysis-associated CTS have less relief of symptoms after surgical release than those with idiopathic CTS [9, 11] and that their symptoms recur frequently, with rates ranging from 4.2% to 46.7% after carpal tunnel release [6, 9, 11, 17]. However, these observations are largely based on assessments by tools that have not been standardized, proven reproducible, validated, or responsive to clinical changes, and the studies reported variable followup periods ranging from a mean of 11.7 to 33 months [6, 9, 11, 13, 17]. Although CTS is common in patients receiving long-term hemodialysis, the available literature does not confirm whether patients with hemodialysis-associated CTS do worse than those with idiopathic CTS.
The purposes of this study were twofold: (1) to compare the pain and function in patients with hemodialysis-associated CTS with those of carpal tunnel release in patients with idiopathic CTS at 2 years after carpal tunnel release; and (2) to compare the operation-related complications after carpal tunnel release in patients with hemodialysis-associated and idiopathic CTS.
Patients and Methods
From January 2003 and July 2008, we treated 236 patients who underwent carpal tunnel release for CTS. Of these, 36 patients with end-stage renal disease (ESRD) had hemodialysis-associated CTS (HD-CTS group); they were matched with 54 patients with idiopathic CTS (I-CTS). CTS was diagnosed with clinical symptoms and signs and positive electrophysiologic findings [2]. Surgical indications included failed nonoperative treatment more than 3 months, clinical evidence of median nerve denervation like thenar muscle atrophy or weakness, and the patient’s decision to directly undergo surgical treatment. For this study we excluded 93 patients with (1) a history of pregnancy, trauma, or previous carpal tunnel release (n = 8); (2) an associated disease that might affect outcome such as diabetes mellitus, hypothyroidism, rheumatoid arthritis, cervical radiculopathy, other peripheral nerve entrapments, except ESRD (n = 17); (3) other associated tenosynovitis of the same hand such as trigger finger or de Quervain disease (n = 21); or (4) inadequate followup (less than 24 months) (n = 47). The minimum followup was 24 months (mean, 44.3 months; range, 24–90 months) although all postoperative comparisons were made only at 24 months for consistency. No patients were recalled specifically for this study; all data were obtained from medical records and radiographs. Prior Institutional Review Board approval was obtained for our study.
All of the patients with hemodialysis-associated CTS were right-handed. There were eight men and 28 women with a mean age of 59.8 years (range, 44–80 years). The right hand was involved in 20 patients and the left in 24. A functioning arteriovenous fistula (AVF) was located on the right forearm in 14 patients and the left in 22 patients. Four patients also had an obstructed AVF on the left forearm. The mean duration of hemodialysis was 15.5 years (range, 8–26 years). The mean time from the onset of CTS symptoms to carpal tunnel release was 18.0 months (range, 6–60 months).
We matched the comparison group of patients with idiopathic CTS by gender, age, and symptom severity. To match age, we used a 5-year age band to select control subjects. We did not include left-handed patients. To match symptom severity, we chose patients with idiopathic CTS whose difference in the BCTQ-S score was less than 0.5 among the age-matched patients in the I-CTS group The I-CTS group included 54 patients with 11 men and 43 women and a mean age of 59.2 years (range, 45–76 years). The mean time from the onset of CTS symptoms to carpal tunnel release was 34.4 months (range, 8–120 months). Among our study population, eight patients with hemodialysis-associated CTS and 12 patients with idiopathic CTS had carpal tunnel release on both hands; however, we analyzed only the dominant hands in these patients (Table 1).
The mean duration of symptoms before surgery was shorter in the HD-CTS group than in the I-CTS group: 18.0 months versus 34.4 months, respectively (Table 1). The mean preoperative BCTQ-S score (95% CI) and BCTQ-F score (95% CI) were 3.3 (3.1–3.5) and 2.1 (1.8–2.4) in the HD-CTS group and 3.2 (3.1–3.3) and 2.3 (2.1–2.4) in the I-CTS group. These scores mean that the patients with hemodialysis-associated CTS experienced an abrupt increase of symptoms in a relatively short time compared with patients with I-CTS (p = 0.009).
Surgery was performed by the senior author (SBH). The patient was placed under general or regional anesthesia and positioned in the supine position with the affected arm supported by a hand table. For patients with hemodialysis-associated CTS and an ipsilateral AVF, a sterile 1-inch tourniquet was applied just proximal to the wrist crease to prevent AVF obstruction (a complication that could happen with the use of a standard pneumatic tourniquet proximal to the AVF site). For all other patients, a standard pneumatic tourniquet was applied at the upper arm. For all patients, we used the limited open approach to release the transverse carpal ligament as previously described [4, 15]. We made a longitudinal incision from Kaplan’s cardinal line, 3 to 4 mm ulnar to and parallel with the thenar crease, 3 cm long toward the ulnar border of the palmaris longus tendon. We bluntly dissected the subcutaneous tissues and exposed the transverse carpal ligament. The proximal edge of the ligament was incised carefully, and a blunt probe was inserted to protect the underlying median nerve while the ligament was divided under direct vision using scissors. Because hypertrophic tenosynovitis was identified in seven hands of five patients with hemodialysis-associated CTS, we simultaneously performed a tenosynovectomy. None of the patients with idiopathic CTS had tenosynovectomy in our series. The tourniquet then was deflated, and meticulous hemostasis was established.
Postoperative splints were not used, and all patients were instructed in performing ROM exercises for the fingers and wrist. The sutures were removed 2 weeks postoperatively. Manual scar massage then was encouraged for scar desensitization and to decrease scar adhesion to the underlying tissues. At 4 to 6 weeks after surgery, patients were allowed to return to work with a 2-pound weight restriction, and at 6 to 8 weeks after surgery, they were allowed full activities without restrictions.
Postoperatively, patients were followed up in the outpatient clinic at 2 weeks, 6 weeks, 3 months, 6 months, and annually thereafter. The symptoms and functional status were assessed before surgery and at each followup. One observer (BRK) not involved in the treatment evaluated the symptoms and functional status of patients preoperatively and at each followup with the BCTQ [1, 3, 12]. The BCTQ is a disease-specific, self-administrated, and patient-based questionnaire that incorporates a symptom severity scale and a functional status scale. The BCTQ was introduced in 1993 and has become a well-recognized and validated outcome assessment tool for CTS [12]. The symptom severity (BCTQ-S) scale is comprised of 11 items that address symptom severity, frequency, and duration of symptoms, whereas the functional status (BCTQ-F) scale is comprised of eight questions that assess the difficulty of performing eight daily tasks. Each question offers five possible responses of increasing severity that are scored from 1 (none) to 5 (most severe); that is, a lower score means less pain and better function. We calculated the mean values of all items in the BCTQ. If a patient had recurrent CTS symptoms after carpal tunnel release, the patient was asked the duration of the symptom-free period.
We evaluated the difference between preoperative and postoperative BCTQ scores in each group using the paired t-test and compared preoperative and postoperative BCTQ scores between the two groups using the independent t-test. The chi-square test was used to compare the incidence of complications between the two groups. We used SPSS Version 18.0 (SPSS, Inc, Chicago, IL, USA) for statistical analyses.
Results
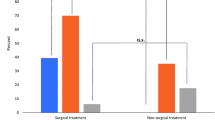
Two years after carpal tunnel release, the mean BCTQ-S score (95% CI) and BCTQ-F score (95% CI) improved to 2.1 (range, 1.8–2.5) and 2.1 (range, 1.8–2.4) in the HD-CTS group and 1.4 (range, 1.3–1.5) and 1.4 (range, 1.3–1.5) in the I-CTS group (Table 2). The patients receiving hemodialysis had higher (p < 0.001) BCTQ-S scores and BCTQ-F scores than the patients with idiopathic CTS. All but six patients with hemodialysis-associated CTS had lower BCTQ-S scores at 2 years followup than the score measured before surgery. In contrast, all patients with idiopathic CTS had lower BCTQ-S scores.
Four patients in the HD-CTS group had complications: two had delayed wound healing and two had revision carpal tunnel release at 15 and 21 months after the index carpal tunnel release resulting from recurrent symptoms. The patients who underwent revision surgery had symptomatic improvement but residual symptoms at last followup (8 and 13 months after revision surgery). No patient reported AVF-related complications after carpal tunnel release.
Discussion
CTS occurs in approximately 10% of patients receiving long-term hemodialysis, a much higher incidence than for idiopathic CTS in the general population [6]. Furthermore, the prevalence of CTS correlates with the duration of hemodialysis [5, 8, 14]. Although these patients are likely to have less favorable symptoms and functional status after carpal tunnel release, it is unclear if patients who have release for hemodialysis-associated CTS have differing long-term relief of symptoms compared with patients with idiopathic CTS. We therefore compared (1) the BCTQ scores and (2) the operation-related complications in patients who had carpal tunnel release for hemodialysis-associated CTS with those of patients who had release for idiopathic CTS.
There are several limitations to this study. First, this was a retrospective case-control study that compared the symptoms and functional status of carpal tunnel release between patients with hemodialysis-associated CTS and idiopathic CTS. Because we matched patients in the control group for age, gender, and diseased hand with patients in the hemodialysis-associated CTS group, the control group may not truly represent the general population of patients with idiopathic CTS. Second, we compared only the symptoms and functional status at 2 years after surgery in both groups. The short-term outcomes of carpal tunnel release are beyond the scope of this study. In addition, several studies have described relief of CTS symptoms with short-term followup after carpal tunnel release in patients with hemodialysis-associated CTS [6, 13, 17]. Third, we performed flexor tenosynovectomy in only five patients (seven hands) with hypertrophic tenosynovitis in hemodialysis-associated CTS. Therefore, the efficacy of tenosynovectomy in relieving symptoms or recurrence cannot be evaluated by the findings of our study. In addition, we did not control whether tenosynovectomy was performed when matching the comparison group of patients with idiopathic CTS because tenosynovectomy rarely is needed in this group of patients.
Despite surgical release of the transverse carpal ligament being common in patients with severe symptoms of CTS, few clinical studies with adequate followup periods have assessed patients receiving long-term hemodialysis with a validated assessment. According to previously published studies [6, 11, 13, 17], improvement of CTS symptoms rates from 53.3% to 95.8% and the duration of hemodialysis and CTS symptoms are likely to be important factors determining recovery from CTS symptoms after carpal tunnel release (Table 3). However, these studies are based largely on assessments by tools that have not been standardized, proven reproducible, validated, or responsive to clinical changes. Furthermore, three of these articles included data from patients who had only very short-term followup of 2 or 6 months [6, 13, 17]. We compared the scores of the BCTQ, a well-recognized and validated outcome assessment tool for CTS, in patients with hemodialysis-associated CTS with those of carpal tunnel release in patients with idiopathic CTS at 2 years after carpal tunnel release. Patients with hemodialysis-associated CTS had improved (lower) BCTQ symptom scores in comparison to their preoperative symptom scores, although their scores were much higher than those for patients with idiopathic CTS at 2 years after carpal tunnel release. Approximately 83.3% of our patients with hemodialysis-associated CTS reported improvement of CTS symptoms compared with their initial symptoms. Two previous studies considered flexor tenosynovectomy for patients with severe flexor tenosynovitis at the time of carpal tunnel release [6, 9]. One of these studies compared two groups of patients who underwent carpal tunnel release with or without flexor tenosynovectomy and concluded flexor tenosynovectomy seemed to reduce the recurrence of CTS symptoms [9]. We agree that flexor tenosynovectomy should be performed with carpal tunnel release when patients with hemodialysis-associated CTS have severe flexor tenosynovitis. However, we do not think the procedure should be done for all patients with hemodialysis-associated CTS even if they have a mild form of tenosynovitis.
We also aimed to compare patients with hemodialysis-associated CTS and idiopathic CTS in terms of complications related to carpal tunnel release. Four of our patients had complications, all were in the HD-CTS group: two had revision carpal tunnel releases and two had delayed wound healing. Patients with hemodialysis-associated CTS seem to have a greater chance of experiencing complications after carpal tunnel release than patients with idiopathic CTS (p = 0.012). Other studies also reported similar rates of revision carpal tunnel release in patients with hemodialysis-associated CTS [6, 11], even though recurrence rates of CTS symptoms were much higher, ranging from 4.2% to 46.7% [6, 11, 17]. No AVF-related complication was observed in our series. For carpal tunnel release in patients with an ipsilateral AVF, a sterile 1-inch tourniquet was applied just proximal to the wrist crease to prevent AVF obstruction. Other studies rarely have reported AVF-related complications even though the pneumatic tourniquet was applied around the upper arm [11, 13]. However, AVF-related complications should be kept in mind if the carpal tunnel release takes longer than usual when the pneumatic tourniquet is used.
The majority of our patients with hemodialysis-associated CTS had impairment 2 years after carpal tunnel release, whereas the patients with idiopathic CTS did not. The CTS-related symptoms were much less severe than preoperative symptoms in patients receiving long-term hemodialysis. Therefore, although carpal tunnel release did not completely resolve the symptoms at 2 years after surgery, most patients were improved and we recommend carpal tunnel release for patients with hemodialysis-associated CTS if nonoperative treatment fails.
References
Amadio PC, Silverstein MD, Ilstrup DM, Schleck CD, Jensen LM. Outcome assessment for carpal tunnel surgery: the relative responsiveness of generic, arthritis-specific, disease-specific, and physical examination measures. J Hand Surg Am. 1996;21:338–346.
American Association of Electrodiagnostic Medicine, American Academy of Neurology, American Academy of Physical Medicine and Rehabilitation. Practice parameter for electrodiagnostic studies in carpal tunnel syndrome: summary statement. Muscle Nerve. 1993;16:1390–1391.
Atroshi I, Breidenbach WC, McCabe SJ. Assessment of the carpal tunnel outcome instrument in patients with nerve-compression symptoms. J Hand Surg Am. 1997;22:222–227.
Bromley GS. Minimal-incision open carpal tunnel decompression. J Hand Surg Am. 1994;19:119–120.
Gejyo F, Narita I. Current clinical and pathogenetic understanding of beta2-m amyloidosis in long-term haemodialysis patients. Nephrology (Carlton). 2003;8(suppl):S45–S49.
Gilbert MS, Robinson A, Baez A, Gupta S, Glabman S, Haimov M. Carpal tunnel syndrome in patients who are receiving long-term renal hemodialysis. J Bone Joint Surg Am. 1988;70:1145–1153.
Gousheh J, Iranpour A. Association between carpel tunnel syndrome and arteriovenous fistula in hemodialysis patients. Plast Reconstr Surg. 2005;116:508–513.
Harris SA, Brown EA. Patients surviving more than 10 years on haemodialysis: the natural history of the complications of treatment. Nephrol Dial Transplant. 1998;13:1226–1233.
Hirasawa Y, Ogura T. Carpal tunnel syndrome in patients on long-term haemodialysis. Scand J Plast Reconstr Surg Hand Surg. 2000;34:373–381.
Kessler M, Netter P, Azoulay E, Mayeux D, Pere P, Gaucher A. Dialysis-associated arthropathy: a multicentre survey of 171 patients receiving haemodialysis for over 10 years. The Co-operative Group on Dialysis-associated Arthropathy. Br J Rheumatol. 1992;31:157–162.
Kim SJ, Shin SJ, Kang ES. Endoscopic carpal tunnel release in patients receiving long-term hemodialysis. Clin Orthop Relat Res. 2000;376:141–148.
Levine DW, Simmons BP, Koris MJ, Daltroy LH, Hohl GG, Fossel AH, Katz JN. A self-administered questionnaire for the assessment of severity of symptoms and functional status in carpal tunnel syndrome. J Bone Joint Surg Am. 1993;75:1585–1592.
Naito M, Ogata K, Goya T. Carpal tunnel syndrome in chronic renal dialysis patients: clinical evaluation of 62 hands and results of operative treatment. J Hand Surg Br. 1987;12:366–374.
Otsubo S, Kimata N, Okutsu I, Oshikawa K, Ueda S, Sugimoto H, Mitobe M, Uchida K, Otsubo K, Nitta K, Akiba T. Characteristics of dialysis-related amyloidosis in patients on haemodialysis therapy for more than 30 years. Nephrol Dial Transplant. 2009;24:1593–1598.
Serra JM, Benito JR, Monner J. Carpal tunnel release with short incision. Plast Reconstr Surg. 1997;99:129–135.
Shinzato T, Nakai S, Akiba T, Yamagami S, Yamazaki C, Kitaoka T, Kubo K, Maeda K, Morii H. Report of the annual statistical survey of the Japanese Society for Dialysis Therapy in 1996. Kidney Int 1999;55:700–712.
Shiota E, Tsuchiya K, Yamaoka K, Kawano O. Open carpal tunnel decompression in long-term haemodialysis patients [corrected]. J Hand Surg Br. 2001;26:529–532.
Sivri A, Celiker R, Sungur C, Kutsal YG. Carpal tunnel syndrome: a major complication in hemodialysis patients. Scand J Rheumatol 1994;23:287–290.
Acknowledgments
We thank Bo Ram Kim RN (specializing in orthopaedics) (BRK) for assessing clinical outcomes and collecting data.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she, or a member of their immediate family, has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
About this article
Cite this article
Kang, H.J., Koh, I.H., Lee, W.Y. et al. Does Carpal Tunnel Release Provide Long-Term Relief in Patients with Hemodialysis-Associated Carpal Tunnel Syndrome?. Clin Orthop Relat Res 470, 2561–2565 (2012). https://doi.org/10.1007/s11999-012-2309-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-012-2309-4