
Abstract
Background
Gowers’ sign is a screening test for muscle weakness, typically seen in Duchenne muscular dystrophy but also seen in numerous other conditions. The mildest presentations and the variations of Gowers’ sign are poorly described in the literature but are important to recognize to help with early diagnosis of a neuromuscular problem.
Questions/purposes
We therefore (1) defined the characteristics of the mildest forms and the compensatory mechanism used, (2) categorized the spectrum of this sign as seen in various neuromuscular diseases, and (3) provide educational videos for clinicians.
Methods
We videotaped 33 patients with Gowers’ sign and three healthy children. Weakness was categorized as: mild = prolonged or rise using single-hand action; moderate = forming prone crawl position and using one or two hands on thigh; severe = more than two thigh maneuvers, rising with additional aid, or unable to rise.
Results
The earliest changes were exaggerated torso flexion, wide base, and equinus posturing, which reduce hip extension moment, keep forces anterior to the knee, and improve balance. Patients with moderate weakness have wide hip abduction, shifts in pelvic tilt, and lordosis, which reduce knee extension moment, improve hamstrings moment arm, and aide truncal extension. The classic Gowers’ sign (severe) exaggerates all mechanisms.
Conclusions
The classically described Gowers’ sign is usually a late finding. However more subtle forms of Gowers’ sign including mild hand pressure against the thigh and prone crawl position should be recognized by clinicians to initiate additional diagnostic tests.
Level of Evidence
Level III, diagnostic study. See the Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In 1879, neurologist Sir William Richard Gowers described a pattern of rising from the floor seen in boys with pseudohypertrophic muscular paralysis [2], now known as Duchenne muscular dystrophy [9]. Although Gowers was not the first to notice this particular motor behavior [9], he was perhaps the first to emphasize the importance of this sign and suggested that it was probably pathognomonic of Duchenne muscular dystrophy, although in fact it is not [2, 9, 10]. Gower’s sign can be seen with any condition that is associated with weakness of the pelvic girdle or lower extremities, including but not limited to, Becker’s muscular dystrophy, limb girdle and other muscular dystrophy, proximal ascending pseudomyopathic diseases, spinal muscular atrophy, sarcoglycanopathy, polymyositides, discitis, and juvenile idiopathic arthritis.
Gowers’ sign is an excellent screening test for muscle weakness and is classically described as follows: from a supine or sitting position, a child will first roll prone, extending their arms and legs far apart. With most of the trunk weight resting on the extended arms, they push the body backward to shift the weight of the trunk over the extended legs. To extend the hip, the child places their hands onto the knees and walks the arms up the thighs until upright [6]. Children with mild disease may not even need a hand on the knee as they are able to bend at the hips once the knees are extended [4]. The mildest presentations of Gowers’ sign are poorly described in the literature but are important to recognize early, as early diagnosis of hereditary causes of pelvic girdle weakness can be valuable in counseling parents regarding potential future offspring.
We therefore (1) defined the characteristics of the mildest forms of Gowers’ sign and the compensatory mechanism used by the patients to stand, (2) categorized the spectrum of this sign as seen in various neuromuscular diseases, and (3) provided educational videos for clinicians to use.
Patients and Methods
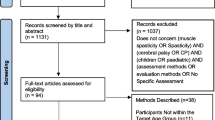
The patients in this study were seen in a multidisciplinary neuromuscular clinic with two neurologists, the senior author (SJM), and other physicians and therapists. The diagnosis was made by the neurologist using any diagnostic test they needed. The senior author invited all patients with a positive Gowers’ sign to be videotaped. Consent forms to videotape the patients were obtained from the legal guardian. We retrospectively reviewed the videos of 33 patients with a positive Gowers’ sign. There were 26 males and seven females. Seven patients were videotaped more than once for a total of 41 videos, made between July 2001 and November 2010. The average age of the patients was 8 years (range, 3–19 years). There were 13 patients with Duchenne muscular dystrophy, one with Becker muscular dystrophy, three with congenital muscular dystrophy, two with Ullrich muscular dystrophy, one with congenital myotonic dystrophy, three with unknown muscular dystrophy (per neurology), two with congenital fiber-type disproportion, three with congenital myopathy, one with sarcoglycanopathy, one with spinal muscular atrophy, one with mitochondrial myopathy, one with an inflammatory hip, and one with Guillain-Barré syndrome (Fig. 1). There were also three healthy patients as control subjects, two males and one female, with an average age of 7 years.

The distribution of diagnoses is shown.
The patients were videotaped performing Gowers’ sign from the knee sit position. Some also were videotaped performing the maneuver from a supine position. The maneuvers were repeated and videotaped from the coronal and sagittal views. The patients were encouraged to rise from the floor without use of their hands if possible. The videos were evaluated for actions such as rolling prone, forming the prone crawl position on the hands and knees, using one or more maneuvers of the arms to extend the hips, compensatory torso position, and foot equinus. Age at filming and time to complete the maneuver were recorded and analyzed with descriptive statistics. Our three healthy children take only a second to stand (Video 1. Supplemental material is available with the online version of CORR).
From patient records we extracted the following: age of the patient at initial presentation, age when Gowers’ sign initially was noted, most recent ambulatory status, age at cessation of ambulation, and age at diagnosis.
We classified the maneuvers (Table 1) using a scale developed by Cornelio et al. with minor modifications, adding one hand support on the thigh as a characteristic of level 2, and multiple hand maneuvers as a characteristic of level 8 [1]. Weakness levels were classified as follows: mild weakness (1 to 4 points) included prolonged or strained rise without support, rise using a one hand support on the thigh, or rise using one or both hands on the floor without thigh support; moderate weakness (5 to 7 points) included use of the prone crawl position and one to two hands on the thigh in rising; and severe weakness (8 to 10 points) included use of the prone crawl position with more than two hand-on-thigh maneuvers, rising only with additional aid (chair, gurney, etc), or being unable to rise (Table 2).
Results
Our findings in the mildest cases of Gowers’ sign were as follows: 13 videos showed 11 different patients with a mild Gowers’ sign (Video 2. Supplemental material is available with the online version of CORR). The average Gowers’ sign time was 3.1 seconds (range, 1–8 seconds). All 11 patients were still able to ambulate at the time of this review. In the mildest cases of Gowers’ sign, the patients might simply take longer with more concentrated actions or have more instability in rising but do not require supports. Some flex the torso near or beyond 90° and plant the forward foot farther anteriorly for a wider base (Video 2. Supplemental material is available with the online version of CORR). In one patient, a valgus knee position was formed with the feet wide apart to serve as a base from which to rise. Equinus positioning often is seen. This is in contrast to our healthy control patients who usually took an upright kneeling position by extending the knees to 90° and the hips to neutral, forward flexed one hip, planted one foot, then fully extended the knees and hips, providing leverage into the upright stance with less than 30° torso flexion throughout rise. Their rise is smooth, with a narrow base, no equinus, and their normal rise time is usually 1 second (Video 1. Supplemental material is available with the online version of CORR).
Twenty videos showed 15 patients with a moderate Gowers’ sign (Video 3. Supplemental material is available with the online version of CORR). Patients videotaped more than once showed progression of disease, but five of six remained in the moderate category. The average Gowers’ sign time was 8.1 seconds (range, 3–19 seconds). Eight of 15 patients with moderate Gowers’ sign had lost the ability to ambulate by the time of this review. The mean time from videotaping until loss of ambulation was 3.3 years. Eight videos showed patients with severe Gowers’ sign (Video 4. Supplemental material is available with the online version of CORR). The average Gowers’ sign time was 20.8 seconds (range, 6–50 seconds). The mean time from videotaping until loss of ambulation was 2.4 years (Table 3). With moderate Gowers’ sign (Video 3. Supplemental material is available with the online version of CORR), children start using the prone crawl position on all hands and knees. Once prone, the hands are walked backward toward the feet or vice versa, which shifts the center of gravity over previously extended legs. Wide hip abduction is commonly seen in this stage. Often maneuvers such as an equinus thrust while a hand is on the ipsilateral thigh provide additional force and momentum. Hyperlordosis of the torso shifts the center of gravity posteriorly to allow locking of the anterior hip capsule. To complete the maneuver, children commonly waddle in place, reducing earlier compensatory hip abduction. With severe Gowers’ sign (Video 4. Supplemental material is available with the online version of CORR), the prone position is more extended and the feet are wider apart. Children with severe Gowers’ sign also require more hand supports on the floor, multiple supports on the thigh, or additional external support. The torso is flexed farther forward and more time is spent in equinus.
The entire spectrum of Gowers’ sign can be viewed on the four supplemental videos available with the online version of CORR.
Discussion
Gowers’ sign as classically described is a late finding. The mildest presentations of Gowers’ sign are poorly described in the literature but are important to recognize, as early diagnosis of hereditary causes of pelvic girdle weakness can be valuable in counseling parents regarding potential future offspring. We therefore (1) defined the characteristics of the mildest forms of Gowers’ sign and the compensatory mechanism used by the patients to stand, (2) categorized the spectrum of this sign as seen in various neuromuscular diseases, and (3) provided educational videos for clinicians to use.
There are several limitations of our study. First, not all children were agreeable to being videotaped and younger ones with milder signs often were not cooperative. However, we presume the patients we did videotape are representative of the population. Performance of Gowers’ sign also is difficult to standardize, but effort was made to use the same knee sit position in most patients and encourage rapid rise without using the hands if possible.
Our first goal was to define the characteristics of milder forms of Gowers’ sign and the compensatory mechanism used by the patients to stand. Gowers’ sign is a physical examination screening test for muscle weakness, classically seen in Duchenne muscular dystrophy. Patients with numerous conditions (eg, Becker muscular dystrophy, congenital muscular dystrophy, Ullrich muscular dystrophy, congenital fiber-type disproportion, sarcoglycanopathy, spinal muscular atrophy, mitochondrial myopathy, inflammatory hip, or Guillain-Barré syndrome) also can have this finding (Fig. 1). In any child using a hand push off the thigh, it is important to repeat the test as even a healthy toddler may use this form of hand push to get up. Often an obese child will use a hand push off the thigh or floor, which can give a false positive Gowers’ sign. Sometimes it is necessary to have them get up from the kneeling position with their arms crossed across their chest. Milder presentations of Gowers’ sign are poorly described in the literature but are important to recognize early. The clinician then can start the appropriate neuromuscular workup. Earlier diagnosis obviously is helpful for the patient in providing physical therapy, bracing, and sometimes surgery. In addition, many of these disorders are hereditary conditions in which earlier diagnosis can be valuable in counseling parents regarding potential future offspring.
Second, we wanted to categorize the spectrum of this sign as seen in various neuromuscular diseases and document the compensatory mechanisms used in more involved children. The time to perform the Gowers’ sign ranges from 1 second in a healthy child, to 3 seconds in the mild group, 8 seconds in the moderate group, and an average of 21 seconds in the severe group. The earliest forms of Gowers’ sign include exaggerated torso flexion, wide base formation, prolonged rise, instability, equinus posturing, and occasional arm supports off the floor. These stem from beginnings of muscle weakness but they also serve as compensatory mechanisms to ease the ability to rise. Equinus posturing is not typical in healthy patients, and is likely a result of Achilles contractures, but this also helps to maintain a force line anterior to the knee compensating for extension weakness [8]. In moderate cases, the prone crawl position and extension of all four extremities is used. Consistent with a previous study, children who had a positive Gowers’ sign almost universally turned prone first in rising from a supine position [12], which reduces the forces required for knee extension. By focusing on singular joint actions, this also might reduce the energy required for typical coactivation of multiple muscle groups in the rising action [13]. With the knees extended, the hamstrings are stretched resulting in maximized knee extension moment [11]. The upper extremities’ position of abduction and extension further helps to complete hip extension. Wide hip abduction, in part from tensor fascia lata shortening, compensates for gluteus medius and minimus weakness by producing a wide base as normal balance and stability are compromised. The wide abduction is reduced once upright with waddling in place. Anterior pelvic tilt, lumbar hyperlordosis, and upper limb extension are used to compensate for a weak gluteus maximus muscle. In severe cases, hand supports on the floor and thigh travel less distance, secondary to a weaker shoulder girdle, knee extensors, and hip extensors. Heel contracture and equinus posturing often are evident, but also serve to improve the knee extension moment. However, when the equinus becomes too severe or when hip and/or knee flexion contractures develop, the patient cannot arise without an external support of a chair or wall.
Our final goal was to provide an educational video for clinicians to use. We have developed these teaching videos, as reference guides for clinicians, showing the spectrum of Gowers’ sign and the wide range of compensatory mechanisms which these children use when rising. Our study confirms that many neuromuscular diseases can produce a positive Gowers’ sign and multiple variations can be seen [3–5, 7, 9]. The classically described Gowers’ sign is the severe grade on our scale and is usually a late finding. Milder Gowers’ signs should be recognized so that earlier diagnosis of the type of neuromuscular disease can be made. The videos should help clinicians’ achieve that goal.
References
Cornelio F, Dworzak F, Morandi L, Fedrizzi E, Balestrini MR, Gondoni L. Functional evaluation of Duchenne muscular dystrophy: proposal for a protocol. Ital J Neurol Sci. 1982;3:323–330.
Gowers WR. Clinical lecture on pseudo-hypertrophic muscular paralysis. Lancet. 1879;2:1–2, 37–39, 73–75, 113–116.
Kang PB, Krishnamoorthy KS, Jones RM, Shapiro FD, Darras BT. Atypical presentations of spinal muscular atrophy type III (Kugelberg-Welander disease). Neuromuscular Disord. 2006;16:492–494
Koehler PJ, Bruyn GW, Pearce JMS, eds. Neurological Eponyms. New York, NY: Oxford University Press; 2000.
Mirovsky Y, Copeliovich L, Halperin N. Gowers’ sign in children with discitis of the lumbar spine. J Pediatr Orthop B. 2005;14:68–70.
Pearce JM. Gowers’ sign. J Neurol Neurosurg Psychiatry. 2000;68:149.
Stathopulu E, Baildam E. Gowers’ sign in children with juvenile idiopathic arthritis. Rheumatology (Oxford). 2003;42:1002–1003.
Sutherland DH, Olshen R, Cooper L, Wyatt M, Leach J, Mubarak S, Schultz P. The pathomechanics of gait in Duchenne muscular dystrophy. Dev Med Child Neurol. 1981;23:3–22.
Tyler KL. Origins and early descriptions of “Duchenne muscular dystrophy”. Muscle Nerve. 2003;28:402–422.
Tyler KL, McHenry LC Jr. Classics in neurology. Fragments of neurologic history: pseudohypertrophic muscular dystrophy and Gowers’ sign. Neurology. 1983;33:88–89.
Visser JJ, Hoogkamer JE, Bobbert MF, Huijing PA. Length and moment arm of human leg muscles as a function of knee and hip-joint angles. Eur J Appl Physiol Occup Physiol. 1990;61:453–460.
Wallace GB, Newton RW. Gowers’ sign revisited. Arch Dis Child. 1989;64:1317–1319.
Zajac FE. Understanding muscle coordination of the human leg with dynamical simulations. J Biomech. 2002;35:1011–1018.
Author information
Authors and Affiliations
Corresponding author
Additional information
Each author certifies that he or she, or a member of their immediate family, has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research editors and board members are on file with the publication and can be viewed on request.
Each author certifies that his or her institution approved the human protocol for this investigation, that all investigations were conducted in conformity with ethical principles of research.
This study was performed at Rady Children’s Hospital and Health Center.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Video 1 (WMV 14559 kb)
Video 2 (WMV 24796 kb)
Video 3 (WMV 43171 kb)
Video 4 (WMV 41546 kb)
About this article
Cite this article
Chang, R.F., Mubarak, S.J. Pathomechanics of Gowers’ Sign: A Video Analysis of a Spectrum of Gowers’ Maneuvers. Clin Orthop Relat Res 470, 1987–1991 (2012). https://doi.org/10.1007/s11999-011-2210-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-011-2210-6