
Abstract
Background
Clinical cartilage restoration is evolving, with established and emerging technologies. Randomized, prospective studies with adequate power comparing the myriad of surgical techniques used to treat chondral injuries are still lacking and it remains a challenge for the surgeon treating patients to make evidence-based decisions.
Questions/purposes
We reviewed the history of the major cartilage repair/restorative procedures, indications for currently available repair/restorative procedures, and postoperative management.
Methods
We performed searches using MEDLINE and cartilage-specific key words to identify all English-language literature. Articles were selected based on their contributions to our current understanding of the basic science and clinical treatment of articular cartilage lesions or historical importance. We then selected 77 articles, two of which are articles of historical importance.
Results
Current cartilage restorative techniques include débridement, microfracture, osteochondral fragment repair, osteochondral allograft, osteochondral autograft, and autologous chondrocyte transplantation. Pending techniques include two-staged cell-based therapies integrated into a variety of scaffolds, single-stage cell-based therapy, and augmentation of marrow stimulation, each with suggested indications including lesion size, location, and activity demands of the patient. The literature demonstrates variable improvements in pain and function contingent upon multiple variables including indications and application.
Conclusions
For the patient with symptomatic chondral injury, numerous techniques are available to the surgeon to relieve pain and improve function. Until rigorous clinical trials (prospective, adequately powered, randomized control) are available, treatment decisions should be guided by expert extrapolation of the available literature based in historically sound principles.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Injury to articular cartilage is common; one study of 31,516 knee arthroscopies found 63% of patients had chondral injury [14]. Cartilage injuries of the knee affect approximately 900,000 Americans annually, resulting in more than 200,000 surgical procedures [13].
Although nonsurgical management of articular cartilage injury has remained largely the same over many decades, surgical treatment of chondral injuries continues to evolve. Reparative techniques (marrow stimulation) and restorative techniques (cell-based therapies and autologous or allograft transplants) continue to be refined, giving surgeons more tools and options for biologic reconstruction of the articular surfaces.
Surgical attempts at restoration of articular cartilage have a long history. Early techniques included epiphyseal and whole-joint transplants [43, 45]. In 1925, one of the first osteoarticular transplants was described [44]. Contemporary methods have evolved from several different approaches. Current marrow stimulation procedures have emerged from the Pridie technique [60], which was later termed spongialization by Ficat et al. [17]. This technique allows primitive mesenchymal stem cells to differentiate and form fibrocartilage [17, 60]. Dr. Allan Gross popularized the concept of fresh osteochondral allograft transplantation [26, 27] and Dr. Lars Peterson is responsible for the first generation of cultured chondrocyte implantation [58]. While there are a number of new emerging technologies at various stages of preclinical and clinical development, most will have their lineage from one of these three distinct approaches. By understanding the use of existing cartilage surgical approaches, their limitations, and the nuances of postoperative rehabilitation, it may be possible to further refine these techniques to improve pain, function, and patient satisfaction.
Current cartilage restorative procedures include marrow stimulation, fresh osteochondral allografts, osteochondral autografts, and cultured cartilage implantation. Although these provide treatment options for the patient with a symptomatic chondral injury, there remains abundant controversy and confusion on the application of these techniques.
To help surgeons navigate the literature and reconcile treatment options and techniques for application to specific injuries and patients, we reviewed (1) the history of the major cartilage repair/restorative procedures: marrow stimulation, osteochondral allografts, cultured chondrocyte implantation, osteochondral autografts; (2) indications for currently available repair/restorative procedures; and (3) postoperative management.
Search Strategy and Criteria
We searched all published literature in the English language using MEDLINE for the key words “articular cartilage injury” AND “marrow stimulation OR microfracture” (323 articles), “osteochondral autograft” (114 articles), “osteochondral allograft” (48 articles), and “autologous chondrocyte implantation” (113 articles). Within each subgroup, all titles were reviewed by three authors (JK, AD, SS). We preliminarily excluded 140 articles because they were nonmusculoskeletal (20); did not discuss articular cartilage injury (48); or primarily discussed small joints, nonweightbearing joints, or the spine (72). Abstracts of the remaining articles were reviewed. Seventy-seven articles were chosen by the two senior authors (BC, JF) based on their relative contributions to our current understanding of the basic science (28), clinical treatment of articular cartilage lesions (45), or historical importance (four). We included the four articles of historical importance published before MEDLINE (Lexer [44] [three articles] and Pridie [60]) (Fig. 1).

A flowchart shows the results of our search strategy for articles relevant to our review.
Current Cartilage Repair/Restorative Techniques
Marrow Stimulation
Pridie and Ficat developed a treatment for cartilage defects and chondrosis with aggressive débridement of cartilage and removal of subchondral bone to expose the cancellous bone [3, 6, 17, 60]. This resulted in clot formation with marrow elements that gradually organized and remodeled to create fibrocartilage fill. Patient outcomes were highly variable and largely anecdotal [17, 60]. These case series did not have a control group and thus the positive effects from débridement alone were unknown. This was especially true when patients presented with the acute or subacute onset of mechanical symptoms (ie, unstable osteochondritis dissecans) that responded favorably to débridement with little or no symptoms related to the presence of the cartilage defect itself. Ficat et al. [17] have reported minimal to no pain and improvements in function from this procedure in 79% of patients treated with spongialization.
With the advent of arthroscopy in the 1970s, early arthroscopic pioneers applied the Pridie and Ficat principles of débriding cartilage lesions to subchondral bone and then creating bleeding at the base of the lesion [33]. Gradually the technique evolved from full removal of the subchondral plate to a gentle superficial burring termed abrasion arthroplasty. This allowed bleeding yet maintained the majority of the thickness of the subchondral plate. Dr. Lanny Johnson suggested a “super clot” would form with better adherence if these technical principles were adopted [77]. Because of the technical demands and variability required to “lightly burr” the subchondral plate, drilling and microfracture, as popularized by Steadman et al. [70], largely supplanted abrasion arthroplasty. With microfracture, after the calcified cartilage layer is removed, a small microfracture awl is used to create 1- to 2-mm fracture holes spaced 3 to 5 mm apart to create bleeding and clot formation. Empirically, it was believed the “marrow-derived cells” would lead to hyaline-like cartilage if exposed to the appropriate postoperative mechanical environment (continuous passive motion and protected weightbearing) [66]. In addition, it was suggested microfracture did not cause thermal necrosis thought possible with drilling and the act of fracturing would stimulate the “healing response” cascade [70]. The relative ease of performing an all-arthroscopic and resource-efficient procedure coupled with acceptable results in small- to medium-sized cartilage lesions led to microfracture becoming the most widely used cartilage restoration procedure in the United States [50]. Still under debate is the upper limit of lesion size that allows for a reasonable result and whether it is useful for patellar lesions. Steadman et al. [69] reported good results in all compartments with lesions greater than 4 cm2 while Knutsen et al. [39] found worse clinical outcomes based on SF-36 scores with lesions (only femoral lesions where treated) over 4 cm2. Kreuz et al. [41] noted uniformly poor results at the patella and in patients older than 40 years.
Semantically, these techniques are commonly lumped into the category of “marrow stimulation.” This terminology may be considered somewhat of a misnomer as there is typically little or no red marrow in subchondral cancellous bone and thus most of the pluripotential cells in the clot are similar in origin to any other clot that occurs clinically throughout the body. Cytokines released during clot formation attract pluripotential cells that form tissue that ranges from fibrous to hyaline-like cartilage. One current technique increases the number of adult stem cells by harvesting true hematopoietic marrow from the iliac crest and transferring the marrow or concentrated adult stem cells to a microfracture-prepared bed [18]. As the goal is to encourage the pluripotential cells to differentiate into a chondrocyte-like phenotype with three-dimensional structure, another approach is to apply an acellular scaffold that provides a framework for cells to organize (autologous membrane-induced chondrogenesis). The scaffold may range from a true physical membrane or a biphasic liquid hydrogel that congeals in situ. With each of these techniques, it may be possible to further influence the pluripotential cells with growth factors, such as reported with bone morphogenetic protein 7, also known as osteogenic protein 1 [11, 36, 37]. To date, the nuances of marrow stimulation continue to be refined. For example, Chen et al. [9] demonstrated, in an animal model, drilling does not cause thermal injury and the drill holes actually allow more consistent channels for cell migration compared to microfracture holes that may be partially blocked with bony debris. Finally, the postoperative environment is important in directing cell differentiation, although the exact degree of weightbearing and duration of continuous passive motion (or equivalent) remains unknown.
Fresh Osteochondral Allografts
Dr. Allan Gross began using fresh osteochondral allografts for segmental loss of bone and cartilage after en bloc resection of knee tumors [26, 27]. At the same time, frozen osteochondral allografts were also being used, but over time, the matrix deteriorated due to the absence of viable chondrocytes [47]. This importance of viable cells remains a tenant of osteochondral allografts as various forms of cryopreservation have largely been unsuccessful [34, 47, 74]. The initial application of osteoarticular grafts was with large segmental joint transplantation with large portions of bone. Notably, avascular bone requires extensive time to be replaced or incorporated through creeping substitution and thus bony collapse or insufficiency fractures were not uncommon [61]. Because chondral and osteochondral nonneoplastic lesions of the knee typically are associated with minimal involvement of the subchondral bone, Bugbee and Convery [7] recommended osteochondral allografts have the least amount of bone possible to minimize these adverse consequences. Although there is evidence using a goat model that chondrocyte viability may be improved with prolonged storage at 37°C, current constructs utilize fresh grafts stored for 14 to 28 days at 4°C with only 6 to 8 mm of subchondral bone [56, 72, 73]. While empirically the chances for success increase as the number of more viable chondrocytes increases, the absolute number of viable chondrocytes required to maintain the matrix over time remains unknown. The chondrocyte viability can be further compromised at the time of implantation as osteochondral allografts and cartilage in general remain vulnerable to the effects of impaction and thus the recommendation for minimal force insertion [35, 62]. Finally, the viability may be further negatively influenced by the postoperative environment [59].
Although it is often stated osteochondral allografts are immunoprivileged, a percentage of patients become antibody positive after osteochondral allograft transplantation [8, 19, 20]. Comparing patient outcomes, those who were antibody positive had less favorable outcomes compared to those who were antibody negative [21, 68, 76]. It is generally believed the antibodies form in response to the bony portion of the graft and, more specifically, the vascular and marrow elements present within the subchondral bone. Therefore, thin “shell allografts” may potentially decrease the risk of immunogenicity as the total volume of bone is diminished and the thin bone shell can be better cleared of marrow elements by pulsatile lavage.
The results of osteochondral allograft transplantation have been promising. Ghazavi et al. [23] investigated the results of fresh osteochondral allografts used to reconstruct posttraumatic osteochondral defects in 123 patients with a mean age of 35 years. They reported 85% of the knees had an increase in at least 10 points postoperatively in modified Hospital for Special Surgery knee score, or maintenance of a score of 75 or greater, with no need for further surgery. Only 18 failures were reported in this series at a mean followup of 7.5 years. These authors found patients with an age of more than 50 years, bipolar defects, malalignment, and Workers Compensation were at risk for an increase of failure [23]. Similar results were found by Chu et al. [10] in a study of 55 patients who underwent osteochondral allograft transplantation in the knee with an average followup of 75 months. Overall, they reported 76% of knees were rated “good” or “excellent.” However, when the results were subcategorized, 84% of patients with unipolar transplants were rated “good” to “excellent” versus only 50% of those with bipolar procedures [10]. Bugbee and Convery [7] reported 18 patients (19 knees) with greater than 10-year followup. The average surface area replaced was 11 cm2. Fourteen of these were monopolar lesions and five were bipolar. Although three patients (four knees) had died at the followup time period reviewed, of the remaining 15 knees, 11 were rated “good” or “excellent.” One knee underwent repeat allografting at 8 years postoperatively, two underwent knee arthroplasty, and one underwent arthrodesis [7].
Davidson et al. [15] reported 67 patients who received osteochondral allografts for the treatment of full-thickness femoral condylar lesions with a mean followup of 40 months. They found improvements in both the International Knee Documentation Committee and SF-36 scores as compared to preoperative values and nearly normal International Cartilage Repair Society (ICRS) scores at followup. Furthermore, second-look arthroscopy performed in 10 knees revealed grossly normal repair tissue, and biopsy samples demonstrated no differences between graft and native cartilage chondrocyte density [15]. Similar improvements in clinical outcome measures have also been reported by McCulloch et al. [48] who demonstrated 84% satisfaction in 25 consecutive patients with an average followup of 35 months.
A new cartilage allograft technique under investigation involves the implantation of intact fragments of articular cartilage only. The technique uses minced juvenile allogenic fresh-stored cartilage and forms hyaline-like cartilage in the laboratory [2]. It is currently available in the United States because it is accepted by the US Food and Drug Administration (FDA) as any other isotopic use of allograft that is “minimally manipulated tissue.” However, there is only one published case [4] and two case series reported at the 2010 ICRS Congress (Farr J, Kercher J, Salata M, and Yao J); www.clinicaltrials.gov lists an ongoing prospective postmarket uncontrolled case series (Trial Number NCT00791245).
Another isotopic use of minimally manipulated (same FDA oversight as minced juvenile cartilage) osteochondral allograft is cold-sterilized radiated osteochondral cylinders of various sizes, which have undergone matrix crosslinking with methylene blue. An uncontrolled prospective case series is scheduled to begin in 2011. Obviously, no comments can be made on efficacy.
Cultured Chondrocyte Implantation
Dr. Lars Peterson’s report of a two-stage cartilage restoration technique initiated the interest in cell-based therapy for the treatment of cartilage lesions [59]. Initially, a biopsy of healthy articular cartilage is arthroscopically harvested from a low- or no-load location. The cartilage is then enzymatically treated to release the chondrocytes, which are subsequently expanded in culture to create more than 10 million cells from only the few hundred thousand cells originally in the biopsy. The cell suspension is then injected historically beneath a periosteal patch or more recently a collagen scaffold [24].
Over the years since Peterson’s original description, there have been several modifications of the technique of autologous chondrocyte implantation (ACI). The cellular aspect of ACI has recently become a major focus. For example, there may be a lack of uniformity of the cultured chondrocytes from laboratory to laboratory. In an effort to quantify the cultured chondrocytes, advances are currently testing cells for their phenotype and their ability to produce matrix elements. Theoretically, the ability to manipulate chondrocytes during the culturing process may optimize the production of tissue that is most like hyaline cartilage.
The original ACI technique utilized autologous periosteum to form a watertight cover under which the chondrocyte suspension was injected. In recent years, synthetic collagen has been used as a patch (collagen patch ACI) with clinical outcomes similar to ACI. The technique has been further modified to include seeding of the patch with chondrocytes before implantation and finally allowing the cells to grow on the scaffold matrix (matrix ACI), which allows an all-arthroscopic technique [71].
The concept of changing a two-stage procedure to a one-stage procedure is appealing to both patients and payers. After preclinical studies noted the potential of minced autograft cartilage to produce new cartilage fill in focal defects, a Phase I/II trial was initiated, which demonstrated the safety and efficacy of implanting a construct composed of a scaffold coated with minced cartilage fragments obtained arthroscopically during the same surgical setting. After the positive results of the initial trial, the FDA has approved a statistically powered randomized controlled Phase III trial (approved July 2, 2010) to evaluate the clinical efficacy of this technique. Potential future modifications of each of these techniques will focus on arthroscopic applications, efficacy, and cost-effectiveness.
Osteochondral Autografts
The technique of harvesting medium-sized (7- to 11-mm) osteochondral autograft plugs was popularized by Dr. Craig Morgan in the United States and Dr. Vladimir Bobic in the United Kingdom [3]. At a similar time, the use of smaller osteochondral plugs (mosaicplasty) was popularized by Dr. Lazlo Hangody in Hungary [28]. Both techniques create a circular socket at the recipient site with a drill or circular punch and are harvested using a circular tube osteotome. Several donor sites have been described, including the lateral trochlea near the sulcus terminalis, the intercondylar notch, and the medial trochlea, with Garretson et al. demonstrating in vitro the medial intersection of the trochlea and condyle had less stress [1, 22, 29, 30, 75]. Although long-term sequelae related to donor site harvest remain in question, there are subsets of patients who experience pain at the harvest sites in the near term. To decrease morbidity, low-load areas are used for the donor site and the resultant harvest voids are often back-filled with allograft or synthetically engineered plugs [22].
The literature demonstrates filling the recipient socket entirely can avoid cyst formation, the use of minimal force during impaction can avoid chondrocyte death, and fitting the plug to the surrounding surface can minimize alterations in contact stress [35, 40]. Additionally, the long-term effects of peripheral chondrocyte death, lack of marginal integration when there is side-to-side initial contact, and fibrocartilage fill of voids between the plugs remain to be determined [31]. Several synthetic plugs are in various stages of testing in the United States to assess their ability to become an alternative to the autograft plug. This would utilize the same technique as autograft plugs but would avoid harvest morbidity and would allow an on-the-shelf alternative for smaller defects.
Indications and Technique Selection for Specific Chondral Lesions
The concept of “demand matching” may be applied when deciding on the specific cartilage restoration technique for a particular lesion. Demand matching attempts to match the technique characteristics that best fit the clinical presentation of the patient, the limb, the knee, and the cartilage lesion. This raises several questions related to the necessity of a cartilage repair procedure to definitively create normal stratified hyaline cartilage with basilar and marginal integration. Most reports of cell therapy techniques including histologic analysis as an outcome report substantial tissue variability, with none showing normal stratified hyaline cartilage. For example, Knutsen et al. [39] compared microfracture to ACI with histology ranging from fibrous to hyaline-like in both groups with no correlation with clinical outcome. On the other hand, Saris et al. [67] reported superior histology of biopsies of a chondrocyte cell-based technology compared to microfracture at 1 and 3 years, with those patients implanted with the chondrocyte cell-based technology procedure demonstrating superior outcomes. Kreuz et al. [41] noted progressively deteriorating results in patients after microfracture over time, yet some patients younger than 40 years continued to do well, especially those with smaller lesions of the femoral condyle. In one of the few studies evaluating different surgical treatments for articular cartilage injury, Knutsen et al. [38] reported 2-year outcome data and subsequently on their 5-year outcomes of patients with chondral defects randomized to treatment with microfracture versus ACI. These authors reported no differences in outcomes when comparing the two techniques. Although both studies were prospective and randomized, criticisms of the Knutsen series centered on inadequate patient numbers for statistical power and lack of subset analysis of smaller versus larger lesions.
Taken in aggregate, it appears the cost-effective technique of microfracture may be appropriate for smaller condylar lesions in patients younger than 40 years, but it may be more cost-efficient in the long term to consider osteochondral allograft or cell-based therapy for larger lesions [16, 51]. Additional study is needed to determine whether there is an upper age ceiling when autologous cells do not perform as well as allograft [53, 64].
Patient Selection
Based on our experience, patients with chondral injuries should be considered for treatment, not solely because they have a cartilage defect by MRI or arthroscopy, but rather because they have knee pain and functional loss that can be assigned to the defect. With current techniques, we believe the ideal patient has a body mass index of less than 35 kg/m2, has realistic expectations, is willing to adhere to postoperative rehabilitation protocols, has localized cartilage defects, and is symptomatic. In addition, all relevant comorbidities (eg, malalignment, meniscal deficiency, or ligament deficiency) must be identified and corrected in either a staged or concomitant fashion. With the baby boomer generation experiencing a larger number of knee cartilage problems, there will be pressure to expand cartilage restoration from contained focal defects to larger bipolar and uncontained cartilage defects. The goal is to preoperatively predict the best treatment for the patient, limb, knee, and defect considering the patient age, lesion size, lesion location, and chondral status of the joint proper (Table 1).
Articular cartilage cannot be restored in isolation. All pathologic or injured tissues of the knee “organ” must be treated. For example, the synovial lining is important in effecting the anti-inflammatory and inflammatory balance in the knee. Further studies are needed to evaluate what role, if any, hyaluronic acid injections, anti-inflammatory medications, and/or neutrapharmaceuticals play in addressing the local inflammatory environment of the knee.
To maximize patient outcomes and provide a suitable environment for the cartilage restorative procedure, concomitant pathology or mechanical problems should also be addressed. Ligamentous insufficiency and instability should be treated and normal mechanical alignment should be restored. Failure to do so may overload the cartilage implant and lead to failure on a mechanical basis even when the biology would have otherwise been successful. In addition, there are major therapeutic benefits to unloading the compartment that complement the results of a biologic reconstruction [24, 26]. The menisci improve the nutritional environment of the articular surfaces and reduce contact stress across the tibiofemoral joint. If compromised, meniscal function is re-established or at least improved through transplantation. Even partial meniscectomy is associated with increases in tibiofemoral contact forces [42]. The results of patients who undergo combined cartilage repair with meniscal allograft transplantation are equivalent or superior to those reported for cartilage repair as an isolated procedure [25, 65]. Rue et al. [65] reported a series of 30 patients with combined meniscal allograft transplantation procedures and cartilage restoration procedures. Using various standardized outcome surveys including the Lysholm, International Knee Documentation Committee, and SF-12 scales, these authors demonstrated 76% of patients were completely or mostly satisfied with their surgical results and 90% would have surgery again. Improvements in outcomes scores and patient satisfaction were comparable to historical published reports of these procedures performed in isolation.
Lesion Type and Site
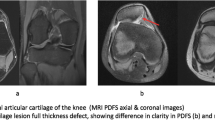
As opposed to the original Outerbridge cartilage lesion classification [55] that combined the extent of cartilage damage and size, the ICRS classification system maps and delineates the following: (1) defect dimensions, (2) defect grade (including depth), and (3) defect location mapping [5, 6, 46]. The original Outerbridge classification was designed to describe patellar chondrosis. Within Grades II and III, it combined the appearance/depth of the lesion with lesion size. Grade 0 lesion was normal cartilage. Grade I was softening. Grade II was a partial-thickness defect with fissures that did not reach subchondral bone and was less than 1 inch in diameter. Grade III was fissuring to the level of subchondral bone with a diameter greater than 1.5 cm. A Grade IV lesion had exposed subchondral bone. The more commonly used “modified Outerbridge” classification used only the description of the articular surface and reported the dimensions separately. In the ICRS classification system, Grade 1 is normal, Grade 1a has some mild softening or fibrillations, and Grade 2 has more involvement but still less than ½ the cartilage depth. Grade 3 lesions involve more than ½ the cartilage depth and include subgroups a, b, c, and d with increasing severity of damage (3a: > 50% cartilage thickness damage, 3b: damage to calcified cartilage; 3c: exposed subchondral bone, 3d: full-thickness delamination). A Grade 4 lesion is an osteochondral lesion violating the subchondral plate (4a: superficial; 4b: deep bony involvement). The dimensions and knee region of involvement are reported separately. This classification system allows for consistency in evaluating injuries of the articular surfaces, as well as development and implementation of treatment algorithms. It is important to use an intra-articular reference or ruler to precisely measure the defects as arthroscopic magnification is variable. This information will aid in staging the lesion for optimal treatment.
Postoperative Management
While each technique has unique postoperative requirements, certain generalizations are possible. As the human knee cannot be fully duplicated by any animal model, postoperative management has largely been empiric. For example, continuous passive motion as pioneered by Salter et al. [66] is often recommended to improve matrix production of chondrocytes and to aid in differentiation of pluripotential cells toward a more chondroid phenotype. Continuous passive motion reportedly improves proteoglycan and collagen reorganization [54, 63]. The degree of postoperative weightbearing allowed remains controversial for each technique. In studies evaluating long-term outcomes for ACI, histologic analysis demonstrated biopsies from weightbearing surfaces appeared to resemble organized hyaline cartilage with Type II collagen. Biopsies in nonweightbearing areas resembled fibrocartilage [57]. Mature chondrocytes (osteochondral autograft and allograft) need cyclic loading (within physiologic range) for nutrition and to stimulate maintenance of the surrounding matrix; in contrast, developing or differentiating cells need loading but at a much lower magnitude.
Strengthening is obviously a key to enhancing function, but when the muscle units that need strengthening actually load the area of implantation, caution is warranted [52]. This is especially true in the patellofemoral compartment [12, 32, 49]. Therefore, early rehabilitation programs for cellular constructs should focus on a core proximal strengthening program until the implant is able to withstand physiologic loading. Return to sport-specific activities after articular cartilage restoration can be prolonged. After cell-based restorative procedures such as ACI, it can be up to 9 to 24 months after surgery to allow appropriate proliferation, matrix production, and maturation of the graft before substantial stressing [52].
Discussion
Symptomatic full-thickness chondral defects remain a major clinical challenge. Although nonsurgical management of articular cartilage injury has remained largely the same over the past decade, surgical treatment of chondral injuries continues to evolve and repair/restoration techniques continue to be refined, giving surgeons more tools and options for biologic reconstruction of the articular surfaces. Multiple options are described that can be used to treat similar lesions. We therefore performed a review of the pertinent literature on the topic to help allow surgeons to navigate the literature and reconcile treatment options and techniques for application to specific injuries and patients. We therefore reviewed (1) the history of the major cartilage repair/restorative procedures: marrow stimulation, osteochondral allografts, cultured chondrocyte implantation, osteochondral autografts; (2) indications for currently available repair/restorative procedures; and (3) postoperative management.
We acknowledge limitations with our review. First, ours is a selective review and not a systematic review of the literature. We performed our search using MEDLINE using multiple search terms with nesting but did not include a search of the EMBASE database or Google Scholar. Our search strategy may thus have missed eligible studies within the field of cartilage or articular cartilage injury. Second, other than the Knutsen et al. [39] and Saris et al. [67] studies discussed previously, there is a paucity of rigorous, Level I, prospective, randomized, adequately powered literature comparing treatments for chondral injury. Third, the low quality of the studies we reviewed mandates the results and conclusions of such studies be interpreted cautiously. As this is a selective review, we did not assess study quality using methodology formulated for use in systematic reviews.
Historical treatments have gradually evolved into contemporary techniques of restoring chondral lesions. Cartilage repair/restorative procedures have evolved substantially from original marrow stimulation techniques. While these advancements have attempted to enhance repair tissue quality and quantity in an attempt to ultimately improve durability and functional improvement, biopsies of cell therapy techniques have failed to show consistent hyaline cartilage and thus the common term hyaline-like is often used in the literature. As the structure of articular cartilage is intricately linked to its function and the reproduction of native hyaline cartilage with its architecture and zonal arrangement has yet to be reproduced, the benefit, characteristics, and durability of this “hyaline-like” cartilage repair tissue remain unknown. The current literature available does not address the necessity for all chondral lesions to be filled with normal stratified hyaline cartilage. Rigorous clinical studies need to be performed to examine why some lesions with fibrocartilage fill may produce adequate patient-reported outcomes while others will have a positive clinical result only with hyaline-like cartilage. Attempts at reproduction of a true hyaline cartilage continue.
Although marrow stimulation techniques continue to play a large role in the treatment of specific chondral injuries, newer techniques including ACI, osteochondral allografts, and osteochondral autografts have been developed. We have described the development and early to midterm clinical results of such techniques for treatment of chondral injuries. Randomized, prospective studies with adequate power comparing these techniques to one another are still lacking, and it remains a challenge for the surgeon treating patients with injuries of the articular surfaces to reconcile the literature available and make evidence-based decisions.
Until these much-needed rigorous clinical trials are conducted and reported, treatment decisions will have to be made on the available literature. We have assimilated the literature on articular cartilage injuries along with our experience to help provide guidelines for treatment of these difficult injuries. Treatment decision-making must take into consideration patient goals, physical demands, expectations, and perceptions, as well as defect size, depth, location, chronicity, previous treatments and response, and concomitant pathology.
References
Ahmad CS, Cohen ZA, Levine WN, Ateshian GA, Mow VC. Biomechanical and topographic considerations for autologous osteochondral grafting in the knee. Am J Sports Med. 2001;29:201–206.
Ahmed TA, Hincke MT. Strategies for articular cartilage lesion repair and functional restoration. Tissue Eng Part B Rev. 2010;16:305–329.
Bobic V, Morgan C, Carter T. Osteochondral autologous graft transfer. Oper Tech Sports Med. 2000;8:168–178.
Bonner KF, Daner W, Yao JQ. 2-year postoperative evaluation of a patient with a symptomatic full-thickness patellar cartilage defect repaired with particulated juvenile cartilage tissue. J Knee Surg. 2010;23:109–114.
Brittberg M, Peterson L. Introduction to an articular cartilage classification. ICRS Newsletter. 1998;1:5–8.
Brittberg M, Winalski CS. Evaluation of cartilage injuries and repair. J Bone Joint Surg Am. 2003;85(Suppl 2):58–69.
Bugbee WD, Convery FR. Osteochondral allograft transplantation. Clin Sports Med. 1999;18:67–75.
Bujia J, Alsalameh S, Naumann A, Wilmes E, Sittinger M, Burmester GR. Humoral immune response against minor collagens Type IX and XI in patients with cartilage graft resorption after reconstructive surgery. Ann Rheum Dis. 1994;53:229–234.
Chen H, Sun J, Hoemann CD, Lascau-Coman V, Ouyang W, McKee MD, Shive MS, Buschmann MD. Drilling and microfracture lead to different bone structure and necrosis during bone-marrow stimulation for cartilage repair. J Orthop Res. 2009;27:1432–1438.
Chu CR, Convery FR, Akeson WH, Meyers M, Amiel D. Articular cartilage transplantation: clinical results in the knee. Clin Orthop Relat Res. 1999;360:159–168.
Chubinskaya S, Merrihew C, Cs-Szabo G, Mollenhauer J, McCartney J, Rueger DC, Kuettner KE. Human articular chondrocytes express osteogenic protein-1. J Histochem Cytochem. 2000;48:239–250.
Cohen NP, Foster RJ, Mow VC. Composition and dynamics of articular cartilage: structure, function, and maintaining healthy state. J Orthop Sports Phys Ther. 1998;28:203–215.
Cole BJ, Frederick RW, Levy AS, Zaslav KR. Management of a 37 year-old man with recurrent knee pain. J Clin Outcomes Manag. 1999;6:46–57.
Curl WW, Krome J, Gordon ES, Rushing J, Smith BP, Poehling GG. Cartilage injuries: a review of 31,516 knee arthroscopies. Arthroscopy. 1997;13:456–460.
Davidson PA, Rivenburgh DW, Dawson PE, Rozin R. Clinical, histologic, and radiographic outcomes of distal femoral resurfacing with hypothermically stored osteoarticular allografts. Am J Sports Med. 2007;35:1082–1090.
Derrett S, Stoeks E, James M, Bartlett W, Bentley G. Costs and health status outcomes following autologous chondrocyte implantation (ACI) and mosaicplasty: costs and health status outcomes. J Bone Joint Surg Br. 2006;88:254.
Ficat RP, Ficat C, Gedeon P, Toussaint JB. Spongialization: a new treatment for diseased patellae. Clin Orthop Relat Res. 1979;144:74–83.
Fortier LA, Potter HG, Rickey EJ, Schnabel LV, Foo LF, Chong LR, Stokol T, Cheetham J, Nixon AJ. Concentrated bone marrow aspirate improves full-thickness cartilage repair compared with microfracture in the equine model. J Bone Joint Surg Am. 2010;92:1927–1937.
Friedlaender GE. Immune responses to osteochondral allografts: current knowledge and future directions. Clin Orthop Relat Res. 1983;174:58–68.
Friedlaender GE, Horowitz MC. Immune responses to osteochondral allografts: nature and significance. Orthopedics. 1992;15:1171–1175.
Friedlaender GE, Strong DM, Sell KW. Studies on the antigenicity of bone. II. Donor-specific anti-HLA antibodies in human recipients of freeze-dried allografts. J Bone Joint Surg Am. 1984;66:107–112.
Garretson R, Katolik L, Verma N, Beck P, Bach B, Cole B. Contact pressure at osteochondral donor sites in the patellofemoral joint. Am J Sports Med. 2004;32:967–974.
Ghazavi MT, Pritzker KP, Davis AM, Gross AE. Fresh osteochondral allografts for post-traumatic osteochondral defects of the knee. J Bone Joint Surg Br. 1997;79:1008–1013.
Gomoll A, Probst C, Farr J, Cole B, Minas T. Use of a Type I/III bilayer collagen membrane decreases reoperation rates for symptomatic hypertrophy after autologous chondrocyte implantation. Am J Sports Med. 2009;37:205–235.
Gomoll AH, Kang RW, Chen AL, Cole BJ. Triad of cartilage restoration for unicompartmental arthritis treatment in young patients: meniscus allograft transplantation, cartilage repair and osteotomy. J Knee Surg. 2009;22:137–141.
Gross AE, Langer F, Houpt J, Pritzker K, Friedlaender G. Allotransplantation of partial joints in the treatment of osteoarthritis of the knee. Transplant Proc. 1976;8:129–132.
Gross AE, Silverstein EA, Falk J, Falk R, Langer F. The allotransplantation of partial joints in the treatment of osteoarthritis of the knee. Clin Orthop Relat Res. 1975;108:7–14.
Hangody L, Füles P. Autologous osteochondral mosaicplasty for the treatment of full-thickness defects of weight-bearing joints: ten years of experimental and clinical experience. J Bone Joint Surg Am. 2003;85(Suppl 2):25–32.
Hangody L, Kárpáti Z. [New possibilities in the management of severe circumscribed cartilage damage in the knee] [in Hungarian]. Magy Traumatol Ortop Kezseb Plasztikai Seb. 1994;37:237–243.
Hangody L, Kish G, Kárpáti Z, Udvarhelyi I, Szigeti I, Bély M. Mosaicplasty for the treatment of articular cartilage defects: application in clinical practice. Orthopedics. 1998;21:751–756.
Huntley JS, Bush PG, McBirnie JM, Simpson AH, Hall AC. Chondrocyte death associated with human femoral osteochondral harvest as performed for mosaicplasty. J Bone Joint Surg Am. 2005;87:351–360.
Irrgang JJ, Pezzullo D. Rehabilitation following surgical procedures to address articular cartilage lesions in the knee. J Orthop Sports Phys Ther. 1998;28:232–240.
Johnson LL. Arthroscopic abrasion arthroplasty historical and pathologic perspective: present status. Arthroscopy. 1986;2:54–69.
Jomha NM, Lavoie G, Muldrew K, Schachar NS, McGann LE. Cryopreservation of intact human articular cartilage. J Orthop Res. 2002;20:1253–1255.
Kang RW, Friel NA, Williams JM, Cole BJ, Wimmer MA. Effect of impaction sequence on osteochondral graft damage: the role of repeated and varying loads. Am J Sports Med. 2010;38:105–113.
Klein-Nulend J, Louwerse RT, Heyligers IC, Wuisman PI, Semeins CM, Goei SW, Burger EH. Osteogenic protein (OP-1, BMP-7) stimulates cartilage differentiation of human and goat perichondrium tissue in vitro. J Biomed Mater Res. 1998;40:614–620.
Klein-Nulend J, Semeins CM, Mulder JW, Winters HA, Goei SW, Ooms ME, Burger EH. Stimulation of cartilage differentiation by osteogenic protein-1 in cultures of human perichondrium. Tissue Eng. 1998;4:305–313.
Knutsen G, Drogset JO, Engebretsen L, Grøntvedt T, Isaksen V, Ludvigsen TC, Roberts S, Solheim E, Strand T, Johansen O. A randomized trial comparing autologous chondrocyte implantation with microfracture: findings at five years. J Bone Joint Surg Am. 2007;89:2105–2112.
Knutsen G, Engebretsen L, Ludvigsen TC, Drogset JO, Grøntvedt T, Solheim E, Strand T, Roberts S, Isaksen V, Johansen O. Autologous chondrocyte implantation compared with microfracture in the knee: a randomized trial. J Bone Joint Surg Am. 2004;86:455–464.
Koh JL, Wirsing K, Lautenschlager E, Zhang LO. The effect of graft height mismatch on contact pressure following osteochondral grafting: a biomechanical study. Am J Sports Med. 2004;32:317–320.
Kreuz PC, Erggelet C, Steinwachs MR, Krause SJ, Lahm A, Niemeyer P, Ghanem N, Uhl M, Südkamp N. Is microfracture of chondral defects in the knee associated with different results in patients aged 40 years or younger? Arthroscopy. 2006;22:1180–1186.
Lee SJ, Aadalen KJ, Malaviya P, Lorenz EP, Hayden JK, Farr J, Kang RW, Cole BJ. Tibiofemoral contact mechanics after serial medial meniscectomies in the human cadaveric knee. Am J Sports Med. 2006;34:1334–1344.
Lexer E. The use of free osteoplasty together with trials on arthrodesis and joint transplantation [in German]. Archiv fur klin Chirurgie. 1908;86:939–954.
Lexer E. Joint transplantation and arthroplasty. Surg Gynecol Obstet. 1925;40:782–809.
Lexer E. The use of free osteoplasty together with trials on arthrodesis and joint transplantation. Archiv fur klin Chirurgie. 1908;86:939–954. Clin Orthop Relat Res. 2008;466:1771–1776.
Mainil-Varlet P, Aigner T, Brittberg M, Bullough P, Hollander A, Hunziker E, Kandel R, Nehrer S, Pritzker K, Roberts S, Stauffer E; International Cartilage Repair Society. Histological assessment of cartilage repair: a report by the Histology Endpoint Committee of the International Cartilage Repair Society (ICRS). J Bone Joint Surg Am. 2003;85(Suppl 2):45–57.
Malinin TI, Mnaymneh W, Lo HK, Hinkle DK. Cryopreservation of articular cartilage: ultrastructural observations and long-term results of experimental distal femoral transplantation. Clin Orthop Relat Res. 1994;303:18–32.
McCulloch PC, Kang RW, Sobhy MH, Hayden JK, Cole BJ. Prospective evaluation of prolonged fresh osteochondral allograft transplantation of the femoral condyle: minimum 2-year follow-up. Am J Sports Med. 2007;35:411–420.
McGinty G, Irrgang JJ, Pezzullo D. Biomechanical considerations for rehabilitation of the knee. Clin Biomech (Bristol). 2000;15:160–166.
McNickle AG, Provencher MT, Cole BJ. Overview of existing cartilage repair technology. Sports Med Arthrosc. 2008;16:196–201.
Minas T. Chondrocyte implantation in the repair of chondral lesions of the knee: economics and quality of life. Am J Orthop. 1998;27:739–744.
Nho SJ, Pensak MJ, Seigerman DA, Cole BJ. Rehabilitation after autologous chondrocyte implantation in athletes. Clin Sports Med. 2010;29:267–282, viii.
Niemeyer P, Köstler W, Salzmann GM, Lenz P, Kreuz PC, Südkamp NP. Autologous chondrocyte implantation for treatment of focal cartilage defects in patients age 40 years and older: a matched-pair analysis with 2-year follow-up. Am J Sports Med. 2010;38:2410–2416.
O’Driscoll SW, Keeley FW, Salter RB. The chondrogenic potential of free autogenous periosteal grafts for biological resurfacing of major full-thickness defects in joint surfaces under the influence of continuous passive motion: an experimental investigation in the rabbit. J Bone Joint Surg Am. 1986;68:1017–1035.
Outerbridge RE. The etiology of chondromalacia patellae. J Bone Joint Surg Br. 1961;43:752–757.
Pallante AL, Bae WC, Chen AC, Görtz S, Bugbee WD, Sah RL. Chondrocyte viability is higher after prolonged storage at 37 degrees C than at 4 degrees C for osteochondral grafts. Am J Sports Med. 2009;37(Suppl 1):24S–32S.
Peterson L, Brittberg M, Kiviranta I, Akerlund EL, Lindahl A. Autologous chondrocyte transplantation: biomechanics and long-term durability. Am J Sports Med. 2002;30:2–12.
Peterson L, Menche D, Grande D, Klein M, Burmester G, Pugh J, Pitman M. Chondrocyte transplantation—an experimental model in the rabbit. Trans Orthop Res Soc. 1984;9:218.
Peterson L, Minas T, Brittberg M, Nilsson A, Sjögren-Jansson E, Lindahl A. Two- to 9-year outcome after autologous chondrocyte transplantation of the knee. Clin Orthop Relat Res. 2000;374:212–234.
Pridie K. A method of resurfacing osteoarthritic knee joints. J Bone Joint Surg Am. 1959;41:618–619.
Pritzker KP, Gross AE, Langer F, Luk SC, Houpt JB. Articular cartilage transplantation. Hum Pathol. 1977;8:635–651.
Pylawka TK, Wimmer M, Cole BJ, Virdi AS, Williams JM. Impaction affects cell viability in osteochondral tissues during transplantation. J Knee Surg. 2007;20:105–110.
Reinold MM, Wilk KE, Macrina LC, Dugas JR, Cain EL. Current concepts in the rehabilitation following articular cartilage repair procedures in the knee. J Orthop Sports Phys Ther. 2006;36:774–794.
Rosenberger RE, Gomoll AH, Bryant T, Minas T. Repair of large chondral defects of the knee with autologous chondrocyte implantation in patients 45 years or older. Am J Sports Med. 2008;36:2336–2344.
Rue JP, Yanke AB, Busam ML, McNickle AG, Cole BJ. Prospective evaluation of concurrent meniscus transplantation and articular cartilage repair: minimum 2-year follow-up. Am J Sports Med. 2008;36:1770–1778.
Salter RB, Simmonds DF, Malcolm BW, Rumble EJ, MacMichael D, Clements ND. The biological effect of continuous passive motion on the healing of full-thickness defects in articular cartilage: an experimental investigation in the rabbit. J Bone Joint Surg Am. 1980;62:1232–1251.
Saris DBF, Vanlauwe J, Victor J, Haspl M, Bohnsack M, Fortems Y, Vandekerckhove B, Almqvist KF, Claes T, Handelberg F, Lagae K, van der Bauwhede J, Vandenneucker H, Yang KG, Jelic M, Verdonk R, Veulemans N, Bellemans J, Luyten FP. Characterized chondrocyte implantation results in better structural repair when treating symptomatic cartilage defects of the knee in a randomized controlled trial versus microfracture. Am J Sports Med. 2008;36:235–246.
Sirlin CB, Brossmann J, Boutin RD, Pathria MN, Convery FR, Bugbee W, Deutsch R, Lebeck LK, Resnick D. Shell osteochondral allografts of the knee: comparison of MR imaging findings and immunologic responses. Radiology. 2001;219:35–43.
Steadman JR, Briggs KK, Rodrigo JJ, Kocher MS, Gill TJ, Rodkey WG. Outcomes of microfracture for traumatic chondral defects of the knee: average 11-year follow-up. Arthroscopy. 2003;19:477–484.
Steadman JR, Rodkey WG, Rodrigo JJ. Microfracture: surgical technique and rehabilitation to treat chondral defects. Clin Orthop Relat Res. 2001;391(Suppl):S362–S369.
Steinwachs M. New technique for cell-seeded collagen-matrix-supported autologous chondrocyte transplantation. Arthroscopy. 2009;25:208–211.
Williams JM, Virdi AS, Pylawka TK, Edwards RB, Markel MD, Cole BJ. Prolonged-fresh preservation of intact whole canine femoral condyles for the potential use as osteochondral allografts. J Orthop Res. 2005;23:831–837.
Williams SK, Amiel D, Ball ST, Allen RT, Wong VW, Chen AC, Sah RL, Bugbee WD. Prolonged storage effects on the articular cartilage of fresh human osteochondral allografts. J Bone Joint Surg Am. 2003;85:2111–2120.
Xia Z, Murray D, Hulley PA, Triffitt JT, Price AJ. The viability and proliferation of human chondrocytes following cryopreservation. J Bone Joint Surg Br. 2008;90:1245–1248.
Yagishita K, Sekiya I, Sakaguchi Y, Shinomiya K, Muneta T. The effect of hyaluronan on tendon healing in rabbits. Arthroscopy. 2005;21:1330–1336.
Yagishita K, Thomas BJ. Use of allograft for large Hill-Sachs lesion associated with anterior glenohumeral dislocation: a case report. Injury. 2002;33:791–794.
Zhang D, Johnson LJ, Hsu HP, Spector M. Cartilaginous deposits in subchondral bone in regions of exposed bone in osteoarthritis of the human knee: histomorphometric study of PRG4 distribution in osteoarthritic cartilage. J Orthop Res. 2007;25:873–883.
Author information
Authors and Affiliations
Corresponding author
Additional information
Dr. Farr has received research or institutional support from Zimmer, Inc (Warsaw, IN) and DePuy Mitek, Inc (Raynham, MA); miscellaneous nonincome support, commercially derived honoraria, or other nonresearch related-funding from Zimmer; has received royalties from DePuy Mitek; and is a consultant/advisory board member for Johnson and Johnson Co (New Brunswick, NJ) and Zimmer. Dr. Cole has received research or institutional support from Zimmer, DePuy Mitek, and Arthrex, Inc (Naples, FL); has received royalties from Zimmer and DePuy Orthopaedics, Inc (Warsaw, IN); and is a consultant for Zimmer and DePuy. Each additional author certifies that he has no commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
This work was performed at the OrthoIndy Cartilage Restoration Center of Indiana.
About this article
Cite this article
Farr, J., Cole, B., Dhawan, A. et al. Clinical Cartilage Restoration: Evolution and Overview. Clin Orthop Relat Res 469, 2696–2705 (2011). https://doi.org/10.1007/s11999-010-1764-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-010-1764-z