
Abstract
Background/rationale
A 10-year survivorship of 100% was reported for patients with PFC cruciate-retaining prostheses. Beyond 10 years, we observed additional polyethylene wear likely related to thin liners gamma-irradiated in air and were concerned this wear might predispose to implant construct failure.
Questions/purposes
We therefore determined (1) the functional scores at a minimum of 15 years followup, (2) rates of radiographic failure, (3) overall revision rates, and (4) mode of failure after 10 years and the fate of the revised implants.
Methods
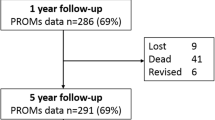
We retrospectively reviewed 75 patients with 101 press-fit condylar posterior cruciate-retaining prostheses. At a minimum followup of 15 years, 35 patients (47 knees) were living and evaluated clinically. No patients were lost to followup.
Results
There were no revisions during the first 11 years and six reoperations subsequently were performed in five patients (6% overall rate of revision but 12.8% in patients who survived more than 15 years). Three of six revisions had concerning liner wear at 10 years and all six were revised for polyethylene wear. Polyethylene exchange was performed in four of the five patients who underwent revisions, all of whom were doing well at an average of 7.2 years (range, 4.7–9.1 years) after the revision procedure.
Conclusions
At long-term followup, the overall revision rate remained low (6%). For patients surviving 15 years or more, the rate of revision was 12.8% and all revisions were secondary to aseptic sequelae of polyethylene wear. All revisions occurred more than 10 years after the initial procedures.
Level of Evidence
Level IV, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The press-fit condylar TKA system (PFC; Johnson and Johnson, Raynham, MA) has been in use since 1984 [30]. The PFC system is one of several second-generation prostheses modified from the total condylar and kinematic total knee prostheses. In addition to modifications designed to improve flexion and patellofemoral mechanics, the PFC and other contemporary prostheses included modularity of the tibial component.
The PFC prosthesis was originally a cruciate-retaining design. Consistent with general cruciate-retaining TKA design principles, the PFC originally used a relatively flat, nonconforming tibiofemoral interface [30]. Thin polyethylene inserts were used to maintain anatomic joint line position and preserve proximal tibial bone. Intermediate and preliminary long-term studies of this prosthesis have had revision rates for aseptic sequelae of polyethylene wear ranging from 1% to 3.8% at 8 to 17 years followup [6, 13, 20, 27, 29].
Modularity in TKA offers advantages, including increased intraoperative versatility and polyethylene exchange, as a less destructive and potentially cost-effective option for revision. However, drawbacks of modularity such as backside wear also have been reported [12, 14, 16, 25]. Some surgeons have questioned the appropriateness of polyethylene exchange as a revision technique, particularly in cases of accelerated polyethylene wear [1, 15]. Early polyethylene failure is likely related to technical issues such as malalignment and instability. Simple polyethylene exchange would not address the underlying abnormality. Still, polyethylene exchange is advocated for knees with well-fixed components [21].
One hundred percent 10-year survivorship in a cohort of patients with PFC cruciate-retaining prostheses followed at 5-year intervals was reported [20, 31]. The clinical scores and radiographic evaluation, as described by the Knee Society, at each interval were reported. Beyond 10 years, failures of the polyethylene were observed. The polyethylene was thin (8 mm in 77% of the knees), and there was concern this would predispose the implant to failure. Because the failure mode appeared limited to, or initiated by, polyethylene failure, it is important to determine the long-term survivorship with revision as an end point for polyethylene exchange.
The purpose of the current study was to address: (1) the functional scores at a minimum of 15 years followup, (2) rates of radiographic failure, (3) the overall revision rates, (4) the mode of failure after 10 years, and the fate of implants that were revised.
Patients and Methods
One of the authors (SSK) designed this prospective study in 1988, at the completion of fellowship training, before beginning private practice in Des Moines, IA. It was intended to report, at 5-year intervals, the first 100 TKAs using the cemented posterior cruciate-retaining PFC. These cases were performed between November 1988 and January 1991. The final patient required bilateral TKAs such that 101 cemented primary TKAs (75 patients) with the posterior cruciate-retaining PFC prosthesis were included. During this interval, seven additional TKAs were performed. Six patients with an insufficient posterior cruciate ligament underwent posterior stabilized TKAs, and one hybrid PFC (uncemented femoral component, with unresurfaced patella) was performed in a patient younger than 40 years. The posterior stabilized components included two with Insall-Burstein (Zimmer, Warsaw, IN) and four with posterior-stabilized PFC knee prostheses. The average age of the patients at the time of surgery was 71.2 years (range, 52.2–88.8 years). Study participants included 44 females (59 knees) and 31 males (42 knees). There were 52 right knees (51%) and 49 left knees (49%). Twenty-six patients (35%) had bilateral TKAs. Of these, six patients had the bilateral TKAs performed during one surgical procedure. Diagnoses included primary osteoarthritis in 86 knees (85%), rheumatoid arthritis in 13 (13%), avascular necrosis in one (1%), and posttraumatic osteoarthritis in one (1%). Previous knee procedures had been performed in 11 patients before the index TKA. These included six arthroscopies, three meniscectomies, and two patellectomies. The minimum followup was 15 years (mean, 16.6 years; range, 15–18.1 years). At a minimum of 15 years after the primary procedure, 35 patients (47 knees) were living and 40 patients (54 knees) were dead. No patients were lost to followup. After locating living patients, consent for study participation was obtained as per the protocol previously approved by the Institutional Review Board.
All components were cemented. The modular metal-backed tibial tray was titanium, and the femoral component was manufactured with a cobalt-chrome alloy. A three-peg, all-polyethylene patella was used in all procedures except two. In these two procedures, the patella was not resurfaced because prior patellectomy had been performed. A posterior-lipped polyethylene insert with minimally raised anterior and posterior borders and a large radius of curvature was used in all procedures. During the interval of these procedures, a more conforming curved tibial insert became available but was not used in these patients. The thickness of the polyethylene insert was labeled as 8.0 mm (minimum thickness, 5.3 mm) in 78 knees (77%), 10.0 mm (minimal thickness, 8.0 mm) in 17 knees (17%), 12.5 mm (minimal thickness, 10 mm) in five knees (5%), and 15 mm (minimal thickness, 13.0 mm) in one knee (1%). Beginning in 1991, the manufacturer increased the minimal thickness of the 8.0-mm insert from 5.3 mm to 6.0 mm, but the thinner implant was used exclusively in this patient cohort. All components were gamma-irradiated in air.
Indications for revision at the orthopaedic practice performing the primary procedures included a painful knee with radiographic evidence of polyethylene wear. Intraoperatively, fixation of the tibial, femoral, and patellar components was assessed. If the components were well fixed and without obvious malalignment, revision consisted of simple polyethylene exchange. In the presence of additional component loosening or wear, the tibial, femoral, and patellar components were revised as appropriate.
One investigator (ASM) not involved in the surgical procedures and not receiving compensation from the implant manufacturer contacted all patients. All patients were encouraged to return to the clinic for full clinical and radiographic evaluations. Of the 35 patients (47 knees) known to be living at the time of followup, all were located, and the survivorship or need for revision of the prosthesis was confirmed. Because of major dementia, three patients (four knees) were unable to participate in the full telephone assessment of clinical status such that discussion was limited to confirmation that the original implant was not painful with ambulation. Therefore, only 32 patients (43 knees) completed the full telephone evaluation. Clinical outcome measures included the pain and functional components of the Knee Society scoring system [23] and the WOMAC [3]. Physical examinations of the 11 patients (15 knees) returning to the clinic included the physical examination components of the Knee Society scoring system [17].
We obtained standing AP, lateral, and Merchant views. For patients unable or unwilling to return for full clinical evaluation, local or portable radiographic evaluation was arranged. Radiographic followup was obtained for 28 patients (38 knees, 81% of knees in living patients).
All radiographs were evaluated using the Knee Society protocol [17] by two authors (JJC, ASM) not involved with the surgery or subsequent care with findings by consensus.
Among the patients who had died, contact was made with a surviving relative for all patients. In all cases, the survival of the prosthesis at the time of the patient’s death was confirmed. In addition, no pending revisions or revision indications were identified at the time of death. These determinations were made at either the time of the 9- to 12-year study [20] or as part of the current study.
Kaplan–Meier survivorship analysis with 95% confidence intervals was performed using SPSS 13.0 software (SPSS, Chicago, IL) with any revision and component-specific revision as the end points. The Cox proportional hazard regression analysis was used to assess correlation of patient age and polyethylene implant thickness with need for revision.
Cost analysis was performed by extrapolation of data from a recently conducted cost-analysis study performed, in part, by one of the authors (KJB) [5]. Relying on data from four large US orthopaedic centers, the cost-analysis study assigned cost estimates for TKA and various revision options, including simple liner exchange. These data were extrapolated to estimate cost savings for the study cohort in the current study (Appendix 1). In addition, relying on actual use data obtained from the implant manufacturer for 1990, we estimated the nationwide cost savings of modularity in this implant assuming a similar revision rate across the country.
Results
Overall, average WOMAC scores (corrected to higher score higher outcome) were 98 of 100 (95% confidence interval, 96.5–99.5) for the pain component, 95 of 100 (90.8–99.4) for the stiffness component, and 60 of 100 (51.8–68.0) for the functional component. Knee Society average pain score was 48 of 50 (47.1–49.5), and average function score was 48 of 100 (39.8–56.5). The average age of the patients at the time of last clinical followup was 82.5 years. Functional limitations invariably were attributed primarily to other musculoskeletal or systemic morbidities, not the operative knee(s).
Of the 32 nonrevised knees evaluated radiographically, 13 had radiolucent lines observed on radiographic evaluation. There was only one radiolucent line greater than 1 mm identified, an isolated 2-mm radiolucency in Zone 2 of the femur. There were no circumferential radiolucencies identified. Early changes consistent with osteolysis were evident in four patients. In three of four patients, the osteolysis totaled less than 1 cm2 and was limited to one tibial or femoral zone. The most extensive osteolysis was seen in a patient who already had revision of the polyethylene liner and femoral and patellar components on the contralateral side. The unrevised knee had extensive osteolytic findings, including Zones 3, 4, and 5 of the femur and Zone 1 of the AP tibia. There were no radiolucent lines. Clinically, the patient reported no current pain, swelling, or functional limitation with respect to the unrevised or revised knee.
Six reoperations were performed in five patients (Table 1). The rate of revision therefore was 6% (six of 101 knees) at a minimum of 15 years. All revisions were performed for aseptic sequelae of polyethylene wear and occurred greater than 11 years after the index procedure. Survivorship (Fig. 1) for revision for any reason was 91% at 18 years (95% confidence intervals, 0.81–0.96). All revisions occurred in patients with 8-mm polyethylene inserts. Of the 41 unrevised knees, the polyethylene thickness was 8 mm in 31 patients, 10 mm in eight patients, and 12.5 mm in two patients. We observed an association (p = 0.051) of polyethylene thickness with revision. Those with 8-mm thickness were more likely to need revision surgery.

Kaplan–Meier survivorship curves with accompanying 95% confidence intervals for the following end points show: (A) survivorship from any revision, (B) survivorship from liner revision, (C) survivorship from tibial component revision, (D) survivorship from femoral component revision, and (E) survivorship from patellar component revision.
There were three revision scenarios: isolated polyethylene exchange (two knees), femoral revision with polyethylene exchange (two knees, one included the patella), and revision of all components (two knees). None of the six revised knees in five patients had clinical or radiographic signs of failure at an average of 6.7 years (range, 4.7–9.1 years) following revision.
Discussion
A 100% 10-year survivorship was reported for a cohort of patients with PFC cruciate-retaining prostheses followed at 5-year intervals [20, 31]. The current study presents survivorship at a minimum of 15 years along with the previously reported clinical and radiographic variables. There are two aspects of our analysis, evaluation of the surviving knees from the initial study group and analysis of the six failures. The polyethylene was thin (8 mm in 77% of the knees) and we were concerned this predisposed the implant to failure. Because the failure mode appeared limited to, or initiated by, polyethylene failure, we were concerned about the short-term survivorship for polyethylene exchange. With the current minimum 15-year evaluation, we attempted to address: (1) functional scores, (2) rates of radiographic failure, (3) overall revision rates, (4) mode of failure after 10 years, and the fate of implants that had been revised.
We acknowledge several limitations of our study. First, is the small number of failures available to study. Because the modes of failure varied, we were unable to perform subcohort analyses. However, the data suggest high short-term survival for patients with polyethylene exchange. Second, this was an older population. The average age of the overall cohort at the time of the index procedure was 71.2 years, similar to other contemporary TKA cohorts (Table 2). Thus, we had relatively few patients to follow, although for most patients the implant provided function for the duration of their lives.
Strengths of the study include the fact that the operating surgeon (SSK) was not involved in the followup or evaluation of the long-term results. One of the other authors (DDG) performed all the clinical followups during the 15-year interval and two other authors (JJC and ASM) performed all of the radiographic analyses and data collection. All patients were called and requested to return for followup at 5, 10, and 15 years after their surgery.
Numerous TKA cohorts have been followed for 15 years or longer with survivorship rates consistently exceeding 90% [7, 24, 26, 28, 32] (Table 2). Although 15-year studies on modular TKA were reported [13, 27], there are relatively few studies, especially when one considers the frequency with which modular TKA components are used. In addition, as compared with our study, the cohort of Rodricks et al. had more limited radiographic followup [27], and that of Dixon et al. included hybrid replacements [13]. We obtained clinical followup information for 91% of our living patients (32 patients, 43 knees). Three patients (four knees) had dementia. The Knee Society scores obtained in this study were comparable to those of other studies with similar followup (Table 2). We also report WOMAC scores, which were not reported in similar studies.
We obtained radiographic followup for 80% of our living patients (28 patients, 38 knees). Radiolucent lines were present in 34% and were incomplete and nonprogressive. The range of radiolucent lines has varied in reports of the same implant (13–62%); however, in each of those studies, the lines were incomplete and nonprogressive [13, 27]. All studies reported concerns regarding osteolysis [13, 27]. Early changes consistent with osteolysis were evident in four patients in our study.
In the current study, the PFC prosthesis performed well with respect to survivorship (Fig. 1). Fetzer et al. previously reported a survivorship of 100% at 10 years [20]. All revisions occurred greater than 11 years after the index procedure. All failures were related to polyethylene wear leading to osteolysis and/or loosening. Our survivorship, radiographic, and clinical outcomes are comparable to those of other studies with similar 15-year followups, including studies of similar prostheses designs (Table 2). Unlike other studies with a mixture of failure modes (infection, patellar failure), our failures can be attributed to the durability of the polyethylene. In two of the six failures, intervention occurred before major osteolysis. When osteolysis compromised component fixation, the femoral component was involved in all four cases, the tibial component in two of those four. Although we had small numbers, our finding that osteolysis was more likely to occur on the femoral side also was reported by Griffin et al. [21].
In our cohort, relatively thin polyethylene was implanted. In 78 of 101 knees, an 8-mm insert was implanted. However, taking into account the tibial base plate, the actual minimum thickness of an 8-mm insert implanted was 5.3 mm. All failures occurred in patients with 8-mm inserts although given the small numbers of thicker (10, 12.5, 15 mm) inserts implanted we observed only a p = 0.051 level of significance. The PFC implant studied here also uses a relatively flat, nonconforming surface, particularly the posterior-lipped insert. Despite the potentially deleterious effects of thin [2, 10, 22, 34], flat [4, 19] inserts on polyethylene wear, the revision rates in our patients were low and occurred late.
Our study cohort consisted entirely of polyethylene inserts gamma-irradiated in air, a process that has been associated with increased rates of polyethylene wear [9, 11, 33], particularly in combination with increased shelf life of polyethylene before implantation [8, 9, 18]. The catastrophic early failure observed in PFC knee prostheses of the same design implanted after 1991 [18] was not evident in our cohort, which included patients who had TKAs performed just before 1991. Polyethylene shelf life data were not available for analysis in the current study.
At 6.7 years followup (range, 4.7–9.1 years), we found no evidence of clinical or radiographic concerns in the six patients who had undergone revision. Although two of the six patients had complete revisions, four were able to benefit from the modularity of the tibial tray. The potential economic impact of modular exchange versus complete revision is presented in Appendix 1. The limitations to the cost analysis are that it is based on the assumption that the initial decision at the time of primary total knee replacement was to use a more expensive modular device versus a nonmodular device, and that the analysis was based on our small numbers of overall revisions (six).
Although two studies reported high rates of early failure after polyethylene exchange revision TKA [1, 15], our four patients undergoing polyethylene exchange (two isolated polyethylene exchange and two polyethylene exchange associated with femur/patellar revision) reported no knee pain and had no evidence of progressive radiographic abnormality at an average of 7.2 years (range, 4.7–9.1 years) from the revision procedure. This was possible because of the regular followup (every 5 years) of our patients. There is one other study advocating consideration of modular exchange when the component fixation is intact. In a recent retrospective review, an 84% success rate of polyethylene exchange at a minimum of 24 months postrevision in well-aligned knees was reported [21].
The PFC modular, cruciate-retaining total knee prostheses performed well clinically and radiographically at a minimum of 15 years postoperatively. Osteolysis is recognized as the dominant mode of aseptic failure in TKAs, particularly those in which modular-design prostheses are implanted [9, 18]. Because osteolysis can be asymptomatic for a relatively long time, close followup, especially after 10 years, is warranted. Modularity does offer the advantage of a low-morbidity, cost-saving option for revision TKA (Appendix 1.) Use of this potential benefit requires close clinical followup of patients undergoing TKA.
References
Babis GC, Trousdale RT, Morrey BF. The effectiveness of tibial insert exchange in revision total knee arthroplasty. J Bone Joint Surg Am. 2002;84:64–68.
Bartel DL, Bicknell VL, Wright TM. The effect of conformity, thickness, and material on stresses in ultra-high molecular weight components of total joint replacement. J Bone Joint Surg Am. 1986;68:1041–1051.
Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: a health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15:1833–1840.
Benjamin J, Szivek J, Dersam G, Persselin S, Johnson R. Linear and volumetric wear of tibial inserts in posterior cruciate-retaining knee arthroplasties. Clin Orthop Relat Res. 2001;392:131–138.
Bozic KJ, Rubash HE, Sculco TP, Berry DJ. An analysis of Medicare payment policy for total joint arthroplasty. J Arthroplasty. 2008;23(6 suppl 1):133–138.
Buehler KO, Venn-Watson E, D’Lima DD, Colwell CW Jr. The press-fit condylar total knee system: 8- to 10-year results with a posterior cruciate-retaining design. J Arthroplasty. 2000;15:698–701.
Callaghan JJ, O’Rourke MR, Iossi MF, Liu SS, Goetz DD, Vittetoe AV, Sullivan PM, Johnston RC. Cemented rotating-platform total knee replacement: a concise follow-up, at a minimum of fifteen years, of a previous report. J Bone Joint Surg Am. 2005;87:1995–1998.
Collier MB, Engh CA Jr, Engh GA. Shelf age of the polyethylene tibial component and outcome of unicondylar knee arthroplasty. J Bone Joint Surg Am. 2004;86:763–769.
Collier MB, Engh CA Jr, McAuley JP, Engh GA. Factors associated with the loss of thickness of polyethylene tibial bearings after knee arthroplasty. J Bone Joint Surg Am. 2007;89:1306–1314.
Collier JP, Mayor MB, McNamara JL, Surprenant VA, Jensen RE. Analysis of the failure of 122 polyethylene inserts from uncemented tibial knee components. Clin Orthop Relat Res. 1991;273:232–242.
Collier JP, Sperling DK, Currier JH, Sutula LC, Saum KA, Mayor MB. Impact of gamma sterilization on clinical performance of polyethylene in the knee. J Arthroplasty. 1996;11:377–389.
Conditt MA, Stein JA, Noble PC. Factors affecting the severity of backside wear of modular tibial inserts. J Bone Joint Surg Am. 2004;86:305–311.
Dixon MC, Brown, RR, Parsch D, Scott RD. Modular fixed-bearing total knee arthroplasty with retention of the posterior cruciate ligament: a study of patients followed for a minimum of fifteen years. J Bone Joint Surg Am. 2005;87:598–603.
Engh GA, Dwyer KA, Hanes CK. Polyethylene wear of metal-backed tibial components in total and unicompartmental knee prostheses. J Bone Joint Surg Br. 1992;74:9–17.
Engh GA, Koralewicz LM, Pereles TR. Clinical results of modular polyethylene insert exchange with retention of total knee arthroplasty components. J Bone Joint Surg Am. 2000;82:516–523.
Engh GA, Lounici S, Rao AR, Collier MB. In vivo deterioration of tibial baseplate locking mechanisms in contemporary modular total knee components. J Bone Joint Surg Am. 2001;83:1660–1665.
Ewald FC. The Knee Society total knee arthroplasty roentgenographic evaluation and scoring system. Clin Orthop Relat Res. 1989;248:9–12.
Fehring TK, Murphy JA, Hayes TD, Roberts DW, Pomeroy DL, Griffin WL. Factors influencing wear and osteolysis in press-fit condylar modular total knee replacements. Clin Orthop Relat Res. 2004;428:40–50.
Feng EL, Stulberg SD, Wixson RL. Progressive subluxation and polyethylene wear in total knee replacements with flat articular surfaces. Clin Orthop Relat Res. 1994;299:60–71.
Fetzer GB, Callaghan JJ, Templeton JE, Goetz DD, Sullivan PM, Kelley SS. Posterior cruciate-retaining modular total knee arthroplasty: a 9–12 year follow-up investigation. J Arthroplasty. 2002;17:961–966.
Griffin WL, Scott RD, Dalury DF, Mahoney OM, Chiavetta JB, Odum SM. Modular insert exchange in knee arthroplasty for treatment of wear and osteolysis. Clin Orthop Relat Res. 2007;464:132–137.
Hirakawa K, Bauer TW, Stulberg BN, Wilde AH, Borden LS. Characterization of debris adjacent to failed knee implants of 3 different designs. Clin Orthop Relat Res. 1996;331:151–158.
Insall JN, Dorr LD, Scott RD, Scott WN. Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res. 1989;248:13–14.
Keating EM, Meding JB, Faris PM, Ritter MA. Long-term followup of nonmodular total knee replacements. Clin Orthop Relat Res. 2002;404:34–39.
Parks NL, Engh GA, Topoleski LD, Emperado J. The Coventry Award. Modular tibial insert micromotion: a concern with contemporary knee implants. Clin Orthop Relat Res. 1998;356:10–15.
Pavone V, Boettner F, Fickert S, Sculco TP. Total condylar knee replacement: a long-term followup. Clin Orthop Relat Res. 2001;388:18–25.
Rodricks DJ, Patil S, Pulido P, Colwell CW Jr. Press-fit condylar design total knee arthroplasty: fourteen to seventeen-year follow-up. J Bone Joint Surg Am. 2007;89:89–95.
Rodriguez JA, Bhende H, Ranawat CS. Total condylar knee replacement: a 20 year follow-up study. Clin Orthop Relat Res. 2001;388:10–17.
Schai PA, Thornhill TS, Scott RD. Total knee arthroplasty with the PFC system: results at a minimum of ten years and survivorship analysis. J Bone Joint Surg Br. 1998;80:850–858.
Scott RD, Thornhill TS. Press-fit condylar total knee replacement. Orthop Clin North Am. 1989;20:89–95.
Tooma GS, Kobs JK, Thomason HC 3rd, Kelley SS. Results of knee arthroplasty using the cemented press-fit condylar prosthesis: based on a preliminary report. Am J Orthop (Belle Mead NJ). 1995;24:831–834.
Vessely MB, Whaley AL, Harmsen WS, Schleck CD, Berry DJ. The Chitranjan Ranawat Award: Long-term survivorship and failure modes of 1000 cemented condylar total knee arthroplasties. Clin Orthop Relat Res. 2006;452:28–34.
White SE, Paxson RD, Tanner MG, Whiteside LA. Effects of sterilization on wear in total knee arthroplasty. Clin Orthop Relat Res. 1996;331:164–171.
Williams IR, Mayor MB, Collier JP. The impact of sterilization method on wear in knee arthroplasty. Clin Orthop Relat Res. 1998;356:170–180.
Author information
Authors and Affiliations
Corresponding author
Additional information
One of the authors (JJC) received royalties and is a consultant for DePuy; one of the authors (KJB) is a consultant for Integrated Healthcare Association, BC & BS Association, United Health Care, Center for Medicare & Medicaid Services, and Pacific Business Group on Health; and one of the authors (DDG) received research support from DePuy.
Each author certifies that his institution has approved the reporting of these cases, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation was obtained.
Appendix 1. Cost-analysis Data
Appendix 1. Cost-analysis Data
In a recent cost analysis study [5] with the modification of using Medicare reimbursement data instead of institution-specific data reported in the study, the average total cost for revision of all knee components was $22,218, and the cost of a simple liner exchange was $17,377. The cost of a liner exchange and femoral component revision was $18,995. Addition of a patellar revision did not add substantial cost to this procedure.
Our estimated 12% decrease in total revision costs was obtained by using the benefits of modularity. Extrapolation of the data to the nationwide cohort of PFC cruciate-retaining prostheses revealed an estimated total revision cost savings of $1,855,647 for PFC cruciate-retaining knees implanted during a 1-year period (1990). In considering any potential cost-saving measure, it is important to first ensure that the cost-saving measure does not portend a higher likelihood of a poor clinical outcome for the patient.
From January 1 to December 31, 1990 (a 1-year period encompassed by our study interval), 11,612 cruciate-retaining PFC prostheses were implanted in patients in the United States (data obtained from the manufacturer [Johnson and Johnson, Raynham, MA]). Assuming a 6% revision rate, the total revision burden for the nationwide cohort is 696 revisions. Based on a cost of $22,218 per revision and a 12% reduction in revision cost, modularity theoretically conferred an estimated total savings of $1,855,647 for all revisions of PFC cruciate-retaining knees implanted in 1990.
As compared with total revision, an estimated total cost savings of $4841 (22%) was gained for each simple liner exchange, and an estimated cost savings of $3223 (15%) was gained for each femoral/liner exchange. Therefore, modularity allowed an average of 18.5% reduction in cost for 66% of the revisions. This equates to a 12% reduction in overall revision costs for the cohort.
About this article
Cite this article
Malin, A.S., Callaghan, J.J., Bozic, K.J. et al. Routine Surveillance of Modular PFC TKA Shows Increasing Failures after 10 Years. Clin Orthop Relat Res 468, 2469–2476 (2010). https://doi.org/10.1007/s11999-010-1303-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-010-1303-y