
Abstract
Purpose of Review
Current technical advances enable the assessment of the complex changes in body fluid proteomes and thus allow for the discovery of biomarker signatures rather than just following differences of a single marker. In this review, we aim to summarize current approaches to discover and evaluate multi-biomarker panels for improved monitoring of chronic arthritis disease activity.
Recent Findings
Mass spectrometry and affinity proteomic methodologies have been used to identify biomarker panels in synovial fluid, serum, plasma, or urine of pediatric and adult chronic arthritis patients. Notably, despite the numerous efforts to develop new and better biomarker panels, very few have undergone extensive analytical and clinical validation and been adopted into routine use for patient benefit.
Summary
There remains a significant gap between discovery of chronic arthritis biomarker signatures and their validation for clinical use.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Currently, individual blood-based proteins are the most widespread diagnostic biomarkers used in medicine. Biological processes that occur within and between cells and tissues are commonly complex and regulated by multiple proteins, thus to fully understand the dynamics of biological processes, it is desirable to investigate whole proteomes. The “proteome” is a term, coined by Marc Wilkins and first used by Wasinger et al. in 1995, that defines the “total protein complement of a genome” at a given time [1]. It gave rise to the realization that proteome analysis or “proteomics” afforded huge opportunities for new and greater understanding of the role of proteins individually and as protein complexes and networks [2].
Advances in the latest proteomic technologies, software platforms and online repository databases have not only increased the capabilities of this field but also made them more accessible to clinical researchers. Although genomic and transcriptomic platforms are powerful alternatives, they are not useful for providing data to predict downstream events. More specifically, they cannot be used to predict what proteins will actually be expressed in tissue or biofluid, nor can they estimate at what levels. Finally, proteins are subject to a profusion of modifications, often requiring cleavage to become biologically active as well as a plethora of post-translational modifications. It is not possible to capture this information at the genomic level, rather it is the gene products themselves, i.e., proteins that provide the best clues into health and disease [3].
It is now widely recognized that there is significant need to develop tests that can be used in the (i) diagnosis, (ii) treatment, and (iii) management of arthritis and a common link between these clinical demands is that they aim to facilitate early and more appropriate intervention. Key to this is making an early accurate diagnosis and the expectation is that new protein biomarkers, measured in tissues or body fluids may support such diagnoses. It is also anticipated that given the heterogeneity of the disease and inter-individual differences, a panel (or signature) of proteins is more likely to be effective as a biomarker test [4].
An increasing number of biomarkers have been identified in what are termed “discovery” experiments but few if any have been translated to biomarker tests in routine clinical use [5]. The reasons for this lack of success are manifold and variable and now well described [6,7,8,9]. They range from inadequate discovery experiments which are poorly designed [10], the selection of incorrect candidates (from the many available) for further evaluation and the challenges in conducting appropriate analytically robust validation studies which provide convincing evidence of clinical utility [8, 10, 11]. When these challenges are combined with the difficulties associated with getting potential new tests used by the relevant clinical communities and perhaps more significantly finding routes for the adequate re-imbursement for new tests, it is perhaps not overly surprising that few new tests have emerged. This review summarizes recent advances in the use of proteomic technologies for protein biomarker panel discovery and validation and the translation of such proteome knowledge into applicable tools for the care of patients with chronic arthritis.
Protein Biomarker Discovery, Evaluation, and Validation
The starting point for many protein biomarker discovery experiments has been the application of proteomics—in its various forms—with the use of unbiased mass spectrometry-based approaches for protein identification and quantification having dominated to date. The emergence of novel protein discovery approaches such as the use of aptamer libraries, multiplexing of antibody-based methods, and the emergence of highly sensitive assays has offered additional hope for the discovery of new candidate biomarkers. However, with the exception of the impressive efforts to develop well characterized assays to several thousand proteins [10, 12], in many instances, these newer approaches have again focused on the measurement of relatively modest panels of previously well-studied proteins.
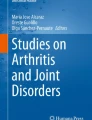
The biomarker development process can be divided into phases as schematically illustrated in Fig. 1 and as noted previously, a commonly recognized reason for “biomarker failure” is poor study design [4, 10, 11]. In general, data from observational studies is considered inferior, as results are often influenced by confounding factors. On the other hand, evidence derived from well-designed prospective cohort studies that follow patients longitudinally and in which cofounding factors may be considered and controlled for is notoriously difficult and expensive to execute [13,15,16,16]. Another factor that has limited biomarker test development is the choice of biological sample used in the discovery phase. It is well recognized that if biomarkers are to be adopted into routine clinical practice, the process used for their analysis should be minimally invasive. Ideally, a test should be based on an easily accessible biological sample such as blood (serum or plasma) that can be obtained following standardized operating procedures. Although in the context of rheumatology, synovial fluid and synovial tissue represent attractive samples to examine (since they are taken from the site of disease), they are less than ideal as routine test samples as they require more invasive collection procedures. It is for this practical reason that many of the new biomarkers reported in literature are not likely to reach clinical utility.

Exemplary schematic work flow of the development of a biomarker panel for clinical application in rheumatology
Proteomic Methodologies for Biomarker Discovery and Validation
Affinity Proteomics
The evaluation of biomarkers has classically relied on the development of antibody-based assays. Enzyme-linked immunosorbent assays (ELISAs) are one of the most widely used methods for clinical diagnostic protein biomarker measurements. ELISA is a singleplex assay that employs two antibodies for the capture and detection of a protein in a test sample. This immune assay concept is widely implemented in many clinical laboratory routines. ELISAs still remain the gold standard for the affinity-based detection/measurement of single analytes including in patients’ body fluids. The recently introduced digital ELISA represents the latest evolutionary step of this assay concept and achieves a 1000-fold increase in sensitivity compared to conventional ELISAs [17, 18•]. While ELISAs are highly valuable for the validation of selected single biomarkers, they are far less suitable during initial discovery or screening phases. Impressive efforts have been made to multiplex “ELISA” and in particular, the Luminex approach in which antibodies are covalently attached to fluorescent beads has achieved significant use for the measurement of multiplexed panels of candidate protein biomarkers. An alternative approach that has attracted significant attention and application particularly for measurement of proteins in biofluids such as serum or plasma involves the use of antibody, protein, or peptide arrays. In contrast to bead-based assays such as Luminex which rely on size and/or color-coded beads coated with analyte-specific capture reagents (antibodies, peptides), such arrays are set up in a planar formate where analyte-specific capture reagents (antibodies, peptides, and aptamers) are immobilized on a solid-phase surface (glass slides, microtiter plate wells). Both bead-based as well as planar arrays can provide the simultaneous (multiplexed) and rapid high-throughput measurement of multiple analytes in very little sample (μl amounts).
In spite of the advantages associated with these techniques, a wide variety of factors are known to affect the performance of antibodies or ligands used in these assays including temperature, pH, incubation times, and particularly cross-reactivity. More recent approaches as aptamer-based technologies (SOMAscan) or proximity ligation assays (PLA) are meant to mitigate cross-reactivity in multiplexed assay formats. Gold and colleagues developed DNA-based binders called aptamers that integrate chemically modified bases (SOMAmers) to optimize affinity and generate a greater binding diversity. The SOMAscan technology is capable of targeting up to 1129 proteins spanning 10 orders of magnitude [19]. The proximity ligation assay (PLA) or proximity elongation assay (PEA) aim to molecularly discriminate specific from unspecific binding [20, 21]. Each target requires to be bound by two antibodies tagged with DNA strands. The antibodies recognize distinct epitopes in close proximity to each other and upon simultaneous binding enable ligation of DNA strands, either assisted by a connector oligonucleotide or directly hybridized to each other by complementary sequences. After elongation, the newly formed DNA strands are amplified by PCR and transduced into a measurable signal [20, 21].
Mass Spectrometry
Mass spectrometry (MS) is a complex and versatile tool that can be used in combination with separation techniques for protein characterization. Liquid chromatography coupled to mass spectrometry (LC-MS/MS) is the most commonly used technique to support “shotgun proteomics” or “bottom up proteomics”—an approach where complex mixtures of proteins are first enzymatically cleaved into peptides which are then separated based on chemical or physical properties and analyzed using a mass spectrometer.
A major drawback associated with LC-MS/MS is that this technique can have limited sensitivity when investigations are carried out in highly complex samples, such as human serum. Serum is a biofluid of choice in clinical proteomics since it is (i) readily available and (ii) a rich source of biomarkers (containing proteins that are synthesized, secreted, shed, or lost from cells and tissues throughout the body). The complexity of the serum proteome exceeds the analytical capacity of even the most sensitive mass spectrometers [22]. Furthermore, serum presents additional analytical challenges as (i) approximately 96% of the total protein content of the fluid is represented by just 14 abundant proteins, which dominate in LC-MS/MS-based analysis of the fluid and (ii) the remaining proteins span a huge (> 12 orders of magnitude) dynamic range in their concentrations. The presence of a limited number of high abundant proteins interferes with the identification and quantification of low abundant proteins. It is estimated that up to 10,000 proteins may be present in serum, most of which are present in relatively low abundance [23] and may represent important markers of disease.
LC-MS/MS has also emerged as powerful tool for the identification of post-translational modifications on serum or plasma proteins as, i.e., phosphorylation, glycosylation or—relevant in rheumatology—citrullination [24]. However, despite the potential of proteomics to measure post-translationally modified proteins and the justified interest in identifying diagnostic biomarkers represented by such, there has also been very limited success in converting newly identified candidates to diagnostic tests. The difficulties associated with developing post-translationally modified proteins as biomarkers are compounded by the additional challenges associated with the pre-analytical stability of such modifications and the added difficulty in generating suitable protocols and reagents either to isolate the post-translationally modified form of the protein and/or in developing assays of requisite specificity [25].
Once candidate proteins have been identified, it has been common to continue their evaluation using assays for the individual proteins based on the use of antibodies. Given the time and cost of developing antibodies to “new” protein, this antibody-based evaluation of candidate biomarker proteins has, in practice, been biased towards candidates for which there may already be antibodies or assays available. Clearly, the disconnection between identifying large numbers of new candidate biomarkers by mass spectrometry-based approaches and subsequently evaluating them by conventional antibody-based approaches has represented a significant bottleneck in progressing new candidates to potential validated biomarker tests. The recent availability of a targeted mass spectrometry-based approach to simultaneously measure a relatively large number of proteins offers a solution to this significant bottleneck in the biomarker development process. This technique is called Multiple Reaction Monitoring (MRM). Importantly, MRM has several significant advantages:
-
i)
It supports simultaneous, robust, and specific analysis of hundreds of proteins (spanning 5 orders of magnitude) in a complex sample
-
ii)
It is relatively inexpensive to develop of MRM assays to 10’s if not 100’s of proteins (compared with the cost of developing antibody-based assays)
-
iii)
Assays can be developed and optimized rapidly (in days) when compared to the long times (months) taken to develop antibody-based assays
Taken together, these suggest that MRM represents an ideal tool for supporting large-scale multi-protein biomarker evaluation studies to demonstrate biomarker clinical validity. With a growing list of potentially important new biomarkers being discovered and now evaluated by mass spectrometry, it is tempting to suggest that ultimately MRM maybe a useful tool for translating these candidates into clinical utility.
Clinical Application of Proteomics in Chronic Arthritides
Affinity proteomics as well as different mass spectrometry platforms have been used for screening of serum, plasma, or urine samples for distinct protein and metabolite signatures or autoantibody responses both in pediatric as well as adult rheumatology (Table 1). One prominent focus in investigating chronic arthritis in adults using affinity proteomics is on the understanding of cyto- and chemokine patterns that are specifically associated with clinical disease onset [26,28,28] or certain serological subtypes [26, 29, 30•]. Further, multiplexed assay platforms have been employed to study autoantibody specificities and epitope spreading [29, 31,33,33]. Finally, both autoantibody as well as cyto- and chemokine signatures have been assessed to better distinguish between diseases with similar clinical phenotypes [30, 34, 35]. Similarly, different mass spectrometry approaches have been used to identify disease specific signatures [36,38,39,40,40] or patterns associated with response to therapy [41, 42].
Affinity proteomic approaches in pediatric rheumatology appear targeted at characterizing cyto- and chemokine patterns to acquire better understanding of potential pathological pathways [43, 44, 45••] and predict disease-related complications [45••, 46]. To date, we could identify only two studies performing mass spectrometry to identify proteomic signatures in context with chronic arthritis in children [47, 48••].
Overall, proteomic studies published in context with chronic arthritis in children or adults reveal a pronounced imbalance between discovery and validation (Table 1); compared to reported discovery of new markers and signatures that are meant to predict [26,28,29,29, 30, 31,33,33, 41, 42, 45••, 46], follow-up [43••, 44, 45••, 47], or discriminate disease [30, 34,36,37,38,39,40,40]; there are very few studies that actually validate findings [36, 48,50,••–50].
This is particularly relevant as the complexity and amount of variables in affinity proteomic assays requires extensive validation. Assay result confounding variables are:
-
i)
Arthritis patients’ biological therapies can have profound, eventually unexpected effects on respective cytokine levels. In these lines, the IL-6 receptor antagonizing antibody tocilizumab has been shown to strongly increase circulating IL-6 levels [51], which requires very careful interpretation of previously set assay thresholds and clinical outcome prediction in tocilizumab-treated patients [48••].
-
ii)
The type of clinical sample, quality, and storage can all significantly influence study outcome [52].
-
iii)
Finally, as already mentioned above, the quality and sensitivity of detection ligands (antibodies, peptides, etc.) is an absolutely critical issue in affinity proteomics. For commercial multiplexed immune assays, it frequently remains unclear which specific capture and detection antibody pairs are in use. This can significantly impact assay reproducibility between different suppliers. While assays results for a given set of samples may still partly correlate [53], absolute measured values may differ dramatically which makes it extremely difficult to introduce universal cut-offs or critical thresholds for example to predict clinical disease onset. Sophisticated buffer recipes have been introduced to minimize matrix effects and undesired capture/detection ligand cross-reactivities within samples. Still, in diseases with high antibody titers such as rheumatoid arthritis (RA), multiplexed cytokine detection has been shown to be significantly confounded by rheumatoid factor (RF) or other heterophilic antibodies [49, 54].
Currently, in adult rheumatology, the Vectra DA disease activity test is the only multi-analyte platform that has been extensively evaluated in multiple studies for clinical use. From a set of 396 candidate biomarkers, a panel of 12 analytes (Table 1) was selected [27, 28]. Based on quantification of these markers by planar antibody array, a multi-biomarker disease activity (MBDA) score is calculated, which proved to correlate significantly with the 28-joint count disease activity score including erythrocyte sedimentation rate (DAS28-ESR) [55] or C-reactive protein (DAS28-CRP) [56] and served as independent predictor of disease activity [56] or radiographic progression in early RA patients [57]. MBDA improved the prediction of relapses in patients with RA in stable remission undergoing DMARD tapering. If combined with testing for anti-citrullinated protein antibodies (ACPAs), the MBDA score further allowed prediction of relapse in more than 80% of the patients [58]. Prediction of response to second-line therapy after methotrexate failure or to different TNFα-blocking drugs yielded less definite results [59••, 60].
For assessment of arthritis activity or prediction of disease progression in children, there are currently no comparable multi-parametric tools or validated biomarkers derived from unbiased proteomic approaches. However, independently of this and extensively reviewed elsewhere [61, 62], the phagocyte-specific S100 proteins S100A8/A9 and S100A12 proved as reliable markers of disease activity and for monitoring response to therapy in juvenile idiopathic arthritis (JIA) [63,65,66,67,67].
Meanwhile, local overexpression of these markers in inflamed joints has also been evaluated using mass spectrometry and suggested to distinguish RA from miscellaneous inflammatory arthritis [68]. Similarly, serum interleukin (IL) 18 has been shown distinguish sJIA from other febrile diseases [69] and to predicting the development of macrophage activation syndrome in systemic juvenile idiopathic arthritis [70]. Elevated IL-18 in systemic juvenile idiopathic arthritis (sJIA) compared to oligo- and polyarticular disease as well as S100A12 has also been identified as part of bead array immune assays [43••, 44] and is currently evaluated as part of a multi-marker panel for improved sJIA diagnosis (full paper in preparation [71]).
Finally, from all already referenced studies, one stood out in that it was dedicated to compare the use of two different affinity proteomics platforms (Luminex, SOMAscan) and mass spectrometry to identify candidate biomarkers that have the potential to distinguish between patients with psoriatic arthritis (PsA) or rheumatoid arthritis (RA) and explore the value of combining different protein discovery platforms for the development of a multiplexed protein biomarker panel. The study identified 324 proteins differentiating PsA and RA using label-free LC-MS, while Luminex targeted 48 proteins and SOMAscan supported the measurement of 1129 markers. By combining the data from these techniques, it was possible to reproducibly quantify a total of 1501 proteins. Importantly, while there was some overlap in the proteins measured by the three platforms, there was no overlap in the proteins that were shown to be differentially expressed proteins between PsA and RA by all three platforms. This demonstrates how challenging it may be to conclude from an unbiased broad screen performed with one technology to a targeted applicable assay in a finally user-friendly format for clinical application [72••].
Conclusion
In addition to the challenges, physicians are facing with the requirement to establish an early diagnosis of rheumatic diseases, there is an unmet need to stratify patients with chronic arthritis according to the nature of their disease with regard to disease extension and prognosis. It is a key task to identify patients who will develop complications such as the extension of the disease, which is a hallmark of patients who suffer from the progression of chronic inflammation. In addition, with rapidly improving therapeutic options, there is a strong need to monitor the effectiveness of treatment and, ideally, to find the right medication for the individual patient. Precision medicine and personalized or at least stratified therapeutic interventions are only achievable if molecular markers help identifying disease processes. Protein biomarkers have the potential to provide an objective measure of arthritic processes and the responses to a pharmacological intervention. They serve an objective molecular indicator or surrogate of pathological processes that possess diagnostic, prognostic, or predictive utility. Hence, they provide an added value to clinical markers that rely on physical variables or symptoms such as joint count, pain assessment, or radiological findings.
The development of new biomarkers for commercialization relies on robust data on the pathophysiological role of potential marker targets in the processes of chronic inflammation. In other words, it is meaningful to focus efforts of biomarker development on those factors that clearly have a molecular role in the initiation, progression, or modulation of the disease processes in arthritis. A number of potential biomarkers have been reported, but few, if any, have been adopted in routine practice. The Vectra DA test is an example of a multiplexed biomarker test that has made it into the clinical routine in the care of patients with RA [73, 74]. Especially in juvenile arthritis patients, single markers such as IL-18 or S100/DAMP-proteins proofed useful, e.g., for identifying patients with systemic arthritis or for monitoring subclinical disease activity. There is, however, no dispute that improved multi-parametric tools are urgently required for both objective diagnosis and optimal management.
Despite the advances in technologies, well-designed studies focusing on protein biomarkers for chronic arthritis are still key for the translation of improved knowledge into applicable tools. Recent advances summarized in this review are encouraging. However, with the exception of a few examples, the list of truly valuable tools in clinical routine is disappointingly small. Thus, there remains an unmet need for future scientific efforts, and the importance of protein biomarker research needs to be emphasized. With regard to the increased interest in treat-to-target therapeutic strategies, it is rather surprising that biomarker research is still underused. Future controlled trials and cohort studies should include strategic plans for proteomic analyses aiming at the discovery and validation of improved biomarkers that would allow precision medicine.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Wasinger VC, Cordwell SJ, Cerpa-Poljak A, Yan JX, Gooley AA, Wilkins MR, et al. Progress with gene-product mapping of the Mollicutes: Mycoplasma genitalium. Electrophoresis. 1995;16(7):1090–4.
Pennington SR, Wilkins MR, Hochstrasser DF, Dunn MJ. Proteome analysis: from protein characterization to biological function. Trends Cell Biol. 1997;7(4):168–73.
Aebersold R, Mann M. Mass-spectrometric exploration of proteome structure and function. Nature. 2016;537(7620):347–55.
Gibson DS, Rooney ME, Finnegan S, Qiu J, Thompson DC, Labaer J, et al. Biomarkers in rheumatology, now and in the future. Rheumatology (Oxford). 2012;51(3):423–33.
Poste G. Bring on the biomarkers. Nature. 2011;469(7329):156–7.
Poste G. Biospecimens, biomarkers, and burgeoning data: the imperative for more rigorous research standards. Trends Mol Med. 2012;18(12):717–22.
Horvath AR, Lord SJ, StJohn A, Sandberg S, Cobbaert CM, Lorenz S, et al. From biomarkers to medical tests: the changing landscape of test evaluation. Clin Chim Acta. 2014;427:49–57.
Horvath AR, Bossuyt PM, Sandberg S, John AS, Monaghan PJ, Verhagen-Kamerbeek WD, et al. Setting analytical performance specifications based on outcome studies—is it possible? Clin Chem Lab Med. 2015;53(6):841–8.
Sandberg S, Fraser CG, Horvath AR, Jansen R, Jones G, Oosterhuis W, et al. Defining analytical performance specifications: Consensus Statement from the 1st Strategic Conference of the European Federation of Clinical Chemistry and Laboratory Medicine. Clin Chem Lab Med. 2015;53(6):833–5.
Skates SJ, Gillette MA, LaBaer J, Carr SA, Anderson L, Liebler DC, et al. Statistical design for biospecimen cohort size in proteomics-based biomarker discovery and verification studies. J Proteome Res. 2013;12(12):5383–94.
Monaghan PJ, Lord SJ, St John A, Sandberg S, Cobbaert CM, Lennartz L, et al. Biomarker development targeting unmet clinical needs. Clin Chim Acta. 2016;460:211–9.
Lollo B, Steele F, Gold L. Beyond antibodies: new affinity reagents to unlock the proteome. Proteomics. 2014;14(6):638–44.
Langham S, Langham J, Goertz HP, Ratcliffe M. Large-scale, prospective, observational studies in patients with psoriasis and psoriatic arthritis: a systematic and critical review. BMC Med Res Methodol. 2011;11:32.
Song JW, Chung KC. Observational studies: cohort and case-control studies. Plast Reconstr Surg. 2010;126(6):2234–42.
Mc Ardle A, Flatley B, Pennington SR, FitzGerald O. Early biomarkers of joint damage in rheumatoid and psoriatic arthritis. Arthritis Res Ther. 2015;17:141.
Mamdani M, Sykora K, Li P, Normand SL, Streiner DL, Austin PC, et al. Reader’s guide to critical appraisal of cohort studies: 2. Assessing potential for confounding. BMJ. 2005;330(7497):960–2.
Rissin DM, Kan CW, Campbell TG, Howes SC, Fournier DR, Song L, et al. Single-molecule enzyme-linked immunosorbent assay detects serum proteins at subfemtomolar concentrations. Nat Biotechnol. 2010;28(6):595–9.
• Rodero MP, Decalf J, Bondet V, Hunt D, Rice GI, Werneke S, et al. Detection of interferon alpha protein reveals differential levels and cellular sources in disease. J Exp Med. 2017;214(5):1547–55. First published application of digital ELISA for quantification of interferon α.
Gold L, Ayers D, Bertino J, Bock C, Bock A, Brody EN, et al. Aptamer-based multiplexed proteomic technology for biomarker discovery. PLoS One. 2010;5(12):e15004.
Lundberg M, Thorsen SB, Assarsson E, Villablanca A, Tran B, Gee N, et al. Multiplexed homogeneous proximity ligation assays for high-throughput protein biomarker research in serological material. Mol Cell Proteomics. 2011;10(4):M110 004978.
Lundberg M, Eriksson A, Tran B, Assarsson E, Fredriksson S. Homogeneous antibody-based proximity extension assays provide sensitive and specific detection of low-abundant proteins in human blood. Nucleic Acids Res. 2011;39(15):e102.
Collins BC, Miller CA, Sposny A, Hewitt P, Wells M, Gallagher WM, et al. Development of a pharmaceutical hepatotoxicity biomarker panel using a discovery to targeted proteomics approach. Mol Cell Proteomics. 2012;11(8):394–410.
Adkins JN, Varnum SM, Auberry KJ, Moore RJ, Angell NH, Smith RD, et al. Toward a human blood serum proteome: analysis by multidimensional separation coupled with mass spectrometry. Mol Cell Proteomics. 2002;1(12):947–55.
Silva AM, Vitorino R, Domingues MR, Spickett CM, Domingues P. Post-translational modifications and mass spectrometry detection. Free Radic Biol Med. 2013;65:925-41.
Verheul MK, van Veelen PA, van Delft MAM, de Ru A, Janssen GMC, Rispens T, et al. Pitfalls in the detection of citrullination and carbamylation. Autoimmun Rev. 2018;17(2):136-41.
Kokkonen H, Soderstrom I, Rocklov J, Hallmans G, Lejon K, Rantapaa DS. Up-regulation of cytokines and chemokines predates the onset of rheumatoid arthritis. Arthritis Rheum. 2010;62(2):383–91.
Centola M, Cavet G, Shen Y, Ramanujan S, Knowlton N, Swan KA, et al. Development of a multi-biomarker disease activity test for rheumatoid arthritis. PLoS One. 2013;8(4):e60635.
Eastman PS, Manning WC, Qureshi F, Haney D, Cavet G, Alexander C, et al. Characterization of a multiplex, 12-biomarker test for rheumatoid arthritis. J Pharm Biomed Anal. 2012;70:415–24.
Sokolove J, Bromberg R, Deane KD, Lahey LJ, Derber LA, Chandra PE, et al. Autoantibody epitope spreading in the pre-clinical phase predicts progression to rheumatoid arthritis. PLoS One. 2012;7(5):e35296.
Chandra PE, Sokolove J, Hipp BG, Lindstrom TM, Elder JT, Reveille JD, et al. Novel multiplex technology for diagnostic characterization of rheumatoid arthritis. Arthritis research & therapy. 2011;13(3):R102.
Brink M, Hansson M, Mathsson L, Jakobsson PJ, Holmdahl R, Hallmans G, et al. Multiplex analyses of antibodies against citrullinated peptides in individuals prior to development of rheumatoid arthritis. Arthritis and rheumatism. 2013;65(4):899–910.
• Too CL, Murad S, Hansson M, Alm LM, Dhaliwal JS, Holmdahl R, et al. Differences in the spectrum of anti-citrullinated protein antibody fine specificities between Malaysian and Swedish patients with rheumatoid arthritis: implications for disease pathogenesis. Arthritis Rheumatol. 2017;69(1):58–69. Peptide array identifying disease-related antibody profiles.
Tong D, Lonnblom E, Yau ACY, Nandakumar KS, Liang B, Ge C, et al. A shared epitope of collagen type XI and type II is recognized by pathogenic antibodies in mice and humans with arthritis. Front Immunol. 2018;9:451.
Ramirez J, Inciarte-Mundo J, Cuervo A, Ruiz-Esquide V, Hernandez MV, Sanmarti R, et al. Differing local and systemic inflammatory burden in polyarticular psoriatic arthritis and rheumatoid arthritis patients on anti-TNF treatment in clinical remission. Clin Exp Rheumatol. 2017;35(1):74–9.
Chen J, Doyle TJ, Liu Y, Aggarwal R, Wang X, Shi Y, et al. Biomarkers of rheumatoid arthritis-associated interstitial lung disease. Arthritis Rheumatol. 2015;67(1):28–38.
Watanabe J, Charles-Schoeman C, Miao Y, Elashoff D, Lee YY, Katselis G, et al. Proteomic profiling following immunoaffinity capture of high-density lipoprotein: association of acute-phase proteins and complement factors with proinflammatory high-density lipoprotein in rheumatoid arthritis. Arthritis Rheum. 2012;64(6):1828–37.
Smolenska Z, Smolenski RT, Zdrojewski Z. Plasma concentrations of amino acid and nicotinamide metabolites in rheumatoid arthritis—potential biomarkers of disease activity and drug treatment. Biomarkers : biochemical indicators of exposure, response, and susceptibility to chemicals. 2016;21(3):218–24.
Ahmed U, Anwar A, Savage RS, Costa ML, Mackay N, Filer A, et al. Biomarkers of early stage osteoarthritis, rheumatoid arthritis and musculoskeletal health. Sci Rep. 2015;5:9259.
Zhang X, Yuan Z, Shen B, Zhu M, Liu C, Xu W. Discovery of serum protein biomarkers in rheumatoid arthritis using MALDI-TOF-MS combined with magnetic beads. Clin Exp Med. 2012;12(3):145–51.
Reindl J, Pesek J, Kruger T, Wendler S, Nemitz S, Muckova P, et al. Proteomic biomarkers for psoriasis and psoriasis arthritis. J Proteome. 2016;140:55–61.
Blaschke S, Rinke K, Maring M, Flad T, Patschan S, Jahn O, et al. Haptoglobin-alpha1, -alpha2, vitamin D-binding protein and apolipoprotein C-III as predictors of etanercept drug response in rheumatoid arthritis. Arthritis research & therapy. 2015;17:45.
Trocme C, Marotte H, Baillet A, Pallot-Prades B, Garin J, Grange L, et al. Apolipoprotein A-I and platelet factor 4 are biomarkers for infliximab response in rheumatoid arthritis. Ann Rheum Dis. 2009;68(8):1328–33.
de Jager W, Hoppenreijs EP, Wulffraat NM, Wedderburn LR, Kuis W, Prakken BJ. Blood and synovial fluid cytokine signatures in patients with juvenile idiopathic arthritis: a cross-sectional study. Ann Rheum Dis. 2007;66(5):589–98.
Kessel C, Lippitz K, Weinhage T, Hinze C, Wittkowski H, Holzinger D, et al. Proinflammatory cytokine environments can drive interleukin-17 overexpression by gamma/delta T cells in systemic juvenile idiopathic arthritis. Arthritis Rheumatol. 2017;69(7):1480–94.
•• Bracaglia C, de Graaf K, Pires Marafon D, Guilhot F, Ferlin W, Prencipe G, et al. Elevated circulating levels of interferon-gamma and interferon-gamma-induced chemokines characterise patients with macrophage activation syndrome complicating systemic juvenile idiopathic arthritis. Ann Rheum Dis. 2017;76(1):166–72. Important multiplexed biomarker profiling in pediatric rheumatology
Ling XB, Lau K, Deshpande C, Park JL, Milojevic D, Macaubas C, et al. Urine peptidomic and targeted plasma protein analyses in the diagnosis and monitoring of systemic juvenile idiopathic arthritis. Clin Proteomics. 2010;6(4):175–93.
Gibson DS, Blelock S, Curry J, Finnegan S, Healy A, Scaife C, et al. Comparative analysis of synovial fluid and plasma proteomes in juvenile arthritis—proteomic patterns of joint inflammation in early stage disease. J Proteome. 2009;72(4):656–76.
•• Reiss WG, Devenport JN, Low JM, Wu G, Sasso EH. Interpreting the multi-biomarker disease activity score in the context of tocilizumab treatment for patients with rheumatoid arthritis. Rheumatol Int. 2016;36(2):295–300. Treatment directly affecting MBDA scores.
Curtis JR, van der Helm-van Mil AH, Knevel R, Huizinga TW, Haney DJ, Shen Y, et al. Validation of a novel multibiomarker test to assess rheumatoid arthritis disease activity. Arthritis Care Res (Hoboken). 2012;64(12):1794–803.
Todd DJ, Knowlton N, Amato M, Frank MB, Schur PH, Izmailova ES, et al. Erroneous augmentation of multiplex assay measurements in patients with rheumatoid arthritis due to heterophilic binding by serum rheumatoid factor. Arthritis Rheum. 2011;63(4):894–903.
Nishimoto N, Terao K, Mima T, Nakahara H, Takagi N, Kakehi T. Mechanisms and pathologic significances in increase in serum interleukin-6 (IL-6) and soluble IL-6 receptor after administration of an anti-IL-6 receptor antibody, tocilizumab, in patients with rheumatoid arthritis and Castleman disease. Blood. 2008;112(10):3959–64.
de Jager W, Bourcier K, Rijkers GT, Prakken BJ, Seyfert-Margolis V. Prerequisites for cytokine measurements in clinical trials with multiplex immunoassays. BMC Immunol. 2009;10:52.
Elshal MF, McCoy JP. Multiplex bead array assays: performance evaluation and comparison of sensitivity to ELISA. Methods. 2006;38(4):317–23.
de Jager W, Prakken BJ, Bijlsma JW, Kuis W, Rijkers GT. Improved multiplex immunoassay performance in human plasma and synovial fluid following removal of interfering heterophilic antibodies. J Immunol Methods 2005;300(1–2):124–135.
Hirata S, Dirven L, Shen Y, Centola M, Cavet G, Lems WF, et al. A multi-biomarker score measures rheumatoid arthritis disease activity in the BeSt study. Rheumatology (Oxford). 2013;52(7):1202–7.
Bakker MF, Cavet G, Jacobs JW, Bijlsma JW, Haney DJ, Shen Y, et al. Performance of a multi-biomarker score measuring rheumatoid arthritis disease activity in the CAMERA tight control study. Ann Rheum Dis. 2012;71(10):1692–7.
Hambardzumyan K, Bolce R, Saevarsdottir S, Cruickshank SE, Sasso EH, Chernoff D, et al. Pretreatment multi-biomarker disease activity score and radiographic progression in early RA: results from the SWEFOT trial. Ann Rheum Dis. 2015;74(6):1102–9.
Rech J, Hueber AJ, Finzel S, Englbrecht M, Haschka J, Manger B, et al. Prediction of disease relapses by multibiomarker disease activity and autoantibody status in patients with rheumatoid arthritis on tapering DMARD treatment. Ann Rheum Dis. 2016;75(9):1637–44.
•• Hambardzumyan K, Saevarsdottir S, Forslind K, Petersson IF, Wallman JK, Ernestam S, et al. A multi-biomarker disease activity score and the choice of second-line therapy in early rheumatoid arthritis after methotrexate failure. Arthritis Rheumatol. 2017;69(5):953–63. Use of MBDA for therapeutic decision-making in RA.
Fleischmann R, Connolly SE, Maldonado MA, Schiff M. Brief report: estimating disease activity using multi-biomarker disease activity scores in rheumatoid arthritis patients treated with abatacept or adalimumab. Arthritis Rheumatol. 2016;68(9):2083–9.
Kessel C, Holzinger D, Foell D. Phagocyte-derived S100 proteins in autoinflammation: putative role in pathogenesis and usefulness as biomarkers. Clin Immunol. 2013;147(3):229–41.
Holzinger D, Kessel C, Omenetti A, Gattorno M. From bench to bedside and back again: translational research in autoinflammation. Nat Rev Rheumatol. 2015;11(10):573–85.
Foell D, Wulffraat N, Wedderburn LR, Wittkowski H, Frosch M, Gerss J, et al. Methotrexate withdrawal at 6 vs 12 months in juvenile idiopathic arthritis in remission: a randomized clinical trial. JAMA. 2010;303(13):1266–73.
Frosch M, Strey A, Vogl T, Wulffraat NM, Kuis W, Sunderkotter C, et al. Myeloid-related proteins 8 and 14 are specifically secreted during interaction of phagocytes and activated endothelium and are useful markers for monitoring disease activity in pauciarticular-onset juvenile rheumatoid arthritis. Arthritis Rheum. 2000;43(3):628–37.
Wittkowski H, Frosch M, Wulffraat N, Goldbach-Mansky R, Kallinich T, Kuemmerle-Deschner J, et al. S100A12 is a novel molecular marker differentiating systemic-onset juvenile idiopathic arthritis from other causes of fever of unknown origin. Arthritis Rheum. 2008;58(12):3924–31.
Gerss J, Roth J, Holzinger D, Ruperto N, Wittkowski H, Frosch M, Wulffraat N, Wedderburn L, Stanevicha V, Mihaylova D, Harjacek M, Len C, Toppino C, Masi M, Minden K, Saurenmann T, Uziel Y, Vesely R, Apaz MT, Kuester RM, Elorduy MJR, Burgos-Vargas R, Ioseliani M, Magni-Manzoni S, Unsal E, Anton J, Balogh Z, Hagelberg S, Mazur-Zielinska H, Tauber T, Martini A, Foell D, for the Paediatric Rheumatology International Trials Organization (PRINTO) Phagocyte-specific S100 proteins and high-sensitivity C reactive protein as biomarkers for a risk-adapted treatment to maintain remission in juvenile idiopathic arthritis: a comparative study. Ann Rheum Dis 2012;71(12):1991–1997.
Holzinger D, Frosch M, Kastrup A, Prince FH, Otten MH, Van Suijlekom-Smit LW, et al. The Toll-like receptor 4 agonist MRP8/14 protein complex is a sensitive indicator for disease activity and predicts relapses in systemic-onset juvenile idiopathic arthritis. Ann Rheum Dis. 2012;71(6):974–80.
Baillet A, Trocme C, Berthier S, Arlotto M, Grange L, Chenau J, et al. Synovial fluid proteomic fingerprint: S100A8, S100A9 and S100A12 proteins discriminate rheumatoid arthritis from other inflammatory joint diseases. Rheumatology (Oxford). 2010;49(4):671–82.
Xia Y, Cui P, Li Q, Liang F, Li C, Yang J. Extremely elevated IL-18 levels may help distinguish systemic-onset juvenile idiopathic arthritis from other febrile diseases. Braz J Med Biol Res. 2017;50(2):e5958.
Shimizu M, Nakagishi Y, Inoue N, Mizuta M, Ko G, Saikawa Y, et al. Interleukin-18 for predicting the development of macrophage activation syndrome in systemic juvenile idiopathic arthritis. Clin Immunol. 2015;160(2):277–81.
Holzinger D, Kessel C, Fall N, Grom A, de jager W, Vastert S et al. S100A12 as diagnostic tool in the differential diagnosis of SJIA associated MAS vs. primary or acquired HLH. Pediatric Rheumatology 2016(Supplement 1):P297.
•• McArdle A, Qasim Butt A, Szentpetery A, de Jager W, de Roock S, FitzGerald O, et al. Developing clinically relevant biomarkers in inflammatory arthritis: a multiplatform approach for serum candidate protein discovery. Proteomics Clin Appl. 2016;10(6):691–8.
Hirata S, Li W, Defranoux N, Cavet G, Bolce R, Yamaoka K, et al. A multi-biomarker disease activity score tracks clinical response consistently in patients with rheumatoid arthritis treated with different anti-tumor necrosis factor therapies: a retrospective observational study. Mod Rheumatol. 2015;25(3):344–9.
Lee YC, Hackett J, Frits M, Iannaccone CK, Shadick NA, Weinblatt ME, et al. Multibiomarker disease activity score and C-reactive protein in a cross-sectional observational study of patients with rheumatoid arthritis with and without concomitant fibromyalgia. Rheumatology (Oxford). 2016;55(4):640–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
DF declares the receipt of research grant support and honoraria from Pfizer, Novartis, Sobi, and Chugai-Roche. The UCD Conway Institute and Proteomics Core is funded by the Programme for Research in Third level Institutions, as administered by Higher Education Authority of Ireland. Research in SRP’s lab is supported by grants from the Health Research Board, Enterprise Ireland and Science Foundation Ireland and previously including the EU funded FP7 MIAMI project. Dr. Pennington reports role as Founder and CSO of Atturos (www.atturos.com) which is developing prostate cancer multiplexed protein biomarker test on MRM platform. Drs. Kessel and Foell have a patent “means and methods for diagnosing and treating inflammatory disorders” (WO 2016/178154 A1) issued to Muenster University. Dr. Foell has a patent “means and methods for diagnosing and treating inflammatory disorders” (WO 2016/178154 A1) issued to Muenster University. Angela McArdle, Emely Verweyen, Toni Weinhage, and Helmut Wittkowski declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Pediatric Rheumatology
Rights and permissions
About this article

Cite this article
Kessel, C., McArdle, A., Verweyen, E. et al. Proteomics in Chronic Arthritis—Will We Finally Have Useful Biomarkers?. Curr Rheumatol Rep 20, 53 (2018). https://doi.org/10.1007/s11926-018-0762-0
Published:
DOI: https://doi.org/10.1007/s11926-018-0762-0