
Abstract
There exists a continuous spectrum of overeating, where at the extremes there are casual overindulgences and at the other a ‘pathological’ drive to consume palatable foods. It has been proposed that pathological eating behaviors may be the result of addictive appetitive behavior and loss of ability to regulate the consumption of highly processed foods containing refined carbohydrates, fats, salt, and caffeine. In this review, we highlight the genetic similarities underlying substance addiction phenotypes and overeating compulsions seen in individuals with binge eating disorder. We relate these similarities to findings from neuroimaging studies on reward processing and clinical diagnostic criteria based on addiction phenotypes. The abundance of similarities between compulsive overeating and substance addictions puts forth a case for a ‘food addiction’ phenotype as a valid, diagnosable disorder.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Chronic overweight and obesity in children and adults have become a worldwide epidemic due to the increasing availability of food, and consequently, its overconsumption [1, 2]. Overweight individuals face a multitude of medical risks including hypertension [3], type 2 diabetes [4], respiratory conditions (e.g., sleep apnea) [5], metabolic syndromes, and cardiovascular diseases [6].
Proper nutrition, as well as, psychical activity, is the key to maintaining a healthy weight [7]. Many overweight individuals struggle with patterns of overeating, which exist on a continuum of severity from casual overindulgence to a compulsive drive to consume certain foods [8••]. Such pathological bouts of excessive and uncontrollable overeating characterize binge eating disorder (BED) [8••]. For BED, behavioral and pharmacological treatments for eating, such as increasing the amount of physical activity (e.g., walking, yoga) [9] and medications (e.g., antidepressants, topiramate, and sibutramine hydrochloride) [10], have provided variable results. Therefore, novel approaches to understanding how eating behaviors impact weight gain are necessary to help individuals reclaim a healthy weight.
It has been proposed that some pathological overeating behaviors may be the result of addictive tendencies toward highly processed foods containing refined carbohydrates, fats, salt, and caffeine [11••, 12]. It is possible, therefore, that the recognition of some cases of compulsive overeating as a ‘food addiction’ similar to substance use disorders (SUDs), as described in the Diagnostic and Statistical Manual of Mental Disorders-5 (DSM-5), could create more awareness and new treatment options based on currently successful treatment techniques for SUD [13].
Several similarities between compulsive overeating and substance addiction have been noted, including the abilities of processed foods and addictive substances to activate the brain’s reward system [14, 15]. The neural reward system is likely to have evolved to augment more reflexive survival mechanisms. In this way, the integration of reward valuation (i.e., estimation the worth of a reward) would have then allowed a complex nervous system to develop. Furthermore, reward valuation would have demotivated erroneous behaviors and encouraged beneficial behaviors through negative rewards (i.e., removal of an averse stimulus) and positive rewards (i.e., appearance of a positive stimulus), respectively [3, 4]. The co-evolution of associative learning between actions and motivational, anticipatory elements known as ‘cues’ are the integral aspect of the reward system which facilitates key behavioral learning processes. Associative learning would have been beneficial to allow the discovery of useful and pleasurable substances which promoted survival and reproduction [16]. Possessing genetic variations allowing individuals to indulge in highly caloric foods would have been greatly beneficial during times of food scarcity to prevent starvation [17]. Currently, however, food is omnipresent and richer in fats and sugars, which contribute to overeating that may lead to obesity [18, 19].
It is clear that food, in general, is not addictive; rather, the particular composition of certain foods appears to be driving the pleasure response. The composition of food has changed drastically over time, such that it has come to contain high concentrations of refined sugars, fats, salt, and even caffeine, particularly present in processed and fast foods [2]. In general, there is a global trend toward increased consumption of calorie-dense foods high in fats, salts, and sugars and a decrease in the consumption legumes, vegetables, and grains [6]. This increase in refined foods shows a positive correlation with the increased incidence of obesity and related health issues, such as diabetes and hypertension [2, 6]. As the global nutrition dynamic is changing, the case for a ‘food addiction’ has become more pertinent as there are increasing opportunities for certain individuals to become ‘addicted’.
The consumption of psychoactive substances such as caffeine, nicotine, alcohol, cocaine, and cannabis is widespread among modern societies [5]. However, not every individual who partakes in substances of abuse becomes addicted, and not every individual develops pathological eating patterns [7]. Thus, it has been suggested that individuals who become addicted, or tend to compulsively overeat, possess some underlying genetic or acquired vulnerability related to brain reward pathways, possibly paired with diminished impulse control [8••]. In this review, we present the neurobiology of the reward system, its role in the control of food intake, and how variation in the sensitivity of this neural circuitry influences the risk for addictive behaviors. We also highlight the ongoing debate on the concept related to ‘food addiction’.
The Neurocognitive Substrates of Reward
The association between food consumption and pleasure is facilitated by the reward system which posits a value on the obtained reward. The anticipated valence of the reward—either positive or negative—correlates with the degree of motivation that is generated, including the amount of reward-seeking behaviors [20, 21]. The reward system is a complex interrelationship between components of the central nervous system and neurotransmitters which facilitate communication. The release of dopamine (DA) within the mesolimbic DA pathway, including the ventral tegmental area (VTA), the nucleus accumbens (NAc), and several limbic regions, such as the hypothalamus, amygdala, hippocampus, and cingulate gyrus, induces motivational processes such as the anticipation of a pleasurable feeling [14, 22, 23••]. Discrepancies between the expected reward and the actual sensation during reward delivery, called reward prediction errors, permit the long-term learning of the reward value of different stimuli present in the environment [24].
The Incentive Sensitization Theory: ‘Liking’ Versus ‘Wanting’
The incentive sensitization theory couples Pavlovian classical conditioning principles with associative learning [25]. Addictive substances produce neuroadaptations which sensitize the reward system to substance-associated stimuli. Substance administration results in DA release within the nucleus accumbens (NAc) and the ventral tegmental area VTA, producing the rewarding effects of the substance. DA induces motivational processes such as the anticipation of pleasurable feelings. Through the modulation and timing of DA release, the reward center controls motivational behaviors and enables long-term encoding of ‘cues’ which are associated with various peripheral stimuli present during substance use. In the presence of cues, DA is released, resulting in motivation mechanisms which encourage substance-seeking behavior (wanting) and subsequent substance use [25]. There appears to be dissociation between ‘wanting’, a learned approach–response regulated by DA, and ‘liking, a hedonic sensation regulated by the endogenous opioid system [26]. Nonetheless, it has been suggested that the combination of both processes is necessary to experience the full scope of the reward [27].
Addiction has been characterized by altered motivational behavior, deficits in self-inhibition, and by poor decision making. Altered dopaminergic signaling in the mesolimbic system may help differentiate individuals who are addicted to substances (including food) and those who are not. Functional hypo-activity of dopaminergic neurons may lead to the consumption of rewarding substances to compensate for DA deficiency [28]. Studies have shown that addicted individuals present with a high responsiveness to reward and are more easily pleased by rewarding stimuli in their environment [29, 30]. Similarly, overweight and obese individuals are more responsive to food cues and show greater anticipation to food reward than those of normal weight [31••, 32].
Desensitization, Tolerance, and Withdrawal
Another component of the addiction paradigm is the tolerance that sets in as the result of continuous substance intake which allows for the maintenance of addictive behaviors over time. The overconsumption of reward can cause the down-regulation of DA receptors, resulting in a diminished reward response (i.e., DA receptor activation); therefore, the threshold at which the substance can elicit a sufficiently rewarding experience tends to increase overtime. To counter this ‘desensitization’, individuals may increase their substance intake to elicit a comparative reward experience, thereby increasing their reward gradually overtime [33]. Eventually, the ‘wanting’ of the reward is maintained while the ‘liking’ of the reward may diminish [15].
The initial hypersensitivity to reward, displayed by individuals with addictive phenotypes, diminishes with prolonged exposure to the reward [28]. This tolerance is the result of neuronal adaptation to the presence of the substance and its induction of DA release. One of these adaptations includes the reduction of DA D2 receptors (DRD2s) in response to a constant release in DA, decreasing the system’s sensitivity to reward [34]. After prolonged substance use, the subjective pleasure experienced from substance use decreases, and substance use becomes compulsory simply to maintain an individual’s equilibrium at baseline [35–37]. It has been suggested that in obese people, DRD2 down-regulation can lead to a mismatch between the expected and the actual rewarding effect of food, for which individuals try to compensate by consuming more. Thus, overeating and substance-addiction mechanisms appear to share clinical and neurobiological similarities. However, it is important to note that obesity is not always the result of addictive tendencies toward palatable food, and that this condition may also be seen in people of normal weight who may engage in compensatory behaviors to offset the ingestion of excessive calories [38].
Neural Reward Circuitry and Food Intake Regulation
The regulation of food intake requires not only the homeostatic and satiety systems but also their interaction and coordination with the system involved in reward processing. The key region of the mesolimbic DA pathway is the VTA which projects its dopaminergic neurons to target regions, specifically the NAc of the ventral striatum. Relevant reward stimuli activate VTA/DA neurons, which induce DA release in the NAc [39, 40].
Released DA binds to specific DA receptors which exist as subtypes D1 to D5 [41]. Binding of DA to D1 and D5 receptors induces activation of the heterotrimeric G protein, which in turn activates the enzyme adenylyl cyclase (AC). AC permits the synthesis of the second messenger cAMP, which activates protein kinase A (PKA). PKA regulates the stimulation of downstream molecules such as DA- and cAMP-regulated neuronal phosphoprotein as well as the transcription response. Subsequently, these molecules permit the regulation of gene expression and additional cellular responses. Furthermore, DA binding to D2, D3, and D4 receptors activates heterotrimeric G proteins which inhibit AC, resulting in the decrease of cAMP synthesis. Consequently, depletion of cAMP results in decreased PKA activation and decreased gene expression. Finally, DA is cleared from the synapse through DA transporter (DAT) reuptake into pre-synaptic neurons [42, 43]. This system allows response reinforcement to both primary rewards such as food and to secondary rewards such as money [44]. Dysfunction in a single component of the DA reward system may result in an impaired reward response [34].
Neuropeptides implicated in energy homeostasis can interact with VTA DA neurons that project to the NAc, prefrontal and limbic regions to signal reward [45]. The secretion of neuropeptides is regulated by the hypothalamus [45]. While short-term regulation refers to the control of food intake during a meal to allow portion control, long-term regulation refers to the control of intake over long periods of time to maintain homeostasis and body weight [46]. These two types of regulation are facilitated by neuropeptides such as leptin, insulin, ghrelin, amylin, cholecystokinin (CCK), and neuropeptide Y (NPY), which interact in the hypothalamus [46].
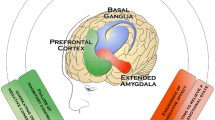
Some neuropeptides such as leptin, secreted from adipose tissue, and amylin, secreted from the pancreas, have been termed adiposity signals as their secretion is directly proportional to the amount of body fat, and they inhibit food intake and promote energy expenditure [47–49]. On the other hand, ghrelin, orexin, and NPY stimulate food intake such that ghrelin secretion is inversely proportional to stored body fat and orexin and NPY are directly proportional. Other neuropeptides secreted from the gut during a meal, such as CCK, provide satiety signals to the brain [50, 51]. These neuropeptides act on two different populations of neurons in the arcuate nucleus, POMC/CART and NPY/AgrP neurons. POMC/CART neurons play a role in stimulating food consumption and thus constitute a catabolic pathway. Conversely, NPY/AgrP neurons inhibit food consumption and thus constitute an anabolic pathway [52, 53]. See Fig. 1 for further details.

The satiety signaling pathway. Note. The paraventricular nucleus (PVN) has been suggested to contain neurons that synthesize catabolic neuropeptides, including corticotropin-releasing hormone (CRH), thyrotropin-releasing hormone (TRH), and oxytocin, whereas the lateral hypothalamic area (LHA) appears to contain neurons that synthesize anabolic neuropeptides such as orexin and melanin-concentrating hormone (MCH). PVN neurons have been shown to be stimulated by POMC/CART neurons and inhibited by NPY/AgrP neurons whereas LHA neurons are stimulated by NPY/AgrP neurons and inhibited by POMC/CART neurons. POMC/CART neurons secrete the neuropeptide a-MSH that binds to the melanocortin receptor 4 (MC4) and activates PVN and LHA neurons. NPY/ AgrP neurons secrete AgrP protein, which is an antagonist of a-MSH and thus blocks the activation of MC4 by a-MSH. NPY/AgrP neurons can also inhibit POMC/CART neurons through the neurotransmitter GABA. Leptin secreted from the adipocytes and insulin secreted from the pancreas inhibit the NPY/AgrP anabolic pathway and stimulate the POMC/CART catabolic pathway. Ghrelin secreted from the stomach stimulates the NPY/AgrP anabolic pathway and inhibits the POMC/CART catabolic pathway. These homeostatic signals and satiety signals such as CCK from the stomach converge in the NTS
Neuropeptides implicated in energy homeostasis can also modulate DA. Studies have shown that leptin can modulate mesolimbic sensitivity to food cues in order to reduce the attractiveness of food while providing satiety signals to the brain [54]. Specifically, leptin binds to its receptor (LepR), thus decreasing NAc activity and inducing a diminished release of DA, which in turn dampens motivation for food-seeking behaviors and consumption [54]. The majority of LepRs are present in neurons of the lateral hypothalamus and express the neuropeptide neurotensin (NT) implicated in reward processes [55]. Leptin depolarizes LepR- and NT-expressing lateral hypothalamic neurons, which ultimately decreases the reward response to food [55]. Insulin similarly attenuates limbic-region response to food stimuli [56]. On the other hand, ghrelin is an orexigenic hormone which increases the firing of DA neurons, and thus, the level of DA in the NAc, thereby stimulating food intake [57, 58]. Different neuropeptides implicated in the regulation of homeostasis and in the functioning of the reward system act together to promote food intake during deprivation and inhibit food intake during satiety. Disruption in one of these regulatory systems may lead to overeating and obesity [59].
Genetic Variation and Addictive Phenotypes
Food consumption is essential for survival; therefore, the reward system has evolved to value and reward the consumption of caloric foods by inducing pleasure [16]. During times of food scarcity, our hominin ancestors would have greatly benefited from a pleasurable response to foods rich in fats and sugars, ensuring their survival and reproductive success. However, in our current environment where highly caloric foods are readily and constantly available, this innate reward system response can result in problematic food overconsumption [16]. The similarities in the neurobiology of substance and food addictions suggest that there are common underlying genetic mechanisms regulating the reward circuitry through the mesolimbic DA pathway [60] and genetic variation of neurotransmitter pathways might also be relevant for treatment interventions in addictions [61].
Dopaminergic System Genes
The importance of dopaminergic signaling in reward mechanisms is clearly highlighted in addiction and obesity research [62, 63]. The DA D2 receptor (DRD2) and DA transporter (DAT) are two central players in the regulation of dopaminergic transmission. While D2 receptors act pre- and post- synaptically to bind DA, DATs are central to the removal of DA from the synaptic cleft and directly regulate post-synaptic dopaminergic signaling. Variants in genes encoding DA D2 receptor (DRD2) and transporter (DAT1, SLC6A3) have been commonly implicated in addictive phenotypes, including compulsive overeating [60].
The DA D2 receptor (DRD2) is centrally involved in the pathway regulating reward processing and motivation. The Taq1 (rs1800497) allele of the ANKK1 gene encoding D2 receptors is the most frequently investigated functional polymorphism and has been associated with reduced dopaminergic signaling [64] and hypo-activation during reward processing [65]. In substance-dependent individuals, carriers of the Taq1 A1 allele show reduced dopaminergic tone, and thereby, may have less efficient dopaminergic signaling. Such a condition may put them at risk for substance use, which may be a compensatory mechanism to increase neural DA levels [66]. Decreased striatal D2 density has been correlated with BMI, with one study reporting that the Taq1 A1 allele accounting for 45.9 % of variation in BMI [67]. Obese individuals and BED patients with the Taq1 A1 allele show greater sensitivity to reward than individuals of normal weight [68], choose food rewards more often in choice tasks, and consume more calories when rewarded with food [69]. Interestingly, DRD2 antagonists which block the reuptake of DA, namely antipsychotic medications, have repeatedly been shown to produce extreme antipsychotic-induced weight gain (AIWG) in individuals treated for schizophrenia, bipolar disorder, and other mental illnesses [70]. Pharmacogenetic studies have shown the association between Taq1 and increased risk for AIWG [71], further supporting the role of DRD2/ANKK1 gene polymorphisms in modulating weight and adiposity.
The DA transporter (DAT) gene (SLC6A3, DAT1) contains a 40 base pair, variable number tandem repeat (VNTR) polymorphism within its untranslated 3′ region. The DAT1 VNTR can contain between 3 and 13 repeats, with 9 to 10 repeats being the most common. Although the function of the DAT1 VNTR is not known, studies have shown that different alleles may result in variation of mesolimbic levels of DAT [72–74]. Carriers of the 9-allele have been shown to have greater striatal availability of DAT, suggesting increased synaptic DA and greater experience of reward [73].
The effects of DAT1 on addiction phenotypes have been well reviewed [73]. However, there is mixed evidence for associations of the DAT1 VNTR polymorphism and weight-related phenotypes. BMI and DAT availability within the striatum has shown a significant interaction, suggesting that variation in the DAT1 VNTR polymorphism may affect neural availability of DAT and sensitivity to food reward [75]. In a study of patients with BED and controls receiving either methylphenidate or placebo, BED patients with the 9/9 or 9/10 genotypes were more likely to show suppression in appetite [76]. Therefore, variations in the DAT1 gene may influence the amount of DA availability and the experience of reward in both SUDs and compulsive overeating.
Opioid Receptors
According to the incentive sensitization theory of addiction, endogenous opioids mediate the hedonic, ‘liking’ sensation that individuals feel when ingesting a pleasurable substance [26]. The involvement of opioids in the hedonic, motivational, and learning aspects of eating palatable foods and of substance use has been well reviewed [77, 78]. Endogenous opioids bind to the opioid receptors, most importantly the μ-opioid receptor encoded by the OPRM1 gene.
Variant A118G (rs1799971) of OPRM1 is the most commonly explored variant in the literature [79]. Individuals with the G/G genotype have been shown to have significantly higher preferences for sweet and fatty foods, which correlated with measures of overeating and BMI [80]. The G/G genotype has also been associated with greater alcohol-related fMRI cue-reactivity in alcohol-dependent individuals and correlated with craving and positive expectation of a hedonic experience [81]. Other variants of OPRM1 have also been explored in compulsive eating and addiction phenotypes, but require further investigation [82, 83].
It has been suggested that the interaction between OPRM1 and the dopaminergic plays a role in combining hedonic experience with motivational drive. Interestingly, a marginally significant interaction (p = 0.06) has been observed between DRD2 Taq1 and OPRM1 A118G in clinically obese individuals, suggesting a role for joint motivational and hedonic aspects in weight gain [84]. In other studies, however, no effect has been shown [85]. Preclinical models of addiction have provided similar evidence of an association of OPRM1 A118G with addicted phenotypes. For instance, mice with G/G genotypes show significantly greater preference for heroin and greater striatal levels of DA post self-administration of heroin, supporting the potential interaction between OPRM1 and the dopaminergic system [86].
Leptin Receptor (LEPR) and the Motivation to Consume
Genes encoding neuropeptides which regulate food intake and satiety may also be involved in modulating dopaminergic signaling. Polymorphisms of the leptin receptor (LEPR) gene have been shown to influence the receptor binding of leptin in the hypothalamus [63]. However, interaction between the leptin system and dopaminergic signaling in addictions and compulsive overeating still requires further investigation.
Genetic variations in LEPR may affect receptor functioning and the amount of central leptin available. Nogueiras and Seeley hypothesize that a potential interaction between leptin and the dopaminergic system may occur through the creation of a heterodimer between D2R and LepR, which may affect DRD2 signal transduction [87]. Similar affects are seen between the ghrelin receptor and DRD2 [87, 88]. In a preclinical model, LepR-knockdown in the lateral hypothalamus results in mice who show increased body weight due to increased consumption of food. Interestingly, in selective midbrain LepR-knockdown mice, there is decreased mesolimbic DA tone, suggesting decreased motivation for food reward [89]. In nicotine-dependent individuals, peripheral leptin levels have been associated with increased craving, depressed mood, decreased euphoria and withdrawal [90], further suggesting a role in motivating consumption [91, 92].
There are three LepR genetic polymorphisms associated with being overweight, including Lys109Arg (rs1137100), Gln223Arg (rs1137101), and Lys656Asn (rs8179187) [64]. The Lys109Arg variant has been particularly related to elevated body fat mass [60]. In one investigation of a large prospective, Dutch cohort (N = 17,500), individuals who gained weight over 6.8 years were more likely to be carriers of the Arg109 and Arg223 alleles, as well as, to have higher leptin levels, suggesting decreased LepR functionality [93]. Although these variants have not been investigated in addiction models, they show promise for future research in this area.
Melanocortin 4 Receptor (MC4R) and Reward Mechanisms
Melanocortins are a group of neuropeptides, including adrenocorticotropic hormone (ACTH), which is cleaved from proopiomelanocortin (POMC) within the pituitary gland [94]. Melanocortins can bind to one of five melanocortin receptors (MC1R to MC5R). Most importantly, MC4R is a key player in the regulation of food intake, such that approximately 5 % of individuals with MC4R gene mutations show dominantly-inherited obesity [95].
The melanocortin system also appears to play a role in the reward mechanism, both for substance and for food rewards. One investigation showed that the rewarding experience of cocaine administration may be mediated by the MC4R. In addition, MC4R mutant mice showed increased expression of MC4R in the NAc and striatum after repeated administration of cocaine, resulting in a sensitization response. In MC4R-null mice, the locomotor response to cocaine was completely prevented [96]. In a rat study, after 7 days of ethanol self-administration, the amount of self-administration increased (a response pattern reflecting tolerance). In cases where rats were given MC4R agonists, the amount of self-administration increased 89 % and was decreased if given MC4R antagonists [97]. MC4R variation may also be associated with decreased DA activity, such that MC4R knockout mice show increased appetite and weight gain.
There are several MC4R variants which have been shown to be associated with increased risk for being overweight and obesity-related phenotypes. In a GWAS of a large cohort of adults (>30,000), MC4R variant rs12970134 was shown to be associated with BMI, weight, and obesity [98]. In a later meta-analysis of 19 studies including 34,195 cases and 89,178 controls, a significant association of rs17782313 with increased risk for obesity in children and adults was confirmed (OR = 1.18, 95 % C.I. = 1.15–1.21, p < 0.001) [99]. More recently, Yilmaz et al. showed that the association between BMI and MC4R rs17782313 was mediated by emotional eating and food cravings [100]. Although more investigation is needed, mediation of the MC4R rs17782313–BMI relationship by emotional eating and cravings suggests a role for disinhibition and impulsivity in weight gain.
Recent evidence suggests a link between MC4R, obesity, and addiction. Porfirio et al. hypothesize that MC4R variation may be correlated with ADHD and increased eating behaviors. MC4R variation may lead to decreased dopaminergic activity which is in accord with the ‘reward deficiency’ theory of ADHD [101]. The connection of MC4R to reward, dopaminergic activity and overweight, further strengthens the support for ‘food addictions’ and ‘substance addictions’ sharing similar mechanisms.
Beneficial Genetic Variants
The genetic effects described above may have been useful throughout evolution to promote a low threshold of adiposity and to encourage the consumption of a large amount of highly caloric food whenever it was available, in order to facilitate energy storage for future needs [102]. Similarly, they may also be beneficial in the motivation to obtain other natural substances for medicinal purposes. However, in our society, where food and addictive substances are widely available, and made highly potent by technological advances, these genetic predispositions might be problematic [14].
Diagnostic Criteria for Addictive Disorders: Is There a Role for ‘Food Addiction’?
Currently, pathological gambling is the only non-substance related, addictive disorder that is diagnosable by the fifth edition of the Diagnostic and Statistical Manual of Mental Disorder (DSM-5) [103]. However, the recognition of BED as part of the collective feeding and eating disorders, including anorexia and bulimia nervosa, may eventually lead to the recognition of ‘food addiction’. Although the existence of a ‘food addiction’ has been a matter of some debate, its parallel symptomatology to SUDs, suggests that some forms of food overconsumption may be similar to addictive disorders.
Both SUDs and binge-eating pathology are characterized by reward system sensitivity which may be mediated by particular gene polymorphisms and overlapping neuroanatomical regions that show similar patterns of activation associated with processing reward [14, 23••]. These genetic and neuroanatomical similarities may lead to similar symptomology which can be argued to support the inclusion of BED as an addiction disorder. Proposed diagnostic criteria for ‘food addiction’ are based on symptoms specified in DSM-IV-TR for substance use disorders [12, 104]. Earlier attempts at exploratory diagnoses of addiction in individuals with BED provided clinical diagnostic evidence that these individuals meet addiction criteria on several dimensions. In a sample of 79 females diagnosed with BED, Cassin et al. showed that 92.4 % of participants ate more than they intended, 49.9 % experienced tolerance, 67.1 % experienced withdrawal, and 91.1 % continued to binge eat despite knowing the adverse effects [104]. Overall, 92.4 % of participants met full criteria for SUDs on two separate rating scales when the word ‘food’ was the ‘addictive’ substance used in the wording of the items [104].
The Yale Food Addiction Scale (YFAS)
Based on the genetic and neuroanatomical similarities between SUDs and compulsive overeating seen in patients with BED, the Yale Food Addiction Scale (YFAS) was developed to measure eating pathology according to DSM-IV criteria for SUDs [105••]. The YFAS aimed to assess individuals with binge-eating behaviors on several primary diagnostic criteria for SUDs (e.g., loss of control; see Table 1) [105••, 106]. Since the first validation of the YFAS [105••], the prevalence of a ‘food addiction’ has been shown to be similar in adult samples worldwide, including in Canada (8.7 %), Germany (8.8 %), USA (11.4 %) [107], and China (9.2 %) [108]. Interestingly, Eichen et al. reported that out of 178 individuals seeking weight-loss treatment, 15 % met YFAS addiction criteria.
Since the implementation of the YFAS, individuals with compulsive overeating tendencies who qualify for full YFAS ‘food addiction’ criteria have been shown to exhibit similar clinical characteristics as those diagnosed with SUDS (e.g., mental illness comorbidity) [11••, 83]. In 67 weight-loss surgery patients, Clark et al. showed that individuals meeting addiction criteria on the YFAS were more likely to experience worse post-surgery weight loss and experience more post-surgery substance use [109]. Those that meet full YFAS criteria endorse the same pattern of mental illness comorbidity as individuals with SUDs diagnoses [110]. Interestingly, overweight individuals that met full YFAS addiction criteria presented with significantly more depressive symptoms than those overweight individuals who did not meet full YFAS criteria [111]. In another sample of 72 obese adults, 25 % of participants met full YFAS criteria [11••]. Of those that met YFAS criteria, 72.2 % almost met diagnosis for BED, 27.8 % for severe depression, and 33.3 % for childhood ADHD, significantly more than those without a ‘food addiction’ diagnosis [11••].
More recently, the YFAS has been adapted for use in children (YFAS-C) [112], which has yielded further validation of the ‘food addiction’ phenotype. In a sample of 75 children of variable weight, greater YFAS scores were associated with greater BMI and more emotional eating. Across dimensions, 24.7 % reported tolerance, 18.9 % reported withdrawal symptoms, 29.3 % felt a loss of control, and 38.6 % presented with more than three symptoms. Overall, 7.2 % of children met full YFAS addiction criteria, which is comparable to those reported in adults [112]. In 50 adolescents seeking weight loss treatment, Meule et al. found that 38 % of patients met full YFAS criteria and presented with more bingeing, food craving, and symptoms of depression [113]. Generally, YFAS criteria produce similar results in adults and children providing more evidence for a robust phenotype [114].
Although greater YFAS scores have been associated with difficulties in reducing weight, depressive symptoms, and attentional specificity for food cues, several studies have reported no associations with overall BMI [115]. The relationship between BMI and YFAS score has been hypothesized to be nonlinear in nature, where obese individuals present with the highest YFAS scores, followed by those overweight and underweight. Not intuitively, underweight individuals display more preoccupation with food than individuals of normal weight, suggesting a relationship with food preoccupation and attentional motivation [115]. Also surprisingly, extremely obese individuals plateau in their YFAS scores, which may result from a limit in the ability to increase their BMI further [115]. Therefore, further investigations are needed to delineate the exact causes and ‘culprits’ in the addictive phenotype of compulsive overeating.
YFAS and Associations with Cognitive, Imaging, and Genetic Evidence
Biological support for the criteria used on the YFAS has come from genetic and brain imaging studies. In an fMRI study of 48 females attempting to achieve a healthy weight, YFAS addiction scores were positively correlated with response to food cues [31••]. Furthermore, individuals with greater YFAS scores showed greater activation of the ACC and medial orbitofrontal cortex, which has previously been associated with an anticipatory response to food [31••]. Interestingly, individuals meeting full YFAS criteria showed decreased lateral orbitofrontal cortex activation, suggesting an association between decreased reward experience after receiving a food reward, similar to the ‘tolerance’ effect seen in SUDs [31••].
Furthermore, the hedonic (‘liking’) and craving (‘wanting’) distinction in the ‘food addiction’ phenotype has previously been reported to be positively correlated with the YFAS score from genetic studies. Evidence from genetics supports the role of hedonic responsiveness in individuals that meet full YFAS criteria [11••]. In a candidate-gene study of the OPRM1 variant A118G in adults (N = 145), dominant and recessive homozygotes were associated with an increased risk for food addiction criteria. Authors also showed that a greater YFAS score and diagnosis of ‘food addiction’ were significantly positively correlated with a greater hedonic response [116]. Individuals that meet full YFAS diagnosis criteria significantly endorse binge eating, hedonic eating, emotional eating, food craving, and snacking compared to non ‘food addicts’ [11••]. The parallels between compulsive eating and drug seeking behaviors are supported by the cravings and hedonic experiences reported by individuals on the YFAS [11••].
YFAS, the DSM-5, and Future Research
The arrival of the DSM-5 has hailed with it modifications of SUDs diagnostic criteria. The new SUDs diagnostic criteria include the addition of symptoms, including cravings. While some of the new SUDs criteria are already endorsed by individuals with compulsive overeating phenotypes (e.g., cravings) [11••], other new criteria (e.g., withdrawal and intoxication) have very little to weak supporting evidence [103, 117•]. Meule and Gearhardt (2014) have evaluated the YFAS in comparison to the DSM-5 SUDs criteria and the relevance of the currently in-use YFAS dimensions [117•]. In regards to compulsive overeating, several SUDs-based diagnostic criteria have been shown to be more relevant for ‘food addiction’ diagnoses, including excessive binging, attempts to cut down, and use despite harm [117•, 118]. ‘Craving’ has been reported in individuals diagnosed with BED or overconsumption and may be added to future versions of the YFAS [117•]. On the other hand, tolerance and withdrawal criteria are not readily endorsed by individuals with compulsive overeating, suggesting that they may be less important for diagnosing ‘food addiction’ phenotype [117•, 118]. Therefore, SUDs criteria which do not have evidence for association with compulsive overeating are cautioned for using to diagnose a ‘food addiction’. Authors call for the adjustments of diagnostic thresholds; therefore, further research is required to evaluate and refine ‘food addiction’ diagnostic criteria [117_ENREF_117].
Conclusion
The abundance of similarities between compulsive overeating and substance addictions puts forth a case for a ‘food addiction’ phenotype as a valid, diagnosable disorder. Whether ‘food addiction’ represents a subtype of BED patients with addictive symptoms or individuals truly pathologically driven to consume food (e.g., fats, sugars, salt, caffeine, etc.) requires further investigation and more evidence.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
James W. The epidemiology of obesity: the size of the problem. J Intern Med. 2008;263(4):336–52.
Sorof J, Daniels S. Obesity hypertension in children a problem of epidemic proportions. Hypertension. 2002;40(4):441–7.
Landsberg L, Aronne LJ, Beilin LJ, Burke V, Igel LI, Lloyd‐Jones D, et al. Obesity‐related hypertension: pathogenesis, cardiovascular risk, and treatment—a position paper of the obesity society and the American society of hypertension. Obesity. 2013;21(1):8–24.
Eckel RH, Kahn SE, Ferrannini E, Goldfine AB, Nathan DM, Schwartz MW, et al. Obesity and type 2 diabetes: what can be unified and what needs to be individualized? J Clin Endocrinol Metab. 2011;96(6):1654–63.
Littleton SW. Impact of obesity on respiratory function. Respirology. 2012;17(1):43–9.
Nikolopoulou A, Kadoglou NP. Obesity and metabolic syndrome as related to cardiovascular disease. Expert Rev Cardiovasc Ther. 2012;10(7):933–9.
Fock KM, Khoo J. Diet and exercise in management of obesity and overweight. J Gastroenterol Hepatol. 2013;28 Suppl 4:59–63.
Davis C. From passive overeating to food addiction: a spectrum of compulsion and severity. ISRN Obesity. 2013;2013:20. This review describes the dimensional scale of compulsive overeating. It also considers the overlapping symptomology between compulsive overeating and addiction phenotypes, in both human and animal studies.
Vancampfort D, Vanderlinden J, De Hert M, Adamkova M, Skjaerven LH, Catalan-Matamoros D, et al. A systematic review on physical therapy interventions for patients with binge eating disorder. Disabil Rehabil. 2013;35(26):2191–6.
Brownley KA, Berkman ND, Sedway JA, Lohr KN, Bulik CM. Binge eating disorder treatment: a systematic review of randomized controlled trials. Int J Eat Disord. 2007;40(4):337–48.
Davis C, Curtis C, Levitan RD, Carter JC, Kaplan AS, Kennedy JL. Evidence that ‘food addiction’ is a valid phenotype of obesity. Appetite. 2011;57(3):711–7. This article to validates the Yale Food Addiction Scale (YFAS) in a sample of obese adults, providing further evidence of the association between YFAS scores and the ‘food addiction’ phenotype. Individuals presenting with ‘food addiction’ showed greater impulsivity, emotional reactivity and comorbidity with attention-deficit/ hyperactivity disorder, binge eating disorder and depression.
Ifland J, Preuss H, Marcus M, Rourke K, Taylor W, Burau K, et al. Refined food addiction: a classic substance use disorder. Med Hypotheses. 2009;72(5):518–26.
Davis C, Carter JC. Compulsive overeating as an addiction disorder. A review of theory and evidence. Appetite. 2009;53(1):1–8.
Volkow ND, Wang G-J, Fowler JS, Telang F. Overlapping neuronal circuits in addiction and obesity: evidence of systems pathology. Philos Trans Royal Soc London B: Biol Sci. 2008;363(1507):3191–200.
Berridge KC. Liking’ and ‘wanting’ food rewards: brain substrates and roles in eating disorders. Physiol Behav. 2009;97(5):537–50.
Davis C. Evolutionary and neuropsychological perspectives on addictive behaviors and addictive substances: relevance to the “food addiction” construct. Subst Abuse Rehab. 2014;5:129.
Bellisari A. Evolutionary origins of obesity. Obesity Rev: Off J Int Assoc Study Obesity. 2008;9(2):165–80.
Cummins S, Macintyre S. Food environments and obesity—neighbourhood or nation? Int J Epidemiol. 2006;35(1):100–4.
Morland KB, Evenson KR. Obesity prevalence and the local food environment. Health Place. 2009;15(2):491–5.
Rainer G. Behavioral flexibility and the frontal lobe. Neuron. 2007;53(3):321–3.
Uchibe E, Doya K. Finding intrinsic rewards by embodied evolution and constrained reinforcement learning. Neural Netw. 2008;21(10):1447–55.
Kalivas PW, Volkow ND. The neural basis of addiction: a pathology of motivation and choice. Am J Psych. 2014.
Volkow ND, Wang GJ, Tomasi D, Baler RD. Obesity and addiction: neurobiological overlaps. Obes Rev. 2013;14(1):2–18. This article reviews the similarities between compulsive overeating and substance use disorders, with a particular focus on evidence from neuroimaging in areas contributing to reward processing, incentive motivation, self-inhibition and other aspects of reward processing.
Baudonnat M, Huber A, David V, Walton ME. Heads for learning, tails for memory: reward, reinforcement and a role of dopamine in determining behavioral relevance across multiple timescales. Frontiers Neurosci. 2013;7.
Robinson TE, Berridge KC. Review. The incentive sensitization theory of addiction: some current issues. Philos Trans R Soc Lond Ser B Biol Sci. 2008;363(1507):3137–46.
Berridge KC, Robinson TE, Aldridge JW. Dissecting components of reward: ‘liking’, ‘wanting’, and learning. Curr Opin Pharmacol. 2009;9(1):65–73.
Berridge KC. Motivation concepts in behavioral neuroscience. Physiol Behav. 2004;81(2):179–209.
Volkow ND, Fowler JS, Wang G-J, Goldstein RZ. Role of dopamine, the frontal cortex and memory circuits in drug addiction: insight from imaging studies. Neurobiol Learn Mem. 2002;78(3):610–24.
Volkow ND, Wang G-J, Telang F, Fowler JS, Logan J, Childress A-R, et al. Cocaine cues and dopamine in dorsal striatum: mechanism of craving in cocaine addiction. J Neurosci. 2006;26(24):6583–8.
Kühn S, Gallinat J. Common biology of craving across legal and illegal drugs—a quantitative meta-analysis of cue-reactivity brain response. Eur J Neurosci. 2011;33(7):1318–26.
Gearhardt AN, Yokum S, Orr PT, Stice E, Corbin WR, Brownell KD. The neural correlates of “food addiction. Arch Gen Psychiatry. 2011;68(8):808–16. This fMRI investigation provides further evidence for the similarities in neural networks implicated in substance use disorders and ‘food addiction’. Researchers showed that individuals with higher food addiction scores showed greater activation of the anterior cingulate cortex (ACC), medial orbitofrontal cortex (OFC), and amygdala in response to food reward anticipation. Interestingly, these individuals also showed less activation of the lateral OFC after receiving a food reward.
Meule A, Lutz A, Vögele C, Kübler A. Women with elevated food addiction symptoms show accelerated reactions, but no impaired inhibitory control, in response to pictures of high-calorie food-cues. Eat Behav. 2012;13(4):423–8.
Wise RA, Koob GF. The development and maintenance of drug addiction. Neuropsychopharmacology. 2014;39(2):254–62.
Volkow ND, Wang GJ, Fowler JS, Tomasi D, Telang F, Baler R. Addiction: decreased reward sensitivity and increased expectation sensitivity conspire to overwhelm the brain’s control circuit. Bioessays. 2010;32(9):748–55.
Gardner EL. Addiction and brain reward and antireward pathways. 2011.
Stice E, Spoor S, Ng J, Zald DH. Relation of obesity to consummatory and anticipatory food reward. Physiol Behav. 2009;97(5):551–60.
Burger KS, Stice E. Variability in reward responsivity and obesity: evidence from brain imaging studies. Current Drug Abuse Rev. 2011;4(3):182.
Parylak SL, Koob GF, Zorrilla EP. The dark side of food addiction. Physiol Behav. 2011;104(1):149–56.
Bromberg-Martin ES, Matsumoto M, Hikosaka O. Dopamine in motivational control: rewarding, aversive, and alerting. Neuron. 2010;68(5):815–34.
Lammel S, Ion Daniela I, Roeper J, Malenka RC. Projection-specific modulation of dopamine neuron synapses by aversive and rewarding stimuli. Neuron. 2011;70(5):855–62.
Volkow ND, Wang G-J, Tomasi D, Baler RD. The addictive dimensionality of obesity. Biol Psychiatry. 2013;73(9):811–8.
Baik J-H. Dopamine signaling in reward-related behaviors. Frontiers Neural Circ. 2013;7.
Beaulieu J-M, Gainetdinov RR. The physiology, signaling, and pharmacology of dopamine receptors. Pharmacol Rev. 2011;63(1):182–217.
Dichter GS, Damiano CA, Allen JA. Reward circuitry dysfunction in psychiatric and neurodevelopmental disorders and genetic syndromes: animal models and clinical findings. J Neurodev Disord. 2012;4(1):19.
Hurley SW, Johnson AK. The role of the lateral hypothalamus and orexin in ingestive behavior: a model for the translation of past experience and sensed deficits into motivated behaviors. Front Syst Neurosci. 2014;8:216.
Havel PJ. Peripheral signals conveying metabolic information to the brain: short-term and long-term regulation of food intake and energy homeostasis. Exp Biol Med. 2001;226(11):963–77.
Woods SC. Gastrointestinal satiety signals I. An overview of gastrointestinal signals that influence food intake. Am J Physiol-Gastrointestinal Liver Physiol. 2004;286(1):G7–G13.
Roth JD, Roland BL, Cole RL, Trevaskis JL, Weyer C, Koda JE, et al. Leptin responsiveness restored by amylin agonism in diet-induced obesity: evidence from nonclinical and clinical studies. Proc Natl Acad Sci. 2008;105(20):7257–62.
Wielinga PY, Löwenstein C, Muff S, Munz M, Woods SC, Lutz TA. Central amylin acts as an adiposity signal to control body weight and energy expenditure. Physiol Behav. 2010;101(1):45–52.
Woods SC, Seeley RJ. Adiposity signals and the control of energy homeostasis. Nutrition. 2000;16(10):894–902.
Geary N. Endocrine controls of eating: CCK, leptin, and ghrelin. Physiol Behav. 2004;81(5):719–33.
Schwartz MW, Woods SC, Seeley RJ, Barsh GS, Baskin DG, Leibel RL. Is the energy homeostasis system inherently biased toward weight gain? Diabetes. 2003;52(2):232–8.
Zigman JM, Elmquist JK. Minireview: from anorexia to obesity—the yin and yang of body weight control. Endocrinology. 2003;144(9):3749–56.
Opland DM, Leinninger GM, Myers Jr MG. Modulation of the mesolimbic dopamine system by leptin. Brain Res. 2010;1350:65–70.
Leinninger GM, Opland DM, Jo YH, Faouzi M, Christensen L, Cappellucci LA, et al. Leptin action via neurotensin neurons controls orexin, the mesolimbic dopamine system and energy balance. Cell Metab. 2011;14(3):313–23.
Mebel DM, Wong JC, Dong YJ, Borgland SL. Insulin in the ventral tegmental area reduces hedonic feeding and suppresses dopamine concentration via increased reuptake. Eur J Neurosci. 2012;36(3):2336–46.
Egecioglu E, Skibicka KP, Hansson C, Alvarez-Crespo M, Friberg PA, Jerlhag E, et al. Hedonic and incentive signals for body weight control. Rev Endocr Metab Disord. 2011;12(3):141–51.
Cone JJ, McCutcheon JE, Roitman MF. Ghrelin acts as an interface between physiological state and phasic dopamine signaling. J Neurosci: Off J Soc Neurosci. 2014;34(14):4905–13.
Volkow ND, Wang GJ, Baler RD. Reward, dopamine and the control of food intake: implications for obesity. Trends Cogn Sci. 2011;15(1):37–46.
Heber D, Carpenter CL. Addictive genes and the relationship to obesity and inflammation. Mol Neurobiol. 2011;44(2):160–5.
Sturgess JE, George TP, Kennedy JL, Heinz A, Muller DJ. Pharmacogenetics of alcohol, nicotine and drug addiction treatments. Addict Biol. 2011;16(3):357–76.
Nutt DJ, Lingford-Hughes A, Erritzoe D, Stokes PR. The dopamine theory of addiction: 40 years of highs and lows. Nat Rev Neurosci. 2015;16(5):305–12.
Michaelides M, Thanos PK, Volkow ND, Wang GJ. Dopamine-related frontostriatal abnormalities in obesity and binge-eating disorder: emerging evidence for developmental psychopathology. Int Rev Psychiatry (Abingdon, England). 2012;24(3):211–8.
Thompson J, Thomas N, Singleton A, Piggot M, Lloyd S, Perry E, et al. D2 dopamine receptor gene (DRD2) Taql A polymorphism: reduced dopamine D2 receptor binding in the human striatum associated with the A1 allele. Pharmacogenet Genomics. 1997;7(6):479–84.
Peciña M, Mickey BJ, Love T, Wang H, Langenecker SA, Hodgkinson C, et al. DRD2 polymorphisms modulate reward and emotion processing, dopamine neurotransmission and openness to experience. Cortex. 2013;49(3):877–90.
Noble EP. Addiction and its reward process through polymorphisms of the D2 dopamine receptor gene: a review. Eur Psychiatry. 2000;15(2):79–89.
Chen AL, Blum K, Chen TJ, Giordano J, Downs BW, Han D, et al. Correlation of the Taq 1 dopamine D2 receptor gene and percent body fat in obese and screened control subjects: a preliminary report. Food Func. 2012;3(1):40–8.
Davis C, Levitan RD, Kaplan AS, Carter J, Reid C, Curtis C, et al. Reward sensitivity and the D2 dopamine receptor gene: a case–control study of binge eating disorder. Prog Neuro-Psychopharmacol Biol Psychiatry. 2008;32(3):620–8.
Epstein LH, Temple JL, Neaderhiser BJ, Salis RJ, Erbe RW, Leddy JJ. Food reinforcement, the dopamine D(2) receptor genotype, and energy intake in obese and nonobese humans. Behav Neurosci. 2007;121(5):877–86.
Lett TA, Wallace TJ, Chowdhury NI, Tiwari AK, Kennedy JL, Muller DJ. Pharmacogenetics of antipsychotic-induced weight gain: review and clinical implications. Mol Psychiatry. 2012;17(3):242–66.
Kao AC, Müller DJ. Genetics of antipsychotic-induced weight gain: update and current perspectives. Pharmacogenomics. 2013;14(16):2067–83.
Fuke S, Suo S, Takahashi N, Koike H, Sasagawa N, Ishiura S. The VNTR polymorphism of the human dopamine transporter (DAT1) gene affects gene expression. Pharmacogenomics J. 2001;1(2):152–6.
van Dyck CH, Malison RT, Jacobsen LK, Seibyl JP, Staley JK, Laruelle M, et al. Increased dopamine transporter availability associated with the 9-repeat allele of the SLC6A3 gene. J Nucl Med. 2005;46(5):745–51.
van de Giessen EM, de Win MM, Tanck MW, van den Brink W, Baas F, Booij J. Striatal dopamine transporter availability associated with polymorphisms in the dopamine transporter gene SLC6A3. J Nucl Med. 2009;50(1):45–52.
Shumay E, Wang G-J, Volkow N, Telang F, Jayne M, Wong C, et al. Exploring the links between the brain dopamine transporter availability, DAT1 genotype and body mass index. J Nucl Med Meeting Abst. 2012;53(1_MeetingAbstracts):195.
Davis C, Levitan RD, Kaplan AS, Carter J, Reid C, Curtis C, et al. Dopamine transporter gene (DAT1) associated with appetite suppression to methylphenidate in a case–control study of binge eating disorder. Neuropsychopharmacology. 2007;32(10):2199–206.
Nathan PJ, Bullmore ET. From taste hedonics to motivational drive: central μ-opioid receptors and binge-eating behaviour. 7. 2009.
Smith DG, Robbins TW. The neurobiological underpinnings of obesity and binge eating: a rationale for adopting the food addiction model. Biol Psychiatry. 2013;73(9):804–10.
Haerian BS, Haerian MS. OPRM1 rs1799971 polymorphism and opioid dependence: evidence from a meta-analysis. Pharmacogenomics. 2013;14(7):813–24.
Davis C, Zai C, Levitan RD, Kaplan AS, Carter JC, Reid-Westoby C, et al. Opiates, overeating and obesity: a psychogenetic analysis. Int J Obesity (2005). 2011;35(10):1347–54.
Bach P, Vollsta Dt-Klein S, Kirsch M, Hoffmann S, Jorde A, Frank J et al. Increased mesolimbic cue-reactivity in carriers of the mu-opioid-receptor gene OPRM1 A118G polymorphism predicts drinking outcome: a functional imaging study in alcohol dependent subjects. European neuropsychopharmacology : the journal of the European College of Neuropsychopharmacology. 2015.
Haghighi A, Melka MG, Bernard M, Abrahamowicz M, Leonard GT, Richer L, et al. Opioid receptor mu 1 gene, fat intake and obesity in adolescence. Mol Psychiatry. 2014;19(1):63–8.
Clarke TK, Crist RC, Kampman KM, Dackis CA, Pettinati HM, O’Brien CP, et al. Low frequency genetic variants in the mu-opioid receptor (OPRM1) affect risk for addiction to heroin and cocaine. Neurosci Lett. 2013;542:71–5.
Carpenter CL, Wong AM, Li Z, Noble EP, Heber D. Association of dopamine D2 receptor and leptin receptor genes with clinically severe obesity. Obesity. 2013;21(9):E467–E73.
Hardman CA, Rogers PJ, Timpson NJ, Munafo MR. Lack of association between DRD2 and OPRM1 genotypes and adiposity. Int J Obes. 2014;38(5):730–6.
Zhang Y, Picetti R, Butelman ER, Ho A, Blendy JA, Kreek MJ. Mouse model of the OPRM1 (A118G) polymorphism: differential heroin self-administration behavior compared with wild-type mice. Neuropsychopharmacology. 2015;40(5):1091–100.
Nogueiras R, Seeley RJ. Our evolving understanding of the interaction between leptin and dopamine system to regulate ingestive behaviors. Mol Metab. 2012;1(1–2):8–9.
Kern A, Albarran-Zeckler R, Walsh HE, Smith RG. Apo-ghrelin receptor forms heteromers with DRD2 in hypothalamic neurons and is essential for anorexigenic effects of DRD2 agonism. Neuron. 2012;73(2):317–32.
Davis JF, Choi DL, Schurdak JD, Fitzgerald MF, Clegg DJ, Lipton JW, et al. Leptin regulates energy balance and motivation through action at distinct neural circuits. Biol Psychiatry. 2011;69(7):668–74.
al’Absi M, Hooker S, Fujiwara K, Kiefer F, von der Goltz C, Cragin T, et al. Circulating leptin levels are associated with increased craving to smoke in abstinent smokers. Pharmacol Biochem Behav. 2011;97(3):509–13.
Morrison CD. Leptin signaling in brain: a link between nutrition and cognition? Biochim Biophys Acta (BBA) - Mol Basis Dis. 2009;1792(5):401–8.
Davis JF. Adipostatic regulation of motivation and emotion. Discov Med. 2010;9(48):462–7.
van Rossum CTM, Hoebee B, van Baak MA, Mars M, Saris WHM, Seidell JC. Genetic variation in the leptin receptor gene, leptin, and weight gain in young Dutch adults. Obes Res. 2003;11(3):377–86.
Voisey J, Carroll L, van Daal A. Melanocortins and their receptors and antagonists. Curr Drug Targets. 2003;4(7):586–97.
Cui H, Mason BL, Lee C, Nishi A, Elmquist JK, Lutter M. Melanocortin 4 receptor signaling in dopamine 1 receptor neurons is required for procedural memory learning. Physiol Behav. 2012;106(2):201–10.
Hsu R, Taylor JR, Newton SS, Alvaro JD, Haile C, Han G, et al. Blockade of melanocortin transmission inhibits cocaine reward. Eur J Neurosci. 2005;21(8):2233–42.
Shelkar GP, Kale AD, Singh U, Singru PS, Subhedar NK, Kokare DM. Alpha-melanocyte stimulating hormone modulates ethanol self-administration in posterior ventral tegmental area through melanocortin-4 receptors. Addict Biol. 2015;20(2):302–15.
Thorleifsson G, Walters GB, Gudbjartsson DF, Steinthorsdottir V, Sulem P, Helgadottir A, et al. Genome-wide association yields new sequence variants at seven loci that associate with measures of obesity. Nat Genet. 2009;41(1):18–24.
Xi B, Chandak GR, Shen Y, Wang Q, Zhou D. Association between common polymorphism near the MC4R gene and obesity risk: a systematic review and meta-analysis. PLoS One. 2012;7(9), e45731.
Yilmaz Z, Davis C, Loxton NJ, Kaplan AS, Levitan RD, Carter JC, et al. Association between MC4R rs17782313 polymorphism and overeating behaviors. Int J Obesity (2005). 2015;39(1):114–20.
Porfirio MC, Giovinazzo S, Cortese S, Giana G, Lo-Castro A, Mouren MC, et al. Role of ADHD symptoms as a contributing factor to obesity in patients with MC4R mutations. Med Hypotheses. 2015;84(1):4–7.
Zheng H, Lenard N, Shin A, Berthoud H-R. Appetite control and energy balance regulation in the modern world: reward-driven brain overrides repletion signals. Int J Obes. 2009;33:S8–S13.
Association AP. Diagnostic and statistical manual of mental disorders: DSM-5. ManMag; 2003.
Cassin SE, von Ranson KM. Is binge eating experienced as an addiction? Appetite. 2007;49(3):687–90.
Gearhardt AN, Corbin WR, Brownell KD. Preliminary validation of the Yale food addiction scale. Appetite. 2009;52(2):430–6. This article reports the first validation of the Yale Food Addiction Scale (YFAS), developed to assess a ‘food addiction’ phenotype. In a sample of young adults, the YFAS predicted binge-eating behavior better than other psychometric tools.
Association AP, Association AP. Diagnostic and statistical manual-text revision (DSM-IV-TRim, 2000). Am Psych Assoc; 2000.
Brunault P, Ballon N, Gaillard P, Réveillère C, Courtois R. Validation of the french version of the Yale food addiction scale: an examination of its factor structure, reliability, and construct validity in a nonclinical sample. Can J Psychiatry. 2014;59(5):276–84.
Chen G, Tang Z, Guo G, Liu X, Xiao S. The Chinese version of the Yale food addiction scale: an examination of its validation in a sample of female adolescents. Eat Behav. 2015;18:97–102.
Clark SM, Saules KK. Validation of the Yale food addiction scale among a weight-loss surgery population. Eat Behav. 2013;14(2):216–9.
Swendsen J, Conway KP, Degenhardt L, Glantz M, Jin R, Merikangas KR, et al. Mental disorders as risk factors for substance use, abuse and dependence: results from the 10‐year follow‐up of the national comorbidity survey. Addiction. 2010;105(6):1117–28.
Eichen DM, Lent MR, Goldbacher E, Foster GD. Exploration of “food addiction” in overweight and obese treatment-seeking adults. Appetite. 2013;67:22–4.
Gearhardt AN, Roberto CA, Seamans MJ, Corbin WR, Brownell KD. Preliminary validation of the Yale food addiction scale for children. Eat Behav. 2013;14(4):508–12.
Meule A, Hermann T, Kubler A. Food addiction in overweight and obese adolescents seeking weight-loss treatment. Eur Eating Disord Rev: J Eating Disord Assoc. 2015;23(3):193–8.
Burrows T, Meule A. Food addiction’. What happens in childhood? Appetite. 2015;89:298–300.
Meule A. Food addiction and body-mass-index: a non-linear relationship. Med Hypotheses. 2012;79(4):508–11.
Davis C, Loxton NJ. A psycho-genetic study of hedonic responsiveness in relation to “food addiction. Nutrients. 2014;6(10):4338–53.
Meule A, Gearhardt AN. Food addiction in the light of DSM-5. Nutrients. 2014;6(9):3653–71. This article provides a detailed comparison between currently proposed dimensions of ‘food addiction’ and new criteria for substance use disorders (SUDs) diagnoses according to the DSM-5.
Meule A. How prevalent is “Food Addiction”? Frontiers Psych. 2011;2.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Nina Carlier, Victoria S. Marshe, Jana Cmorejova, Caroline Davis, and Daniel J. Müller declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Genetic Disorders
Nina Carlier and Victoria S. Marshe contributed equally to this work.
Rights and permissions
About this article

Cite this article
Carlier, N., Marshe, V.S., Cmorejova, J. et al. Genetic Similarities between Compulsive Overeating and Addiction Phenotypes: A Case for “Food Addiction”?. Curr Psychiatry Rep 17, 96 (2015). https://doi.org/10.1007/s11920-015-0634-5
Published:
DOI: https://doi.org/10.1007/s11920-015-0634-5