
Abstract
In contrast to the association of insomnia with mental health, its association with physical health has remained largely unexplored until recently. Based on findings that insomnia with objective short sleep duration is associated with activation of both limbs of the stress system and other indices of physiological hyperarousal, which should adversely affect physical and mental health, we have recently demonstrated that this insomnia phenotype is associated with a significant risk of cardiometabolic and neurocognitive morbidity and mortality. In contrast, insomnia with normal sleep duration is associated with sleep misperception and cognitive-emotional arousal, but not with signs of physiological hyperarousal or cardiometabolic or neurocognitive morbidity. Interestingly, both insomnia phenotypes are associated with mental health, although most likely through different pathophysiological mechanisms. We propose that objective measures of sleep duration may become part of the routine evaluation and diagnosis of insomnia, and that these two insomnia phenotypes may respond differentially to biological versus psychological treatments.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The prevalence of insomnia in the general population ranges between 8 % and 40 %, depending on the definition used. While 20–30 % of the general population has poor sleep (i.e., insomnia, symptoms of difficulty initiating or maintaining sleep, early morning awakening, or non-restorative sleep at any given time), another 8–10 % of the population suffers from chronic insomnia [1, 2]. Also, about 4 % of the population uses sleeping pills on a regular basis [3]. However, the connection of insomnia with significant medical morbidity has not been examined until very recently. This has led to the view of insomnia and its associated mental and physical health complaints as a minor problem from a public health perspective.
A factor that may have contributed to this lack of firm association between insomnia and significant medical morbidity is the definitions used for this disorder and the lack of validated objective/biological markers. Sleep disorders were included for the first time in the Diagnostic and Statistical Manual of Mental Disorders (DSM)-III-R [4] in 1987, and provided overall diagnostic criteria for “insomnia disorders” based on the subjective complaints of difficulty initiating or maintaining sleep or of non-restorative sleep, occurring at least three times a week for at least 1 month, and associated daytime functioning complaints. The DSM-IV-TR eliminated the overall diagnostic criteria for “insomnia disorders”, as well as the frequency criterion, maintained the diagnoses of “primary insomnia”, “dysomnia NOS [not otherwise specified]”, insomnia “related to another mental disorder”, “due to a general medical condition”, and introduced “substance-induced insomnia” [5]. The DSM-5 has eliminated the different insomnia diagnoses in DSM-IV-TR to reintroduce overall diagnostic criteria for “insomnia disorder” with specification of comorbid mental and/or physical conditions, so that no causal attributions between insomnia and the physical/mental condition are made, and has extended the duration criterion from 1 month to 3 months [6]. The latter change is an acknowledgement that chronicity is what differentiates insomnia as a disorder versus insomnia symptoms, that is, poor sleep due to underlying, identifiable physical, emotional, or drug-related factors.
The International Classification of Sleep Disorders (ICSD), and its revised form ICSD-R (1997), also defined insomnia based on subjective sleep and daytime functioning complaints, but, in contrast, attempted to identify subtypes based on “intrinsic” factors, such as etiology (i.e., “psychophysiological”), age of onset (i.e., “idiopathic insomnia”), degree of discrepancy between objective sleep findings and subjective perception of sleep (i.e., “sleep state misperception”), or “extrinsic” environmental factors, such as “inadequate sleep hygiene”, “food-allergy”, or “altitude insomnia”. However, these subtypes, even when refined in the ICSD-2 [7], have not proven to be clinically useful, and the reliability and validity of DSM and ICSD diagnoses is modest, at best [8••].
Although the objective sleep of insomniacs is different than that of normal sleepers, polysomnography (PSG) variables are not required or recommended for the diagnosis of the disorder. In fact, PSG criteria have not proven to be useful in terms of differential diagnosis or severity assessment, and are not currently used in clinical practice. The sleep laboratory is useful for the evaluation of patients with sleep-disordered breathing (SDB), the diagnosis of narcolepsy, and the differential diagnosis of idiopathic versus psychogenic hypersomnia [9, 10], as well as the study of the initial effectiveness, continued efficacy or tolerance, and potential withdrawal effects of a hypnotic drugs. The validity and clinical utility of sleep laboratory testing for diagnosing insomnia has been evaluated in large studies [11, 12] that have shown that PSG measures, such as latency to sleep onset, total sleep time, number of arousals and awakenings, sleep efficiency, or sleep stages, are not useful in the diagnosis or differential diagnosis, including subtyping of insomnia, except to confirm or exclude other sleep pathologies when there is reasonable evidence from clinical history (e.g., SDB or periodic limb movements). The current consensus is, therefore, that PSG is not recommended for routine, differential diagnosis, or severity assessment of insomnia in clinical practice [13].
In this review article, we present evidence that objective measures of sleep are useful in predicting the medical severity of insomnia (i.e., cardiometabolic and neurocognitive morbidity and mortality) and that should be considered in the new classification of insomnia.
Insomnia and the Stress System
In the last two decades, several models have been proposed to understand the etiology and pathophysiology of insomnia, and most of them have emphasized the importance of the joint effect of stress and psychological factors in the pathogenesis of insomnia [14]. The characteristic psychological profile of patients with insomnia, consisting of cognitive–emotional hyperarousal (i.e., obsessive, anxious, ruminative, and dysthymic personality traits) and emotion-oriented coping strategies [14–16], is thought to be present pre-morbidly and play a key role in the etiology of the disorder [14, 17–19, 20••]. Insomnia is associated with precipitating life events [21] and cognitive-emotional arousal [14], and is perceived by the patient as stressful on its own. Thus, insomnia should be expected to be associated with activation of the stress system.
Stress has been associated with the activation of the hypothalamic–pituitary–adrenal (HPA) and the sympatho-adrenal-medullary axes, whereas corticotropin-releasing hormone (CRH) and cortisol (products of the hypothalamus and adrenals, respectively), and catecholamines (products of the sympathetic system) are known to cause arousal and sleeplessness in humans and animals. However, sleep, and particularly deep sleep, appears to have an “anti-stress” effect, as it is associated with an inhibitory effect on the stress system, including its main two components, the HPA axis and the sympathetic system.
While the majority of early studies reported no difference between subjectively defined “poor sleepers” and controls in the levels of cortisol secretion [22–24], later studies found that 24-h urinary free cortisol, norepinephrine, and catecholamine metabolites levels were either increased in patients with insomnia with objective sleep disturbances compared with controls, or were correlated with PSG indices of sleep disturbance in insomnia patients [25–31]. The few exceptions might be related to the fact that the objective sleep of patients with insomnia was very similar to that of controls [32] or to lack of statistical power and controls not being carefully selected [33, 34]. In addition, it was shown that middle-aged healthy individuals were more vulnerable to the sleep-disturbing effects of the stimulating hormones of the HPA axis, that is, CRH, which may explain physiologically the increased prevalence of insomnia in older patients [35].Furthermore, other studies have demonstrated that this type of insomnia is associated with increased nocturnal heart rate and impaired heart rate variability [36, 37], increased overall oxygen consumption (VO2), a measure of whole-body metabolic rate [38, 39], and increased pupil size, indicative of sympathetic system activation [40], but not in insomnia defined only on subjective measures [41, 42].
Another paradox with patients with insomnia who typically complain that they are fatigued and sleepy during the day is that during the Multiple Sleep Latency Test (MSLT) they have either similar or increased daytime sleep latencies when compared with controls [42–45]. In fact, several studies have shown that, within patients with insomnia, those with shorter objective sleep duration show longer sleep latencies in the MSLT [44, 46–48] and are more alert in vigilance tests [38, 39, 46]. This is in contrast to normal individuals who, after sleep deprivation, experience significantly reduced sleep latencies on the MSLT and decreased alertness in vigilance tests, that is, physiological sleepiness [49, 50]. Thus, long latencies in the MSLT may represent a reliable marker of physiological hyperarousal in insomnia patients.
Finally, evidence about the presence of central nervous system hyperarousal in insomnia comes from studies in human subjects using neuroimaging [51, 52], and spectral [53, 54], arousal [55], and event-related [56] electroencephalography analyses, as well as from studies on the neural circuitry of stress-induced insomnia in rats [57]. Increased cortical arousal during sleep is present to a variable degree in all patients with insomnia [53–56] and may explain why they perceive their sleep as wake and as non-restorative [58, 59••].
Insomnia and Cardiometabolic Morbidity
Until recently, chronic insomnia has not been firmly linked with significant medical morbidity, such as cardiovascular disease. Several surveys have shown a significant relationship between difficulty falling asleep or poor sleep with cardiometabolic outcomes such as hypertension [60–62] and diabetes [63–66]. For example, persistent complaints of difficulty initiating or maintaining sleep were associated with an increased risk of hypertension [61], acute myocardial infarction [62], and incident type 2 diabetes [63–66]. However, these studies showed relatively small effect sizes and did not include a PSG evaluation so as to control for SDB or other sleep pathology. The findings of these early studies were dismissed as methodologically flawed by many clinicians and researchers alike [67, 68]. In fact, at least one report showed a reduced mortality rate for those individuals complaining of sleep difficulties after 6 years of follow up [69].
Given the well-established association of hypercortisolemia with significant medical morbidity (i.e., hypertension, diabetes, metabolic syndrome, osteoporosis, and others) [25–31], we hypothesized that insomnia with objective short sleep duration is associated with significant cardiometabolic morbidity and mortality. A series of recent epidemiological studies from the Penn State Adult Cohort [1], which used in-laboratory PSG, have shown that insomnia with objective short sleep duration is associated with a high risk of hypertension [70••, 71••], diabetes [72••], and mortality [73]. For example, compared with normal sleepers who slept ≥6 h per night, the highest odds of hypertension or diabetes was in patients with insomnia who slept ≤5 h [odds ratio (OR) = 5.1 and OR = 2.95, respectively) and the second highest in patients with insomnia who slept 5–6 h (OR = 3.5 and OR = 2.07, respectively), while patients with insomnia who slept ≥6 h were not at significantly increased risk of hypertension or diabetes (OR = 1.3 and OR = 1.1, respectively). Recent longitudinal data from the same cohort have shown that patients with insomnia who slept <6 h were at a significantly higher risk of incident hypertension (OR = 3.75) [71••], suggesting that insomnia precedes the onset of hypertension. Interestingly, in a recent longitudinal study we found that non-obese chronic insomniacs, despite sleeping objectively shorter than controls or poor sleepers, did not have a significantly increased risk of incident obesity; in fact, they were less likely to become obese than controls or poor sleepers [74]. These data indicate that insomnia with objective short sleep duration may be linked to medical morbidity, such as hypertension and diabetes, through mechanisms other than weight gain and obesity (i.e., activation of the stress system and inflammation process). Furthermore, other longitudinal research showed that mortality risk in men was significantly increased in patients with insomnia who slept <6 h compared with normal sleepers (OR = 4.00), and that there was a marginally significant trend toward higher mortality from insomnia with short sleep duration in men with diabetes or hypertension (OR = 7.17) than in those without these comorbid conditions (OR = 1.45). Thus, the impact of insomnia with short sleep duration was much stronger in those with diabetes and hypertension at baseline versus those who were healthy [73]. In women, mortality was not associated with insomnia with short sleep duration, most likely related to the fact that women were followed-up for a shorter time period.
Consistent with the findings of these population-based studies, other recent studies have shown (1) higher night-time systolic blood pressure and reduced day-to-night systolic blood pressure dipping [75]; (2) impaired heart rate variability [76••]; (3) lower cardiac pre-ejection period [77]; and (4) poorer indices of glucose metabolism [78•] in patients with insomnia. Cumulatively, these data suggest that objective short sleep duration may predict the medical severity of chronic insomnia [59••].
Insomnia and Neurocognitive Morbidity
Patients with insomnia typically complain of difficulty concentrating, memory problems, and difficulty focusing attention. However, studies using objective neuropsychological testing have produced inconsistent findings. This has led some researchers to question the existence of true cognitive impairments in insomnia [79] and attribute the daytime complaints to excessive attention to the expected consequences of poor sleep [14].
The role of objective sleep measures in the association of insomnia with cognitive impairment has been addressed in a recent study from the Penn State Adult Cohort [80••]. This study showed that patients with insomnia, based solely on a subjective complaint, did not differ significantly from controls on either PSG variables or neurocognitive performance. However, significant interactions between insomnia and objective short sleep duration (i.e., <6 h) on specific neurocognitive tests were found. Specifically, patients with insomnia with objective short sleep duration showed poorer neuropsychological performance on tests of processing speed, switching attention, and number of short-term visual memory errors and omissions compared with control groups with normal or short sleep duration. In contrast, patients with insomnia with normal sleep duration group showed no significant deficits when compared with controls. Based on these findings, it seems that insomnia with objective short sleep duration is associated with deficits in switching attention, a key component of the “executive control of attention” [80••]. Importantly, the presence of a group of good sleepers with short sleep duration allowed to demonstrate that deficits in executive attention were associated with underlying physiological hyperarousal, a characteristic of chronic insomnia, rather than to short sleep per se [80••]. Another recent study by Edinger et al. [81••] examined the association between physiological hyperarousal, as measured by the MSLT, and response accuracy on reaction time tasks among 89 individuals with primary insomnia compared with 95 well-screened normal sleepers. Interestingly, the authors found that individuals with MSLT mean onset latency >8 mins showed lower night-time sleep efficiencies and increased wake after sleep onset, suggesting 24-h physiological hyperarousal, particularly in the primary insomnia group. Importantly, they found a significant interaction between insomnia and increased MSLT mean onset latency so that individuals with primary insomnia and with MSLT mean onset latency >8 mins showed greater error rates in switching attention tasks than normal sleepers with MSLT mean onset latency >8 mins, who showed no significant deficits. The authors concluded that physiological hyperarousal in insomnia may lead to increased daytime alertness yet dispose these individuals to higher error rates on tasks of switching attention [81••], a finding consistent with those of a study by Fernandez- Mendoza et al. [80••], in which physiological hyperarousal was ascertained by objective short sleep duration.
A recent meta-analysis has shown that individuals with insomnia exhibit performance impairments of small-to-moderate magnitude in several cognitive functions, including working memory, episodic memory, and some aspects of executive functioning [82]. However, an important factor that has been neglected in meta-analytic research of the neurocognitive literature is the role of the degree of objective sleep disturbance in this association. As we have recently reviewed [59••], most studies have shown that cognitive performance is impaired in patients with insomnia with objective sleep disturbances or that it correlates with objective markers of sleep disturbance in patients with insomnia, whereas those studies in which performance was not significantly impaired established insomnia diagnoses using solely subjective criteria [59••].
Cumulatively, the data from these studies indicate that objective short sleep duration may predict its effect on cognitive functions. Future studies should examine whether insomnia with objective short sleep duration may be a premorbid risk factor for mild cognitive impairment and dementia.
Insomnia and Psychiatric Morbidity
Many studies have established that insomnia is highly comorbid with psychiatric disorders and is a risk factor for the development of depression, anxiety, and suicide [83•]. However, the mechanisms by which insomnia precedes the development of psychiatric disorders, for example depression, are unknown. In a recent study from the Penn State Adult Cohort, insomnia with objective short sleep duration was associated with a psychological profile consistent with depressed mood, fatigue, concerns about health and physical functioning, somatically focused anxiety, and poor health status, which is typical of medical outpatients [58]. In contrast, insomnia with normal sleep duration was associated with sleep misperception (i.e., the underestimation of time asleep and overestimation of time awake during the night) and a psychological profile consistent with depressed mood, rumination, anxiety, intrusive thoughts, and poor coping resources [58]. These data have led us to suggest that both insomnia subtypes are associated with (or are at risk of developing) psychiatric disorders, but that different pathophysiological mechanisms may account for such an association [59••]. For example, it is possible that biological mechanisms, that is, hyperactivity of the HPA axis, may play a role in the development of depression in insomniacs with objective short sleep duration, while psychological mechanisms, that is, poor coping resources and ruminative traits, may play such a role in insomniacs with normal sleep duration. However, these hypotheses have yet to be tested.
Natural History of Insomnia: Chronic Insomnia Versus Poor Sleep
As mentioned in the Introduction, about 20 % of the general population has poor sleep (i.e., insomnia symptoms at any given time) and about another 10 % has chronic insomnia. Natural history studies have shown that chronic insomnia is a highly persistent condition, whereas the course of poor sleep is more variable and has a higher remission rate [17, 19, 20••, 84, 85•]. This suggests that insomnia is a disorder, while poor sleep is a symptom of underlying mental and physical health problems [19, 20••, 85•]. Furthermore, objective short sleep duration has been shown to be a risk factor for poor sleep evolving into the more severe form of chronic insomnia [20••], as well as of chronic insomnia becoming persistent [85•]. These latter findings suggest that objective short sleep duration may be a biologic marker of genetic predisposition to chronic insomnia [20••], and of the severity and chronicity of the disorder [85•].
Conclusion
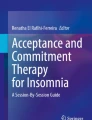
As a result of the above-reviewed literature we have suggested two phenotypes of chronic insomnia. The first phenotype is primarily associated with physiological hyperarousal (i.e., short sleep duration and activation of both limbs of the stress system), significant medical sequelae (e.g., hypertension, diabetes, cognitive impairment, increased mortality), and a persistent course. The second phenotype is associated with cognitive–emotional and cortical arousal, but not with physiological hyperarousal (i.e., normal sleep duration and normal activity of the stress system) or significant medical sequelae, and is more likely to remit over time. Furthermore, the first phenotype is associated with a psychological profile typical of medical outpatients, whereas the second phenotype is associated with sleep misperception, anxious–ruminative traits, and poor coping resources [59••]. Table 1 summarizes the findings of key studies, while Fig. 1 depicts a heuristic model of the underlying pathophysiological mechanisms and clinical characteristics of the two insomnia phenotypes.

Heuristic model of the underlying pathophysiological mechanisms and clinical characteristics of the two insomnia phenotypes based on objective sleep duration. The common characteristics of the two phenotypes are presented in the overlapping area, while their unique characteristics are presented in the areas of each phenotype that do not overlap. Reprinted from Sleep Medicine Reviews, 17(4), Vgontzas AN, Fernandez-Mendoza J, Liao D, Bixler EO [59••], Insomnia with objective short sleep duration: The most biologically severe phenotype of the disorder, 241-54, 2013, with permission from Elsevier
Our proposed model for the two insomnia phenotypes may have an impact on how we diagnose and treat chronic insomnia. As we stated earlier, previously proposed subtypes of insomnia are based on subjective tools such as clinical interviews, questionnaires, and specific scales, and their diagnostic reliability is, at best, modest. The data reviewed here suggest that objective measures of sleep can be useful in detecting the most severe form of insomnia. Thus, we propose the inclusion of objective sleep duration as a criterion in future diagnostic manuals for insomnia in order to differentiate these two clearly different and clinically relevant subtypes of insomnia.
Further, our data suggest that objective measures of sleep, in addition to a thorough clinical evaluation, should become part of the standard diagnostic procedures for insomnia [59••]. Although our studies have focused on the utility of sleep duration, other studies suggest that other variables of sleep efficiency and continuity or of physiological hyperarousal (i.e., MSLT) may also serve as markers of the biological severity of the disorder [20••, 26, 81••, 86–88]. However, a potential disadvantage of biomarkers such as stage 1, slow wave sleep (SWS), or MSLT is that they require a full PSG study or daytime laboratory assessment, whereas sleep duration perhaps could be obtained with simpler methods, for example actigraphy. In this regard, several studies suggest the potential usefulness of actigraphy to assess sleep patterns for a period of days or weeks in the “habitual home environment”, to characterize the severity of the insomnia disorder [88]. A similar amount of home sleep monitoring with PSG would be difficult and impractical for clinical venues. However, several problems associated with the use of actigraphy, such as lack of an industry standard for the sleep algorithms used in different actigraphic devices and the propensity to over- or underestimate sleep time, make its current use limited. Future studies using cost-effective methods should examine which variables, that is, sleep duration versus night-to-night variability, and which methods, that is, actigraphy, salivary cortisol, and peripheral measures of sympathetic activation, are better predictors of cardiometabolic and neurocognitive morbidity.
Finally, our findings may affect the way we treat chronic insomnia. The insomnia phenotype with short sleep duration may respond better to treatments that primarily aim at decreasing physiological hyperarousal and increasing sleep duration, such as medication or other biological treatments [30]. Previous studies have shown that sedative antidepressants such as trazodone or doxepin, used at low dosages, down-regulate the activity of the HPA axis, decrease cortisol levels, and increase sleep duration [30, 89, 90]. Needless to say that biological treatments should be part of a multidimensional approach that combines behavioral changes, that is, sleep hygiene, and psychological interventions, for example cognitive–behavioral therapy (CBT), when indicated. The second phenotype, that is, insomnia with normal sleep duration, may respond better to treatments that primarily aim at decreasing cognitive–emotional arousal, changing sleep-related beliefs and behaviors, and altering sleep misperception, such as CBT [91]. Psychotherapeutic medication may be indicated based on the presence of comorbid psychiatric conditions, that is, anxiety or depressive disorders. The differential treatment response of these two phenotypes should be tested in future placebo-controlled clinical trials. In any event, the treatment of insomnia with objective short sleep duration should become a priority given its severity and its effects on physical health. Finally, in the prevention of chronic insomnia, our strategies should focus on (1) those with premorbid cognitive–emotional hyperarousal and short sleep duration, (2) stress-related poor sleep with short objective sleep duration, and (3) a family history of sleep problems [18, 19, 20••].
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Bixler EO, Vgontzas AN, Lin HM, Vela-Bueno A, Kales A. Insomnia in central Pennsylvania. J Psychosom Res. 2002;53:589–92.
Ohayon MM. Epidemiology of insomnia: what we know and what we still need to learn. Sleep Med Rev. 2002;6:97–111.
Chong Y, Fryar CD, Gu Q. Prescription sleep aid use among adults: United States, 2005–2010. NCHS data brief, no 127. Hyattsville, MD: National Center for Health Statistics; 2013.
Reynolds 3rd CF, Kupfer DJ, Buysse DJ, Coble PA, Yeager A. Subtyping DSM-III-R primary insomnia: a literature review by the DSM-IV Work Group on Sleep Disorders. Am J Psychiatry. 1991;148:432–8.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders, text revision. 4th ed. Washington, DC: American Psychiatric Association; 2000.
American Psychiatric Association. Diagnostic and statistical manual of mental disorders. 5th ed. Washington, DC: American Psychiatric Press; 2013.
American Academy of Sleep Medicine. The International Classification of Sleep Disorders (ICSD-2): diagnostic and coding manual. 2nd ed. Westchester: American Academy of Sleep Medicine; 2005.
Edinger JD, Wyatt JK, Stepanski EJ, Olsen MK, Stechuchak KM, Carney CE, et al. Testing the reliability and validity of DSM-IV-TR and ICSD-2 insomnia diagnoses. Results of a multitrait-multimethod analysis. Arch Gen Psychiatry. 2011;68:992–1002. This multi-site study found that current insomnia nosologies have low validity.
Vgontzas AN, Kales A. Sleep and its disorders. Annu Rev Med. 1999;50:387–400.
Vgontzas AN, Bixler EO, Kales A, Criley C, Vela-Bueno A. Differences in nocturnal and daytime sleep between primary and psychiatric hypersomnia: diagnostic and treatment implications. Psychosom Med. 2000;62:220–6.
Vgontzas AN, Bixler EO, Kales A, Manfredi RL, Tyson K. Validity and clinical utility of sleep laboratory criteria for insomnia. Int J Neurosci. 1994;77:11–21.
Vgontzas AN, Kales A, Bixler EO, Manfredi RL, Vela-Bueno A. Usefulness of polysomnographic studies in the differential diagnosis of insomnia. Int J Neurosci. 1995;82:47–60.
Littner M, Hirshkowitz M, Kramer M, Kapen S, Anderson WM, Bailey D, et al. Practice parameters for using polysomnography to evaluate insomnia: an update. Sleep. 2003;26:754–60.
Kales A, Kales JD. Evaluation and treatment of insomnia. New York: Oxford University Press; 1984.
LeBlanc M, Beaulieu-Bonneau S, Merette C, Savard J, Ivers H, Morin CM. Psychological and health-related quality of life factors associated with insomnia in a population-based sample. J Psychosom Res. 2007;63:157–66.
Morin CM, Rodrigue S, Ivers H. Role of stress, arousal, and coping skills in primary insomnia. Psychosom Med. 2003;65:259–67.
LeBlanc M, Mérette C, Savard J, Ivers H, Baillargeon L, Morin CM. Incidence and risk factors of insomnia in a population-based sample. Sleep. 2009;32:1027–37.
Fernández-Mendoza J, Vela-Bueno A, Vgontzas AN, Ramos-Platón MJ, Olavarrieta-Bernardino S, Bixler EO, et al. Cognitive-emotional hyperarousal as a premorbid characteristic of individuals vulnerable to insomnia. Psychosom Med. 2010;72:397–403.
Singareddy R, Vgontzas AN, Fernandez-Mendoza J, Liao D, Calhoun S, Shaffer ML, et al. Risk factors for incident chronic insomnia: a general population prospective study. Sleep Med. 2012;13:346–53.
Fernandez-Mendoza J, Vgontzas AN, Bixler EO, Singareddy R, Shaffer ML, Calhoun SL, et al. Clinical and polysomnographic predictors of the natural history of poor sleep in the general population. Sleep. 2012;35:689–97. This prospective cohort study found that objective short sleep duration, mental health problems, and familial history of insomnia predict incident insomnia in poor sleepers.
Healey ES, Kales A, Monroe LJ, Bixler EO, Chamberlin K, Soldatos CR. Onset of insomnia: role of life-stress events. Psychosom Med. 1981;43:439–51.
Monroe LJ. Psychological and physiological differences between good and poor sleepers. J Abnorm Psychol. 1967;72:255–64.
Johns MW, Gay TJA, Masterton JP, Bruce DW. Relationship between habits, adrenocortical activity and personality. Psychosom Med. 1971;33:499–508.
Frankel BL, Buchbinder R, Coursey R, Snyder F. Sleep patterns and psychological test characteristics of chronic primary insomniacs. Sleep Res. 1973;2:149.
Adam K, Tomeny M, Oswald I. Physiological and psychological differences between good and poor sleepers. J Psychiatr Res. 1986;20:301–16.
Vgontzas AN, Tsigos C, Bixler EO, Stratakis CA, Zachman K, Kales A, et al. Chronic insomnia and activity of the stress system: a preliminary study. J Psychosom Res. 1998;45:21–31.
Vgontzas AN, Bixler EO, Lin HM, Prolo P, Mastorakos G, Vela-Bueno A, et al. Chronic insomnia is associated with nyctohemeral activation of the hypothalamic-pituitary-adrenal axis: clinical implications. J Clin Endocrinol Metab. 2001;86:3787–94.
Rodenbeck A, Huether G, Ruether E, Hajak G. Interactions between evening and nocturnal cortisol secretion and sleep parameters in patients with severe chronic primary insomnia. Neurosci Lett. 2002;324:159–63.
Shaver JL, Johnston SK, Lentz MJ, Landis CA. Stress exposure, psychological distress, and physiological stress activation in midlife women with insomnia. Psychosom Med. 2002;64:793–802.
Rodenbeck A, Cohrs S, Jordan W, Huether G, Rüther E, Hajak G. The sleep-improving effects of doxepin are paralleled by a normalized plasma cortisol secretion in primary insomnia. A placebo-controlled, double-blind, randomized, cross-over study followed by an open treatment over 3 weeks. Psychopharmacology (Berl). 2003;170:423–8.
Irwin M, Clark C, Kennedy B, Christian Gillin J, Ziegler M. Nocturnal catecholamines and immune function in insomniacs, depressed patients, and controls subjects. Brain Behav Immun. 2003;17:365–72.
Riemann D, Klein T, Rodenbeck A, Feige B, Horney A, Hummel R, et al. Nocturnal cortisol and melatonin secretion in primary insomnia. Psychiatry Res. 2002;113:17–27.
Varkevisser M, Van Dongen HP, Kerkhof GA. Physiologic indexes in chronic insomnia during a constant routine: evidence for general hyperarousal? Sleep. 2005;28:1588–96.
Bonnet MH. Hyperarousal as the basis for insomnia: effect size and significance. Sleep. 2005;28:1500–1.
Vgontzas AN, Bixler EO, Wittman AM, Zachman K, Lin HM, Vela-Bueno A, et al. Middle-aged men show higher sensitivity of sleep to the arousing effects of corticotropin-releasing hormone than young men: clinical implications. J Clin Endocrinol Metab. 2001;86:1489–95.
Stepanski E, Glinn M, Zorick F, Roehrs T, Roth T. Heart rate changes in chronic insomnia. Stress Med. 1994;10:261–6.
Bonnet MH, Arand DL. Heart rate variability in insomniacs and matched normal sleepers. Psychosom Med. 1998;60:610–5.
Bonnet MH, Arand DL. 24-hour metabolic rate in insomniacs and matched normal sleepers. Sleep. 1995;18:581–8.
Bonnet MH, Arand DL. Physiological activation in patients with sleep state misperception. Psychosom Med. 1997;59:533–40.
Lichstein K, Johnson RS. Pupillometric discrimination of insomniacs. Behav Res Ther. 1994;32:123–9.
Lichstein KL, Johnson RS, Sen Gupta S, O’Laughlin DL, Dykstra TA. Are insomniacs sleepy during the day? A pupillometric assessment. Behav Res Ther. 1992;30:283–92.
Lichstein KL, Wilson NM, Noe SL, Aguillard RN, Bellur SN. Daytime sleepiness in insomnia: behavioral, biological and subjective indices. Sleep. 1994;17:693–702.
Seidel WF, Ball S, Cohen S, Patterson N, Yost D, Dement WC. Daytime alertness in relation to mood, performance, and nocturnal sleep in chronic insomniacs and noncomplaining sleepers. Sleep. 1984;7:230–8.
Stepanski E, Zorick F, Roehrs T, Young D, Roth T. Daytime alertness in patients with chronic insomnia compared with asymptomatic control subjects. Sleep. 1988;11:54–60.
Bonnet MH, Arand DL. Activity, arousal, and the MSLT in patients with insomnia. Sleep. 2000;23:205–12.
Sugerman JL, Stern JA, Walsh JK. Daytime alertness in subjective and objective insomnia: some preliminary findings. Biol Psychiatry. 1985;20:741–50.
Dorsey CM, Bootzin RR. Subjective and psychophysiologic insomnia: an examination of sleep tendency and personality. Biol Psychiatry. 1997;41:209–16.
Roehrs TA, Randall S, Harris E, Maan R, Roth T. MSLT in primary insomnia: stability and relation to nocturnal sleep. Sleep. 2011;34:1647–52.
Bonnet MH, Arand DL. Clinical effects of sleep fragmentation versus sleep deprivation. Sleep Med Rev. 2003;7:297–310.
Vgontzas AN, Zoumakis E, Bixler EO, Lin HM, Follett H, Kales A, et al. Adverse effects of modest sleep restriction on sleepiness, performance, and inflammatory cytokines. J Clin Endocrinol Metab. 2004;89:2119–26.
Nofzinger EA, Nissen C, Germain A, Moul D, Hall M, Price JC, et al. Regional cerebral metabolic correlates of WASO during NREM sleep in insomnia. J Clin Sleep Med. 2006;2:316–22.
Winkelman JW, Buxton OM, Jensen JE, Benson KL, O’Connor SP, Wang W, et al. Reduced brain GABA in primary insomnia: preliminary data from 4T proton magnetic resonance spectroscopy (1H-MRS). Sleep. 2008;311:1499–506.
Krystal AD, Edinger JD, Wohlgemuth WK, Marsh GR. NREM sleep EEG frequency spectral correlates of sleep complaints in primary insomnia subtypes. Sleep. 2002;25:630–40.
Corsi-Cabrera M, Figueredo-Rodríguez P, del Río-Portilla Y, Sánchez-Romero J, Galán L, Bosch-Bayard J. Enhanced frontoparietal synchronized activation during the wake-sleep transition in patients with primary insomnia. Sleep. 2012;35:501–11.
Parrino L, Milioli G, De Paolis F, Grassi A, Terzano MG. Paradoxical insomnia: the role of CAP and arousals in sleep misperception. Sleep Med. 2009;10:1139–45.
Bastien CH, Turcotte I, St-Jean G, Morin CM, Carrier J. Information processing varies between insomnia types: measures of N1 and P2 during the night. Behav Sleep Med. 2013;11:56–72.
Cano G, Mochizuki T, Saper CB. Neural circuitry of stress-induced insomnia in rats. J Neurosci. 2008;28:10167–84.
Fernandez-Mendoza J, Calhoun SL, Bixler EO, Karataraki M, Liao D, Vela-Bueno A, et al. Sleep misperception and chronic insomnia in the general population: role of objective sleep duration and psychological profiles. Psychosom Med. 2011;73:88–97.
Vgontzas AN, Fernandez-Mendoza J, Liao D, Bixler EO. Insomnia with objective short sleep duration: the most biologically severe phenotype of the disorder. Sleep Med Rev. 2013;17:241–54. This article comprehensively reviews the association of insomnia with objective short sleep duration with physiological hyperarousal, medical morbidity, and mortality.
Bonnet MH, Arand DL. Cardiovascular implications of poor sleep. Sleep Med Clin. 2007;2:529–38.
Suka M, Yoshida K, Sugimori H. Persistent insomnia is a predictor of hypertension in Japanese male workers. J Occup Health. 2003;45:344–50.
Laugsand LE, Vatten LJ, Platou C, Janszky I. Insomnia and the risk of acute myocardial infarction: a population study. Circulation. 2011;124:2073–81.
Kawakami N, Takatsuka N, Shimizu H. Sleep disturbance and onset of type 2 diabetes. Diabetes Care. 2004;27:282–3.
Nilsson PM, Rööst M, Engström G, Hedblad B, Berglund G. Incidence of diabetes in middle-aged men is related to sleep disturbances. Diabetes Care. 2004;27:2464–9.
Meisinger C, Heier M, Loewel H, MONICA/KORA Augsburg Cohort Study. Sleep disturbance as a predictor of type 2 diabetes mellitus in men and women from the general population. Diabetologia. 2005;48:235–41.
Mallon L, Broman JE, Hetta J. High incidence of diabetes in men with sleep complaints or short sleep duration: a 12-year follow-up study of a middle-aged population. Diabetes Care. 2005;28:2762–7.
Phillips B, Mannino DM. Do insomnia complaints cause hypertension or cardiovascular disease? J Clin Sleep Med. 2007;3:489–94.
Bonnet MH. Evidence for the pathophysiology of insomnia. Sleep. 2009;32:441–2.
Kripke DF, Garfinkel L, Wingard DL, Klauber MR, Marler MR. Mortality associated with sleep duration and insomnia. Arch Gen Psychiatry. 2002;59:131–6.
Vgontzas AN, Liao D, Bixler EO, Chrousos GP, Vela-Bueno A. Insomnia with objective short sleep duration is associated with a high risk for hypertension. Sleep. 2009;32:491–7. This was the first cohort study to show an association of insomnia with objective short sleep duration with significant medical morbidity, that is, hypertension.
Fernandez-Mendoza J, Vgontzas AN, Liao D, Shaffer ML, Vela-Bueno A, Basta M, et al. Insomnia with objective short sleep duration and incident hypertension: the Penn State Cohort. Hypertension. 2012;60:929–35. This prospective cohort study confirmed the longitudinal association of insomnia with objective short sleep duration with hypertension.
Vgontzas AN, Liao D, Pejovic S, Calhoun S, Karataraki M, Bixler EO. Insomnia with objective short sleep duration is associated with type 2 diabetes: A population-based study. Diabetes Care. 2009;32:1980–5. This cohort study showed an association of insomnia with objective short sleep duration with increased risk of diabetes.
Vgontzas AN, Liao D, Pejovic S, Calhoun S, Karataraki M, Basta M, et al. Insomnia with short sleep duration and mortality: the Penn State cohort. Sleep. 2010;33:1159–64.
Vgontzas AN, Fernandez-Mendoza J, Miksiewicz T, Kritikou I, Shaffer ML, Liao D, et al. Unveiling the longitudinal association between short sleep duration and the incidence of obesity: the Penn State cohort. Int J Obes (Lond). 2013. doi:10.1038/ijo.2013.172.
Lanfranchi PA, Pennestri MH, Fradette L, Dumont M, Morin CM, Montplaisir J. Nighttime blood pressure in normotensive subjects with chronic insomnia: implications for cardiovascular risk. Sleep. 2009;32:760–6.
Spiegelhalder K, Fuchs L, Ladwig J, Kyle SD, Nissen C, Voderholzer U, et al. Heart rate and heart rate variability in subjectively reported insomnia. J Sleep Res. 2011;20:137–45. This study showed that impaired heart rate variability was present in insomniacs with objective short sleep duration.
De Zambotti M, Covassin N, De Min TG, Sarlo M, Stegagno L. Sleep onset and cardiovascular activity in primary insomnia. J Sleep Res. 2011;20:318–25.
Knutson KL, Van Cauter E, Zee P, Liu K, Lauderdale DS. Cross-sectional associations between measures of sleep and markers of glucose metabolism among subjects with and without diabetes: the Coronary Artery Risk Development in Young Adults (CARDIA) Sleep Study. Diabetes Care. 2011;34:1171–6. This cohort study showed that markers of glucose metabolism were poorest in insomniacs with objective short sleep duration.
Riedel BW, Lichstein KL. Insomnia and daytime functioning. Sleep Med Rev. 2000;4:277–98.
Fernandez-Mendoza J, Calhoun S, Bixler EO, Pejovic S, Karataraki M, Liao D, et al. Insomnia with objective short sleep duration is associated with deficits in neuropsychological performance: a general population study. Sleep. 2010;33:459–65. This cohort study showed an association of insomnia with objective short sleep duration with significant neurocognitive impairment.
Edinger JD, Means MK, Krystal AS. Does physiological hyperarousal enhance error rates among patients with insomnia? Sleep. 2013;36:1179–86. This cohort study showed an association of insomnia with physiological hyperarousal with significant neurocognitive impairment.
Fortier-Brochu E, Beaulieu-Bonneau S, Ivers H, Morin CM. Insomnia and daytime cognitive performance: a meta-analysis. Sleep Med Rev. 2012;16:83–94.
Baglioni C, Battagliese G, Feige B, Spiegelhalder K, Nissen C, Voderholzer U, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affect Disord. 2011;135:10–9. This meta-analysis showed that insomnia is a significant predictor of incident depression.
Morin CM, Bélanger L, LeBlanc M, Ivers H, Savard J, Espie CA, et al. The natural history of insomnia: a population-based 3-year longitudinal study. Arch Intern Med. 2009;169:447–53.
Vgontzas AN, Fernandez-Mendoza J, Bixler EO, Singareddy R, Shaffer ML, Calhoun SL, et al. Persistent insomnia: the role of objective short sleep duration and mental health. Sleep. 2012;35:61–8. This cohort study showed that objective short sleep duration and mental health problems predict the persistence of insomnia.
Edinger JD, Means MK, Carney CE, Krystal AD. Psychomotor performance deficits and their relation to prior nights’ sleep among individuals with primary insomnia. Sleep. 2008;31:599–607.
Fung MM, Peters K, Redline S, Ziegler MG, Ancoli-Israel S, Barrett-Connor E, et al. Decreased slow wave sleep increases risk of developing hypertension in elderly men. Hypertension. 2011;58:596–603.
Sánchez-Ortuño MM, Edinger JD, Means MK, Almirall D. Home is where sleep is: an ecological approach to test the validity of actigraphy for the assessment of insomnia. J Clin Sleep Med. 2010;6:21–9.
Deuschle M, Schmider J, Weber B, Standhardt H, Körner A, Lammers CH, et al. Pulse-dosing and conventional application of doxepin: effects on psychopathology and hypothalamus-pituitary-adrenal (HPA) system. J Clin Psychopharmacol. 1997;17:156–60.
Monteleone P. Effects of trazodone on plasma cortisol in normal subjects. A study with drug plasma levels. Neuropsychopharmacology. 1991;5:61–4.
Edinger JD, Wohlgemuth WK, Radtke RA, Marsh GR, Quillian RE. Cognitive behavioral therapy for treatment of chronic primary insomnia: a randomized controlled trial. JAMA. 2001;285:1856–64.
Edinger JD, Fins AI, Glenn DM, Sullivan Jr RJ, Bastian LA, Marsh GR, et al. Insomnia and the eye of the beholder: are there clinical markers of objective sleep disturbances among adults with and without insomnia complaints? J Consult Clin Psychol. 2000;68:586–93.
Acknowledgment
This paper was supported by National Institutes of Health grants R01 51931, R01 33 40916, and R01 64415 to Alexandros N. Vgontzas.
Compliance with Ethics Guidelines
ᅟ
Conflict of Interest
Julio Fernandez-Mendoza and Alexandros N. Vgontzas declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Sleep Disorders
Rights and permissions
About this article
Cite this article
Fernandez-Mendoza, J., Vgontzas, A.N. Insomnia and its Impact on Physical and Mental Health. Curr Psychiatry Rep 15, 418 (2013). https://doi.org/10.1007/s11920-013-0418-8
Published:
DOI: https://doi.org/10.1007/s11920-013-0418-8