
Abstract
This article reviews the most recent studies of the pharmacologic treatment of borderline personality disorder (BPD). Although research continues using randomized controlled trials with a placebo arm as well as active medication, meta-analyses and systematic reviews have revealed that the use of any specific medication or medication class in BPD remains at best uncertain and inconclusive. Studies indicate that the selective serotonin reuptake inhibitors have fallen out of favor, and researchers have turned their attention to the study of mood stabilizers and atypical antipsychotics. Thus, it is not surprising that trends in prescribing appear to be shifting toward the use of these two classes over the selective serotonin reuptake inhibitors; yet we remain without any medication that has a specific indication for treatment of BPD or an indication for any symptom that is seen as part of the BPD syndrome.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Although pharmacologic treatment of borderline personality disorder (BPD) has been a researched topic for more than 30 years [1], the actual effectiveness data that we have available remain skimpy. At the present time, the study of BPD with pharmacologic agents is really just beginning. No medications have received a US Food and Drug Administration indication for the treatment of the disorder in the United States, and there is no approved medication in the United Kingdom or European Union. Thus, whenever medications are used in BPD, they are considered off label except perhaps when they are being used to treat an Axis I comorbidity accompanying the Axis II BPD.
Nonetheless, medications are used frequently in patients with BPD [2–4], particularly in attempts to reduce some of the disruptive symptoms that present clinically. The reduction of these symptoms—often seen as key features of the clinical picture—is the primary goal of pharmacotherapy, but such symptom reduction in response to pharmacotherapy remains modest [5••]. No medication is thought to treat the syndrome of BPD itself [6••]. Rather, we are left trying to impact specific symptoms or behaviors that are part of the overall BPD syndromic presentation. Nonetheless, a body of evidence continues to accumulate in support of the idea that medications can be safely used with some improvements in specific aspects of the anxiety, self-destruction, agitation, cognitive distortions, and mood components that typify the illness. A substantial number of randomized, placebo-controlled trials (RCTs), open-label studies, and meta-analyses on the topic continue to be published. Despite these accumulating data, however, medications are still viewed as adjunctive to other forms of treatment of BPD, particularly psychotherapy [6••, 7].
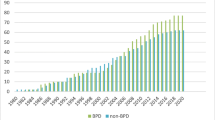
This article explores and summarizes the past 5 years of literature on the topic. Although we concentrate on the past 2 years of published studies, we choose the past 5 years overall because it has been during that time that a shift has occurred in the classes of pharmacologic agents studied in BPD, from the selective serotonin reuptake inhibitors (SSRIs) to the atypical antipsychotics and mood stabilizers. Looking at only the past few years then will, we think, fail to convey an appreciation of how this shift influences the pharmacologic choices that clinicians are currently making.
Randomized Controlled Trials
We identified eight RCTs in this period [8•, 9•, 10, 11•, 12, 13•–15•]. Four involved atypical antipsychotic medications (olanzapine and ziprasidone), three investigated mood stabilizers (topiramate and lamotrigine), one used haloperidol as a comparator to olanzapine [10], and one looked at the α-blocking agent clonidine, a class that had not been studied in BPD previously.
Olanzapine was investigated in three trials. Two studies found no significant difference from placebo, while a third, which compared olanzapine with haloperidol, found an equally positive response to both. In a multicenter, 12-week study of 314 people with BPD (70% women) conducted by Schulz et al. [8•], olanzapine (2.5–20 mg) and placebo resulted in significant—but not differentiable—improvements on the Zanarini Rating Scale for BPD [16]. This similar improvement between active medication and placebo may be thought to reflect nonspecific, immediate improvements often seen clinically in this population in response to treatment novelty, or to the attention paid to participants in a controlled trial. This may then represent placebo or psychological responses rather than medication-specific effects. Linehan et al. [9•] compared olanzapine with placebo in 24 women with BPD who were also receiving 6 months of dialectical behavioral therapy. All the participants showed improvement in irritability, aggression, self-injury, and depression. Those who received olanzapine tended to improve more quickly than those who received placebo, but this was not statistically significant (P = 0.1). However, Shafti and Shahveisi [10] found no difference in efficacy between olanzapine and haloperidol on the Brief Psychiatric Rating Scale. Both groups showed significant improvement compared with baseline measurements, but the study did not have a placebo control arm and thus could not differentiate between medication-specific and nonspecific results. A similar study involving a 12-week, double-blind trial of ziprasidone in 60 patients with BPD [11•] found no statistically significant difference compared with placebo on the Clinical Global Impression Scale for use in BPD [17] or its subscales.
The mood stabilizers topiramate and lamotrigine also underwent clinical trials in BPD patients. Fifty-six women with BPD were evenly divided between a topiramate and placebo arm in a 12-week RCT [12]. Significant improvements were found on intent-to-treat analysis of somatization, hostility, anxiety, interpersonal sensitivity, and interpersonal functioning as measured by the Symptom Checklist, the Medical Outcomes Survey Short Form 36, and the Inventory of Interpersonal Problems. Another topiramate study in a group of 44 aggressive male patients with BPD found that after 18 months, they continued to show significant reductions on the State-Trait Anger Expression Inventory. Furthermore, the 22 patients who had originally been in the placebo group showed benefits similar to those of the initial treatment group when switched to the treatment arm [13•]. An additional benefit was mild, sustained weight loss. Reich et al. [14•] showed that lamotrigine was superior to placebo in decreasing affective lability and instability in a double-blind study with a group of 28 (13 placebo) BPD patients.
α-Blockade had not specifically been studied in BPD. However, it has been helpful with hyperarousal (insomnia, irritability, agitation, hypervigilance) in post-traumatic stress disorder (PTSD) [15•]. Many of these symptoms are found in BPD as well, and PTSD itself is highly comorbid in BPD [15•]. In a small study, 18 patients with BPD (17 women) and high hyperarousal scores were treated with 0.15 mg of clonidine in the morning and 0.3 mg at night. Twelve of these patients also had formal PTSD diagnoses. The study showed significant improvement in the Clinician Administered PTSD Scale in those who also had PTSD, and a nonsignificant improvement in those who did not. Sleep also improved significantly in the PTSD group, although minimally, with a mean reduction in sleep latency of 17 min. Both groups reported feeling subjectively more refreshed but did not report improvements in mood. The Symptom Checklist-90-Revised showed no overall improvement in pathology but did show significant improvement in anxiety. However, again, when the patients were subdivided into PTSD-positive and PTSD-negative subgroups, the PTSD-negative patients did not achieve significant results compared with placebo [15•]. The study was limited by its small number of participants, low power, and 30% attrition rate, along with some suspicion that adverse events unblinded some patients in the clonidine group. The authors concluded that although the non-PTSD group did show “trend level improvement,” statistically significant benefit was seen only in the comorbid PTSD patients. This then leads one to question whether the study reflected a BPD treatment or, perhaps more accurately, showed that results similar to those involving α-blockade in other PTSD populations could be reproduced in patients with comorbid BPD.
Open-Label Trials
Four open-label, noncontrolled trials investigated the efficacy of quetiapine in BPD [18–21]. Completer size for the smallest study was 9, followed by 11, 23, and 31 participants in the other studies. All were brief (8–12 weeks). The dose range in three of the trials was similar and ranged roughly from 200 to 400 mg [18–20], while the van den Eynde et al. [21] study reported a range of 100 to 800 mg. All the studies looked at multiple domains of BPD pathology and overall function. All reported improvement in impulsivity, hostility, anger, and overall functioning. Three of the four studies also found significant improvements in depression and general anxiety. Bellino et al. [19] found no significant change in depression, while Adityanjee et al. [20] detected no difference in anxiety on the Symptom Checklist-90. Only two [18, 20] of the three articles [18–20] that specifically measured paranoia and psychotic symptoms reported significant benefit.
However, all these studies must be viewed with caution because of the large placebo effect frequently seen in the BPD population, including trials of other antipsychotics such as olanzapine and ziprasidone. It is not certain that the benefits reported in these trials are medication specific. The potential large placebo response seen in this population raises the question of the utility of open-label trials in BPD. Seemingly positive results may lead clinicians to erroneously attribute efficacy to specific pharmacotherapies that may not outperform the placebo in rigorous studies involving a placebo [22].
Two studies by Bellino et al. [23, 24•] compared fluoxetine monotherapy (20–40 mg) with fluoxetine and interpersonal therapy (IPT) in the treatment of depression in BPD patients. The first study measured 32 completers at 12 and 24 weeks [23]. Although self-reported social functioning was improved in the IPT group compared with the fluoxetine-alone group, other measures were not significant for either group. A statistically significant improvement was noted on the Hamilton Depression Rating Scale (HAM-D) with combined therapy compared with pharmacotherapy alone, but when compared with improvements both groups made as a factor of time, the HAM-D improvement was not found to be significant and is of questionable clinical relevance given the small effect size. The second study, conducted by the same group, attempted to compare fluoxetine with IPT adapted specifically for BPD patients (IPT-BPD) [24•]. Forty-four completers were assessed at 16 and 32 weeks. Duration of treatment rather than treatment type was found to be the single most important factor for improvement, once again suggesting that nonspecific treatment effects may account for much of the benefit BPD patients derive from many therapies [22]. Combined pharmacotherapy and psychotherapy again proved more effective than pharmacotherapy alone for social functioning, but this is also limited by the lack of comparison to IPT (or IPT-BPD) alone or to a sham therapy group.
The same group also published an open-label trial of duloxetine in BPD, which had not been studied previously [25]. They found significant improvements in the BPD Severity Index [26] total score and the subsections for impulsivity, affective lability, and outbursts of anger. Depressive symptoms also showed significant benefit, as did social and occupational functioning and somatization metrics. Again, no placebo control was used, raising the possibility that these were medication-nonspecific effects.
Finally, Miyaoka et al. [27] investigated Yi-gan san, a Chinese medication developed in 1555 as a treatment of restlessness and agitation in children. The study chose 20 women with a history of noncompliance and being difficult to treat, who underwent a washout from all other medications before being given 1.5 g of Yi-gan san extract one to three times daily. This was provided as monotherapy, and no other psychiatric treatment (pharmacotherapy or psychotherapy) was provided or allowed. It is unclear how the dosing schedule was determined in a given individual. Participants were assessed on intake and at weeks 2 and 12. The authors found significant improvement in measurements of depression, anxiety, somatic concerns, hostility, aggression, suspicion, cooperativeness, and global function, but there was no placebo control. The study showed that all the benefit was achieved in the first 2 weeks and remained significant at week 12. The rapidity of this widespread benefit and the participants’ likely perceived novelty of this “natural” treatment make the comparison to placebo an especially relevant question in this group.
Meta-Analyses and Systematic Reviews
Several meta-analyses have examined RCTs aimed at BPD specifically or wherein BPD is considered as part of an examination of the pharmacologic treatment of personality disorders [5••, 28, 29••, 30–32, 33••, 34, 35•, 36•, 37]. The most rigorous of these was the 2010 update by Stoffers et al. [5••] of the Cochrane review on the topic (first published in a shortened version by Binks et al. [28] in 2006). A version was also published in the British Journal of Psychiatry by Lieb et al. [29••]. They noted, as mentioned above, that no treatments seem to modify the core pathology of BPD. Pharmacotherapy provides symptomatic improvement in some cases and domains. After examining data from 27 trials, Stoffers et al. [5••] concluded that SSRI therapy (and tricyclic antidepressant therapy, although there were fewer trials) showed the least benefit in BPD. Specifically, SSRIs showed no benefit for the lability, dysphoria, anger, impulsivity, or suicidal behaviors that form the core and most problematic elements of BPD. When Abraham and Calabrese [30] performed their own (not a meta-analysis) examination of 28 RCTs, they commented similarly that a shift away from studies of SSRIs toward mood stabilizers and antipsychotics had occurred in the literature and probably in practice as well [3]. This contradicts the findings of Nosè et al. [31], whose 2006 meta-analysis suggested that antidepressants could be helpful for affective instability and anger.
Similar findings can be found in the NICE Guidelines on Borderline Personality Disorder from the United Kingdom National Institute for Health and Clinical Excellence’s Guidance documents. Although it is not a formal meta-analysis, this thorough review of the treatment of BPD includes conclusions regarding psychopharmacology [6••]. On page 21 of that guideline (number 78), on which the drug treatment recommendations are summarized, the guideline concludes that, “Drug treatment should not be used specifically for borderline personality disorder or for the individual symptoms or behaviour associated with the disorder (for example, repeated self-harm, marked emotional instability, risk-taking behaviour and transient psychotic symptoms).” Although the NICE Guidelines do not argue against any use of psychopharmacologic agents in BPD, they suggest the following if medications are to be considered: 1) that antipsychotic medication be used only over the short term and not for medium- or long-term treatment; 2) that perhaps psychopharmacologic treatment has a role in the overall treatment of comorbid conditions; 3) that perhaps sedative medications might be considered in the short-term treatment of BPD patients in crisis, but not for longer than 1 week; 4) that the patient with BPD should be provided with written material with respect to the specific drug being suggested, and that the effectiveness and adverse effects of the drug in patients with or without BPD be clearly explained; and 5) that if one has a BPD patient without comorbid conditions, every effort should be made to reduce or stop the pharmacotherapy [6••].
The consensus from reviews and meta-analyses seems to favor mood stabilizers, particularly topiramate, lamotrigine, and perhaps valproate (which, although showing some benefit, has been included only in small studies), but not carbamazepine, which yielded mixed results. Individuals showed improvement in anger, impulsivity, and mood with use of these mood stabilizers [5••, 30, 35•].
The atypical antipsychotic medications aripiprazole and olanzapine also showed benefit in these reviews [5, 29••, 30, 37, 38]; however, as noted above, more recent trials involving olanzapine (including by far the largest to date, with 314 completers) showed no significant difference compared with placebo. Aripiprazole has not been included in further trials as a single agent currently. The first-generation antipsychotics haloperidol and less so fluphenazine were found to have benefits, with the former reducing anger and the latter reducing suicidal behavior [29••].
However, all these meta-analyses suffered from significant limitations. As discussed by Lieb et al. [29••], the studies often used disparate outcome measures, and many of those measures were performed before the development of scales specific to BPD. This hindered the ability to pool the small samples, which has been a major limitation of BPD pharmacologic research to date. Furthermore, Lieb et al. [29••] questioned the generalizability of these studies, most or all of which excluded actively suicidal patients; those with comorbid substance misuse or comorbid PTSD; and, in some cases, other Axis I mood disorders—disorders that are quite common if not ubiquitous in the clinical BPD population. They estimated the BPD severity of most patients to be mild to moderate, creating a selection bias that may tend to favor positive results. They also noted a lack of negative results and incomplete or inconsistent use of outcome measures [37, 39]. Moreover, all these studies looked at monotherapy, whereas polypharmacy tends to be common in BPD, again casting some doubt on their generalizability and applicability to how psychopharmacology is practiced in actual clinical settings.
Discussion and Conclusions
Pharmacologic treatment of BPD remains preliminary despite expanding data indicating that medications can provide symptomatic relief. These data are limited by the small size of the trials, inconsistent outcome measures, and enrollment bias that tends to include mildly to moderately ill patients and exclude the more severely affected, who often are the most demanding (both in the patients’ demeanor, with their frequent help seeking, suicide attempts, and inappropriate anger, as well as in our wish to relieve their intolerable pain) [40]. Trials that are not placebo controlled are particularly at risk of misinterpretation when investigating a disorder characterized by internal states that are evanescent and highly reactive to environmental factors.
What can be said with some confidence is that SSRIs, historically considered the first-line treatment of BPD, have not stood the test of time and further study [33••, 41]. On the whole, they appear to be the least effective group of medications among those studied. The mood stabilizers topiramate and lamotrigine have the best evidence for initial treatment in this population, followed less convincingly by antipsychotics. However, when peri- or transient psychotic symptoms or paranoia dominate the clinical picture, antipsychotic medication should be considered first line [38]. The first study to look at α-blockade revealed that clonidine does not specifically help BPD but does improve the hyperarousal and anger of PTSD in patients who also have BPD. Because the comorbidity of PTSD in the BPD population is high, this finding is potentially quite relevant. This provides an example that may be most relevant to this review, that pharmacotherapy in BPD often appears most effective when there is a comorbid Axis I disorder, and the pharmacologic agent chosen has been found to be effective in reducing the symptoms of that comorbid Axis I disorder when it presents solely as an Axis I disorder.
What confounds our overall choice of which medication to use in any particular patient with BPD is that a given medication often can impact many different symptoms of BPD. Thus, whereas in some studies, atypical antipsychotics seem to be no better than placebo, in other studies, we find that the studied medication is effective for anxiety, impulsivity, aggression, and mood lability. Then, when we turn to a different pharmacologic class, such as the mood stabilizers, the same dilemma appears. Some studies reveal little or no effect and some suggest that the mood stabilizer can impact not only mood or mood lability, but anxiety, aggression, and perhaps impulsivity as well—the same array of symptoms that some antipsychotic medications appear to impact. Cognitive distortions seem to respond most often and most specifically to antipsychotic medication.
The question then arises as to how to proceed. The NICE Guidelines, as summarized above, may provide us with the wisest set of considerations [6••]. Further guidance may come from the fact that not only will the effect of the medication in BPD patients be modest at best, but also that patients with BPD may be more sensitive to the side effects of the medications. Then the prescriber needs to weigh the cost–benefit ratio of that particular medication in the particular patient. Thus, although the cost–benefit ratio of a mood stabilizer may appear to favor the use of the medication for the mood instability of bipolar disorder, that cost–benefit ratio may shift substantially if one is considering the same medication in a patient whose mood instability is seen as part of BPD. Furthermore, when considering a medication in bipolar disorder, one is often thinking about a lifetime of prescribing that medication, whereas in BPD, one may wish to use the medication for as short a time as possible [6••], with the hope that psychosocial treatments will provide additional resilience and stronger coping skills [42] so that the patient may, in the near or medium term, be able to manage moods without reliance on medications.
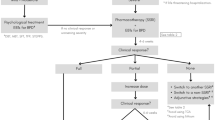
Because these patients present with a wide array of symptoms, it is easy to end up with the patient on multiple medications, one for mood, one for mood lability, one for cognitive distortions when stressed, one for anxiety, and one for sleep. It is hard to predict what such a combination might achieve save for weight gain and a sense of distance or “fogginess” in the patient that he or she is not fully connected to the world. Thus, the wisest (though not always the easiest) way to proceed would be to begin a trial with a single medication with the goal of targeting a specific behavior or symptom, then prescribe that medication in sufficient doses for a long enough time to be able to evaluate whether some clinical response has occurred. If there is no response, then discontinue the medication and try another medication, perhaps, although not always, from a different class of medications. If a clinical response occurs, then evaluate the degree of improvement in the patient and examine which behaviors and symptoms are still present before making a decision as to whether continued improvement might be gained from adding any additional medications. One must ask the question as to whether the problems associated with the addition of another medication outweigh the benefit of adding a second medication.
A final word about the trend toward greater evidence for the effectiveness of atypical antipsychotics and mood stabilizers than for antidepressants, particularly the SSRIs. Caution is needed here because no RCTs have evaluated the use of SSRIs in BPD since 2002 [43]. This is probably related to the fact that all the SSRIs, save for one (escitalopram), are now available in the United States in generic versions. Thus, the pharmaceutical industry has no incentive to conduct these trials and no governmental funding support is available to continue to examine this class of medications. Although the studies of SSRIs carried out through the 1990s did not leave a very impressive mark, the evidence for greater effectiveness of atypical antipsychotics and mood stabilizers may have more to do with the total number of trials that have been performed for each class rather than being based on a solid body of evidence that strongly supports effectiveness of any specific class [37, 44].
There remains great heterogeneity across studies of BPD. Saunders and Silk [37] and Zanarini et al. [39] have suggested that a consortium be formed to discuss guidelines for future studies. Topics to be addressed should include which single medication in each class should be the prototypic medication for that class, which key instruments should be used across studies to measure improvement, and which outcomes ought to be examined to appreciate the effectiveness of pharmacologic treatment. This may help us avoid a scenario in which each different group of researchers decides which metric(s) they think ought to be the outcome measure in any particular study. If we could achieve some consensus, we might finally be able to have sufficient numbers of participants by combining the results from one study (from one center) with results from other centers. Then, with larger numbers of individuals under study with essentially the same methods and metrics being used, we may begin to appreciate better which drugs are truly effective in modifying the symptoms and behaviors that are so troubling in our patients with BPD and for the people who try to treat them.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Soloff PH: Pharmacotherapy of borderline disorders. Compr Psychiatry 1981, 22:535–543.
Zanarini MC, Frankenburg FR, Khera GS, Bleichmar J: Treatment histories of borderline inpatients. Compr Psychiatry 2001, 42:144–150.
Oldham JM, Bender DS, Skodol AE, et al.: Testing an APA practice guideline: symptom-targeted medication utilization for patients with borderline personality disorder. J Psychiatr Pract 2004, 10:156–161.
Baker-Glenn E, Steels M, Evans C: Use of psychotropic medication among psychiatric out-patients with personality disorder. The Psychiatrist 2010, 34: 83–86.
•• Stoffers J, Völlm BA, Rücker G, et al.: Pharmacological interventions for borderline personality disorder. Cochrane Database Syst Rev. 2010, 6:CD005653. This is the full Cochrane systematic review of the pharmacotherapy of BPD. It is a fascinating and thoroughly detailed document, but it may be easier to digest in the more condensed version by Lieb et al. [29••].
•• National Institute for Health and Clinical Excellence (NICE). Borderline Personality Disorder, Treatment and Management. London: The British Psychological Society and The Royal College of Psychiatrists. Available at http://www.nice.org.uk/CG78. Accessed May 1, 2010. As part of the NICE Guideline, this is a thorough review of the psychopharmacologic treatment of BPD. The authors are fairly negative about the usefulness of pharmacologic treatment, but they do give, in the fuller version, guidelines on psychopharmacologic treatment and many details as to how they evaluated the existing literature.
American Psychiatric Association. Practice Guideline for the Treatment of Patients with Borderline Personality Disorder. Am J Psychiatry 2001, 158:1–52
• Schulz SC, Zanarini MC, Bateman A, et. al.: Olanzapine for the treatment of borderline personality disorder: variable dose 12-week randomised double-blind placebo-controlled study. Br J Psychiatry 2008, 193:485–492. This is the largest clinical trial in terms of numbers of participants of BPD pharmacotherapy ever conducted. Unfortunately, the results are not impressive.
• Linehan MM, McDavid JD, Brown MZ, et al.: Olanzapine plus dialectical behavior therapy for women with high irritability who meet criteria for borderline personality disorder: a double-blind, placebo-controlled pilot study. J Clin Psychiatry 2008, 69:999–1005. This study combined dialectical behavioral therapy plus medication or placebo. It re-creates clinical reality, in which most patients receive pharmacotherapy as well as psychosocial (psychotherapeutic) treatment. Both groups improved, and the active medication group improved more (but not significantly more) quickly.
Shafti SS, Shahveisi B: Olanzapine versus haloperidol in the management of borderline personality disorder: a randomized double-blind trial. J Clin Psychopharm 2010, 30:44–47.
• Pascual JC, Soler J, Puigdemont D, et al.: Ziprasidone in the treatment of borderline personality disorder: a double-blind, placebo-controlled, randomized study. J Clin Psychiatry 2008, 69:603–608. This is a negative study for an atypical antipsychotic. The only solidly positive RCT for an atypical antipsychotic is with aripiprazole (Nickel et al. [44]), with some contradictory evidence for olanzapine.
Loew TH, Nickel MK, Muehlbacher M, et. al.: Topiramate treatment for women with borderline personality disorder: a double-blind, placebo-controlled study. J Clin Psychopharm 2006, 26:61–66.
• Nickel MK, Loew TH: Treatment of aggression with topiramate in male borderline patients, part II: 18-month follow-up. Eur Psychiatry 2008, 23:115–117. This study complements this group’s previous study showing the effectiveness of topiramate in women.
• Reich DB, Zanarini MC, Bieri KA: A preliminary study of lamotrigine in the treatment of affective instability in borderline personality disorder. Int Clin Psychopharm 2009, 24:270–275. This is another study that supports the effectiveness of mood stabilizers in the BPD population.
• Ziegenhorn AA, Roepke S, Schommer NC, et.al. : Clonidine improves hyperarousal in borderline personality disorder with or without comorbid posttraumatic stress disorder: a randomized, double-blind, placebo-controlled trial. J Clin Psychopharma 2009, 29:170–173. This is an intriguing study that revealed the effectiveness of clonidine. However, the effectiveness seemed restricted to patients who also had comorbid PTSD.
Zanarini MC, Vujanovic AA, Parachini EA, et al.: Zanarini Rating Scale for Borderline Personality Disorder (ZAN-BPD): a continuous measure of DSM-IV borderline psychopathology. J Personal Disord 2003, 17:233–142.
Bogenschutz MP, Nurnberg HG: Olanzapine versus placebo in the treatment of borderline personality disorder. J Clin Psychiatry 2004, 65:104–109.
Villeneuve E, Lemelin S: Open-label study of atypical neuroleptic quetiapine for treatment of borderline personality disorder: impulsivity as main target. J Clin Psychiatry 2005, 66:1298–303.
Bellino S, Paradiso E, Bogetto F: Efficacy and tolerability of quetiapine in the treatment of borderline personality disorder: A pilot study. J Clin Psychiatry 2006, 67:1042–1046.
Adityanjee, Romine A, Brown E, et al.: Quetiapine in patients with borderline personality disorder: an open-label trial. Ann Clin Psychiatry 2008, 20:219–226
van den Eynde F, Senturk V, Naudts K, et al.: Efficacy of quetiapine for impulsivity and affective symptoms in borderline personality disorder. J Clin Psychopharm 2008, 28:147–155.
Quitkin FM: Placebos, drug effects, and study design: a clinician’s guide. Am J Psychiatry 1999, 156: 829–836.
Bellino S, Zizza M, Rinaldi C, Bogetto F: Combined treatment of major depression in patients with borderline personality disorder: a comparison with pharmacotherapy. Can J Psychiatry 2006, 51:453–460.
• Bellino S, Rinaldi C, Bogetto F: Adaptation of interpersonal psychotherapy to borderline personality disorder: a comparison of combined therapy and single pharmacotherapy Can J Psychiatry 2010, 55:74–81. This is another study (though open-label) exploring the effectiveness of combined psychotherapy and psychopharmacology. Length of treatment seemed to be the most important variable related to improvement.
Bellino S, Paradiso E, Bozzatello P, Bogetto F: Efficacy and tolerability of duloxetine in the treatment of patients with borderline personality disorder: a pilot study. J Psychopharm 2010, 24:333–339.
Arntz A, van den Hoorn M, Cornelis J, et al.: Reliability and validity of the borderline personality disorder severity index. J Person Disord 2003, 17:45–59.
Miyaoka T, Furuya M, Yasuda H, et al.: Yi-gan san for the treatment of borderline personality disorder: an open-label study. Prog Neuropsychopharmacol Biol Psychiatry 2008, 32:150–154.
Binks CA, Fenton M, McCarthy L, et al.: Pharmacological interventions for people with borderline personality disorder. Cochrane Database Syst Rev 2006, 25:CD005653.
•• Lieb K, Völlm B, Rücker G, et al.: Pharmacotherapy for borderline personality disorder: Cochrane systematic review of randomised trials. Br J Psychiatry 2010, 196:4–12. This is the shorter, more concise, more accessible version of the Cochrane review (Stoffers et al. [5••]).
Abraham PF, Calabrese JR: Evidenced-based pharmacologic treatment of borderline personality disorder: a shift from SSRIs to anticonvulsants and atypical antipsychotics? J Affect Disord 2008, 111:21–30.
Nosè M, Cipriani A, Biancosino B, et al.: Efficacy of pharmacotherapy against core traits of borderline personality disorder: meta-analysis of randomized controlled trials. Int Clin Psychopharm 2006, 21:345–353.
Herpertz SC, Zanarini M, Schulz CS, et al.: World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for biological treatment of personality disorders. World J Biol Psychiatry 2007, 8: 212–244.
•• Mercer D, Douglass AB, Links PS: Meta-analyses of mood stabilizers, antidepressants and antipsychotics in the treatment of borderline personality disorder: effectiveness for depression and anger symptoms. J Personal Disord 2009, 23:156–174. This is an excellent meta-analysis that limited itself to studying the outcomes for depression and anger symptoms. Mood stabilizers had the largest effect on anger, with a moderate effect on depression. Antidepressants had a moderate effect on anger but only a small effect on depression. Antipsychotics (particularly aripiprazole) had a moderate effect on anger but no effect on depression. It is worth comparing these results with those of Ingenhoven et al. [35•].
Duggan C, Huband N, Smailagic N, et al.: The use of pharmacological treatments for people with personality disorder: a systematic review of randomized controlled trials. Personality Ment Health 2008, 2: 119–170.
• Ingenhoven T, Lafay P, Rinne T, et al.: Effectiveness of pharmacotherapy for severe personality disorders: meta-analyses of randomized controlled trials. J Clin Psychiatry 2010, 71:14–25. This excellent meta-analysis found that antipsychotics have a moderate effect on cognitive-perceptual symptoms and a moderate to large effect on anger, while antidepressants have no significant effect on impulsivity or depressed mood but a small effect on anxiety and anger. Mood stabilizers had a very large effect on impulsivity, a large effect on anxiety, and a moderate effect on depressed mood. This study provides support for mood stabilizer use in BPD patients, and it is worth comparing and contrasting it with the Mercer et al. [33••] meta-analysis.
• Díaz-Marsá M, González Bardanca S, Tajima K, et al.: Psychopharmacological treatment in borderline personality disorder. Actas Esp Psiquiat .2008, 36:39–49. This is a very thorough review that proposes updated algorithms for the pharmacologic treatment of the following temperamental dimensions found in BPD: impulsivity-aggression, emotion instability, cognitive-perceptual distortions, and anxiety-inhibition. It is in English.
Saunders EFH, Silk K: Personality trait dimensions and the pharmacologic treatment of borderline personality disorder. J Clin Psychopharm 2009, 29: 461–267.
Silk KR, Jibson MD (2010) Personality disorders. In: Rothschild AJ (ed) The Evidence-Based Guide to Antipsychotic Medications. Washington DC: American Psychiatric Publishing, Inc; 2010, pp 101–124
Zanarini MC, Stanley B, Black DW, et al.: Methodological considerations treatment trials for persons personality disorder. Ann Clin Psychiatry 2010, 22:75–83.
Zanarini MC, Frankenburg FR, DeLuca CJ, et al.: The pain of being borderline: dysphoric states specific to borderline personality disorder. Harvard Rev Psychiatry 1998, 6:201–207.
Silk KR, Jibson MD: Personality disorders. In The Evidence-Based Guide to Antidepressant Medications. Edited by Rothschild AJ. Washington DC: American Psychiatric Publishing, Inc; Inc; 2011, In press.
Bateman A, Zanarini MC: Personality disorders. In Cambridge Textbook of Effective Treatments in Psychiatry. Edited by Tyrer P, Silk KR. Cambridge, UK: Cambridge University Press; 2008, pp 659–681.
Rinne T, van den Brink W, Wouters L, et al. : SSRI treatment of borderline personality disorder: a randomized, placebo-controlled clinical trial for female patients with borderline personality disorder. Am J Psychiatry 2002, 159: 2048–2054.
Nickel MK, Muehlbacher M, Nickel C, et al.: Aripiprazole in the treatment of patients with borderline personality disorder: a double-blind, placebo-controlled study. Am J Psychiatry 2006, 163:833–838.
Acknowledgment
Dr. Silk has served as secretary-treasurer for the International Society for the Study of Personality Disorders.
Disclosure
No potential conflicts of interest relevant to this article were reported.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Feurino, L., Silk, K.R. State of the Art in the Pharmacologic Treatment of Borderline Personality Disorder. Curr Psychiatry Rep 13, 69–75 (2011). https://doi.org/10.1007/s11920-010-0168-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11920-010-0168-9