
Abstract
Perioperative management of patients receiving opioid addiction therapy presents a unique challenge for the anesthesiologist. The goal of pain management in this patient population is to effectively manage postoperative pain, to improve patient satisfaction and outcomes, and to reduce the cost of health care. Multimodal analgesics, including nonsteroid anti-inflammatory drugs, intravenous acetaminophen, gabapentanoid agents, and low-dose ketamine infusions, have been used to improve postoperative pain and to reduce postoperative opioid use. Patients on long-term opioid management therapy with methadone and buprenorphine require special considerations. Recommendations and options for treating postoperative pain in patients on methadone and buprenorphine are outlined below. Other postoperative pain management options include patient-controlled analgesia, intravenous, and transdermal, in addition to neuraxial and regional anesthesia techniques. Special patient populations include the parturient on long-term opioid therapy. Recommendations for use of opioids in these patients during labor and delivery and in the postpartum period are discussed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Pain, both acute and chronic, impacts nearly everyone in the world. The International Association for the Study of Pain and the World Health Organization defines pain as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage” [1]. Individual lifestyle factors such as smoking, obesity, and poor health status may also play a role in the development of pain conditions [2]. Psychosocial variables thought to have impact on pain prevalence include stress, anxiety, depression, low self-esteem, and the presence of chronic health problems [3, 4]. The socioeconomic effect of pain is huge, and it has been estimated that individuals with moderate to severe chronic pain lose an average of 8 days of work every 6 months and 22 % lose at least 10 workdays [5].
In 2010, about 100 million adults in the USA were affected by chronic pain, including joint pain or arthritis [6, 7••]. The total costs ranged from $560 billion to $635 billion in 2010. The annual cost of pain is greater than the annual costs of heart disease ($309 billion), cancer ($243 billion), and diabetes ($188 billion) [6, 7••]. It is clear therefore, that persistent chronic pain is a long-term condition, which affects the lives of people by interfering with their quality of life both at home and at work with significant societal consequences. Further, treatments, including medications, physical therapies, and interventional pain procedures, have been developed with aims to minimize suffering and to improve functional status.
Opioid medications are among the most common classes of drugs prescribed worldwide. Exogenous opioids shut down endogenous opioid production and can lead to a significant number of patients taking these agents long term. These drugs are also associated with morbidity and mortality individually and in association with other drugs with additive or synergistic respiratory depressive effects. Further, prescription opioid painkillers are considered a major contributor to the total number of drug deaths. In 2007, for example, nearly 28,000 Americans died from unintentional drug poisoning, and of these, nearly 12,000 involved prescription pain relievers [8]. Opioid medications are clearly effective for many types of pain states and longer acting agents, such as methadone and buprenorphine, and have been developed for patients with long standing pain states and/or substance abuse history.
Since we are treating an increasing number of people for chronic pain, and we are seeing an increase in illicit opioid use, the clinical anesthesiologist is seeing more patients on long-term opioid therapies such as methadone and buprenorphine. With over three million people on or having been treated with buprenorphine, and approximately 50 times that on methadone treatment, treating these patients’ acute postoperative pain is emergently becoming an issue and a challenge for anesthesiologists.
Related to many reasons, therefore, patients with chronic pain on medications such as methadone or buprenophrine pose special considerations for surgery and in the management of associated acute pain treatment. Though large randomized prospective studies are lacking with the chronic pain patient subpopulation on either methadone or buprenorphine, a best practice strategy should include preemptive analgesia and multimodal therapies. This review will describe pharmacological considerations for methadone and buprenorphine. It will also discuss anesthetic management practices and potential strategies that are currently available in clinical practice. Special consideration for pregnant patients on these agents is also reviewed.
Patient Evaluation and Screening Tools
Patients on opioid addiction therapy presenting for surgery present a challenge to an anesthesiologist. There are several different approaches to analgesia in this subpopulation; however, the first step is obtaining a detailed and comprehensive history. Building a good line of communication and trust with these patients will allow the patient to be honest about their drug history. When collecting the patient’s history, it is vital to be professional and preserve a nonjudgmental environment. Focus on specific questions, such as a history of drug dosage, frequency of ingestion, time of last dose, and any possible illicit drug use. The commonly used questionnaire used to detect alcohol abuse has been modified to include drug abuse. In this regard, the CAGE-AID questionnaire includes four questions. (1) Have you ever felt that you ought to cut down on your drinking or drug use? (2) Have people annoyed you by people criticizing your drinking or drug use? (3) Have you ever felt bad or guilty about your drinking or drug use? (4) Have you ever had a drink or used drugs first thing in the morning to steady your nerves or to get rid of a hangover (Eye opener)? While the history is subjective data, it is an indispensable in the care of these patients.
Urinary drug screening (UDS) is vital in obtaining objective information about the patient’s opioid history and drug history. Patients may be selling their opioid medication, which would result in a negative UDS and should raise suspicion of illicit activity. However, a UDS can return false-positive results, which results in a confirmation process that is potentially time consuming, inaccurate, and expensive. Furthermore, a UDS cannot detect past abuse, which justifies why a detailed history is crucial. Whenever possible, dose verification with the opioid maintenance program should be attempted, as it will also give better insight of the patient from a physician who has been taking care of the patient long-term.
New Perioperative Techniques and Advancements
To date, there have been no randomized controlled studies published evaluating pain management modalities for patients on opioid dependence therapy [9]. Recommendations are currently based on case reports and antidotal experiences of physicians. Effective postoperative pain management increases patient satisfaction, improves patient outcomes, and reduces the cost of health care.
Preemptive analgesia is defined as an anti-nociceptive treatment that prevents the establishment of altered central processing of afferent input associated with tissue injury and inflammation [10••]. Agents currently used in the preoperative setting include nonsteroid inflammatory drugs (NSAIDs), gabapentinoids, acetaminophen, clonidine, dexamethasone, and regional/neuraxial anesthesia.
Perioperative pain management for these patients should consist of multimodal analgesics with the goal of improving postoperative pain and reducing opioid analgesic use. The addition of NSAIDs to perioperative analgesia regimens reduces opioid requirements by approximately 20–30 % [11]. The use of intravenous acetaminophen has proven to provide lower pain scores with preemptive use at 6 h after surgery when compared to a placebo group [12]. Khurana and et al. reported that subjects receiving pregabalin showed consistently reduced pain intensity and also required less rescue pain medications in the postoperative period [13]. Chelly and colleagues reviewed 39 clinical trials and showed that a continuous infusion of low-dose ketamine intraoperatively provided a reduction of pain scores and reduction of the opioid consumption [14•]. All of these studies provide us with evidence with that multimodal analgesia approach less centered on opioids can lead to a more effective analgesia in patients. While these techniques have never been studied in patients on opioid maintenance therapy, it is safe to say that they only play a more vital role in this patient population where opioids are commonly ineffective.
Methadone and Buprenorphine
Methadone is a long-acting opioid agonist that is structurally unrelated to other opioids. It is commonly used in the treatment of heroin and other opioid abuse disorders. It is a racemic mixture of two isomers. An R-isomer is an NMDA receptor antagonist which also inhibits uptake of norepinephrine and serotonin, and an S-isomer is a mu and delta receptor agonist [15]. Its binding to and occupying of mu-opioid receptors prevents withdrawal symptoms for a very significant period of time, reduces craving for opioids, and, by maintaining high levels of opioid tolerance, reduces the euphoric effects of subsequent illicit opioid use [16, 17]. It is well-established that the half-life of methadone is approximately 1 day and it takes five half-lives for the majority of a drug at steady state to be eliminated. Therefore, it would take approximately 4–5 days for withdrawal symptoms to become evident. It is highly lipophilic with bioavailability ranging from 36 to 100 %. It is primarily bound to α1-acid glycoprotein (85 to 90 %), metabolized by cytochrome P450 into inactive metabolites, and fecally and renally excreted [15].
Buprenorphine (Subutex) is an opioid agonist-antagonist with a half-life of 37 h. It is a partial agonist at mu-opioid receptors but is a kappa-opioid receptor antagonist [18, 19]. Suboxone is a combination of buprenorphine and naloxone, a mu-opioid antagonist. Naloxone is utilized as a deterrent to reverse the effects of opioids when patients inappropriately crush the drug for intravenous use or snort the drug, which either may result in overdose with respiratory failure [20].
The binding of buprenorphine to both mu and kappa receptors results in hyperpolarization and reduced neuronal excitability. Furthermore, it slowly dissociates from its receptor, which accounts for its long duration of action [18, 19]. Buprenorphine is known as a partial agonist, with less dose-response effect, including less respiratory depression than methadone related to its ceiling effect, and therefore, has less overdose potential [21, 22]. Its bioavailability is 31 % sublingually but undergoes first pass metabolism when taken orally resulting in very low oral bioavailability. It is 96 % bound to alpha and beta globulin and undergoes hepatic metabolism by cytochrome P450 into norbuprenorphine, an active metabolite that has one fifth of the pharmacologic activity of the parent compound. It is eliminated via feces and urine [18].
Pain Management with Methadone and Buprenorphine and Substance Abuse History
Managing acute pain in patients who are on long-term opioid management such as methadone and buprenorphine can be challenging. Physicians have several misconceptions as to how to manage acute pain in these patients, which could be due to opiophobia, which results in under medicating these patients with opioids and other non-opioid analgesics [23]. Other concerns are fear of respiratory depression, addiction relapse, and prescription drug diversion.
Patients on Methadone
The daily methadone dose should be continued until the day of surgery and in the perioperative period. Acute pain should be treated with opioids and non-opioid analgesics and other adjuncts whenever possible such as regional and neuraxial anesthetic techniques. The correct dose of methadone should be verified with the patient and by the methadone-prescribing clinic. Further, the clinic should be informed of the patient’s inpatient requirements of opioids and date of admission and discharge.
If postoperative intake of methadone is not possible, an intravenous dose of methadone can be given. Methadone has a high but variable oral bioavailability ranging from 30 to 100 %. If IV to oral conversion is sought out for the ratio should be 1:1. Some patients could require an upward titration of oral methadone with a ratio of 1:2. However, while converting methadone from oral to IV form, the most common initial ratio used is 2:1. Some patients may require dose escalation to ratios of 1:1. Converting oral to subcutaneous form can be difficult due to varied oral bioavailability. Commonly used ratio of conversion is PO:SC:2:1. This ratio can be escalated to 1:1 if no response to therapy is seen.
Patients on Buprenorphine
Option 1. Discontinue Buprenorphine Therapy
-
(1)
Discontinue buprenorphine therapy 72 h prior to the operative procedure. This eliminates the partial blockade caused by buprenorphine due to its partial agonistic activity. Buprenorphine is discontinued preoperatively over a period of 2–3 weeks with a gradual decrease of 2 mg/day of buprenorphine every 2–3 days and completely discontinued 72 h before surgery. Buprenorphine can also be tapered rapidly over 3 days; however, relapse rates are higher. Patients should be buprenorphine free for 72 h prior to planned procedure. If patients are unable to tolerate withdrawal, maintenance dose of buprenorphine is replaced with an opioid or methadone.
Further doses of pure opioid agonists are added to provide acute pain control.
The patient can either be discharged home on pure opioid agonist drugs with induction protocol of buprenorphine [24] initiated after discharge or induction protocol of buprenorphine can be initiated inpatient after resolution of acute pain.
-
(2)
Buprenorphine can be converted to methadone at 30–40 mg/day. This dose prevents withdrawal symptoms in most patients [25]. Baseline and acute pain opioid requirements are managed with opioid agonists. If withdrawal symptoms persist, methadone can be increased by 5–10 mg per day. With this dosing regimen, response to opioid agonists is more predictable.
After resolution of acute pain, maintenance therapy of buprenorphine is initiated using an induction protocol [24].
Patients should be in mild opioid withdrawal (clinical opioid withdrawal score of 10–12 or greater) prior to initiation of induction protocol of buprenorphine to avoid precipitation of acute withdrawal. Buprenorphine displaces other pure opioid agonists from the receptors; however, as it is a partial agonist, it does not completely activate the receptor like a pure opioid agonist does causing acute withdrawal symptoms in an opioid-dependent patient.
Option 2. Continue Buprenorphine Therapy
-
(1)
Continue maintenance therapy of buprenorphine and treat acute pain with opioid agonists. Higher doses of opioid agonists may be necessary to provide desired analgesia, as they have to compete with buprenorphine at the mu receptor sites. Consider adding opioids with higher intrinsic mu activity such as morphine, fentanyl, or hydromorphone while opioids with less efficacy at the mu receptor such as codeine and hydrocodone are best avoided in this setting. Sublingual and intravenous buprenorphine added to the above regimen also provides good analgesia [26].
-
(2)
Daily dose of buprenorphine can be divided into every 6 or 8 h dosing cycle. This regimen utilizes the analgesic properties of buprenorphine. This regimen can be used in patients with only mild to moderate pain due to the ceiling effect of buprenorphine seen at doses above 32 mg/day sublingual [27]. Agonistic effects of buprenorphine linearly increase up to this dose and reach a plateau and no longer increase with further doses of buprenorphine. Further doses of opioid analgesics may be needed [28].
Patient-Controlled Analgesia
Patient-controlled analgesia (PCA) is a useful method of self-dosing in a closed loop system in which the patient plays an active role in opioid administration. Self-titration provides better patient satisfaction and prevents under-dosing. Patient-controlled analgesia can be administered through various routes: intravenous, which is the most common route, epidural, peripheral nerve catheters, and transdermal.
Long-term methadone or buprenorphine use may necessitate certain PCA adjustments to properly treat postoperative pain. Table 1 provides a framework for converting their current dosage to an intravenous dose postoperatively. Even with this knowledge, finding their correct dose may take time. Adding a PCA basal dose may be necessary in patients on chronic opioid therapy. Also, frequent PCA setting changes may be needed to obtain the desired pain relief.
Rapp et al. found that patients on methadone or buprenorphine preoperatively who are started on PCA postoperatively had a decreased incidence of nausea, vomiting, and pruritus; however, they experienced increased levels of sedation when compared to opioid naïve patients on a PCA. Anesthesiologists caring for these individuals should be aware that these patients are frequently prescribed other medications which could impact side effects postoperatively. Lack of expected tolerance to sedation in this study was possibly linked to the synergistic effects of opioid use in combination with an anxiolytic (19 % of patients in this study) [32].
Transdermal PCA eliminates the need for venous access and uses the principle of iontophoresis. Iontophoresis uses a low intensity current to drive ionization of drug molecules. The electric current travels from the anode to the cathode and uses the skin to complete the circuit required for drug delivery. Once ionized, these molecules are driven across the skin and into the systemic circulation by this electric current.
The transdermal PCA is a preprogrammed self-contained delivery system that is easy to apply and use. This drug delivery route by-passes first hepatic metabolism and may avoid common postoperative issues experienced with oral medications such as nausea, vomiting, and difficulty swallowing. Fentanyl is the most commonly used opioid agent for transdermal PCA due to its high lipid solubility and potency. Chelley et al. and Viscusi et al. demonstrated its safety profile and use in acute postsurgical patients [33, 34].
Pregnant Women and Opioids
Antepartum maternal opioid abuse has increased from 1.19 (95 % CI, 1.01–1.35) to 5.63 (95 % CI, 4.40–6.71) per 1000 hospital births per year [35] and the use of first trimester opioid use in the USA was ∼20 % in 2009. Opioids cross placenta and can result in low birth weight, meconium aspiration, and fetal intolerance to labor. Neonates born to opioid-dependent mothers exhibit neonate abstinence syndrome (NAS) at an estimated rate of about 5.6 %; opioid withdrawal, microcephaly, and growth retardation are at a higher risk of sudden infant death syndrome and infant mortality [36]. Preeclampsia, maternal hemorrhage, and third trimester bleeding are frequently seen complications in pregnant patients taking opioids.
Opioid Replacement Therapy During Pregnancy
Methadone and buprenorphine are both category C drugs. Methadone has traditionally been used since the 1970s for opioid addiction during pregnancy and is prescribed by federally approved methadone clinics. Metabolism of methadone is increased during pregnancy, and the dose should be adjusted accordingly. The safety profile of buprenorphine during pregnancy has not been proven; risks vs. benefits should be discussed with the patient before initiation of buprenorphine treatment. Whenever possible, patient should be started on or transitioned to methadone.
The use of methadone results in better treatment retention than buprenorphine; however, buprenorphine maintenance during pregnancy results in better fetal and maternal outcomes [37]. One study concluded that the symptoms of neonatal abstinence syndrome were less severe in mothers maintained on buprenorphine than methadone; however, rates of NAS were similar in both groups [38]. Mixed agonistic-antagonistic opioids such as nalbuphine, butorphanol, and pentazocine should be avoided as it can precipitate withdrawal.
Pain Management During Labor and Delivery and Postpartum
Epidural analgesia is safe during labor. Spinal anesthesia is a reasonable option in providing surgical anesthesia for a cesarean section. Addition of intrathecal narcotics is based on the anesthesiologist’s preference. Neuraxially administered opioids may not prevent opioid withdrawal.
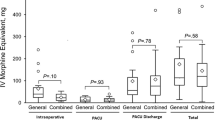
Opioid-dependent pregnant patients can be hyperalgesic, and these patients require additional pain medications tailored to their need. NSAIDS and acetaminophen are usually sufficient in patients who have delivered vaginally. Post-cesarean section pain in patients who are opioid-dependent can be managed with a PCA or higher doses of PO narcotics in addition to NSAIDS and acetaminophen [39]. Women on methadone maintenance therapy required approximately 70 % more opioid analgesic in the first 24 h after cesarean delivery compared to non-opiate-dependent control patients. Higher pain scores was noted in methadone maintained patients after vaginal delivery; however, opioid utilization was similar to non-opioid-dependent control patients [40].
In patients who are on buprenorphine, the total dose of buprenorphine can be divided and administered every 6–8 h to take advantage of its analgesic properties. Supplemental buprenorphine, 2–4 mg every 6–8 h can be added. Transverse abdominal plane blocks can be performed as an adjunct to spinal anesthesia without intrathecal morphine to reduce total opioid consumption in the first 24 h [41].
A study done by Jabalameli et al. suggests infiltrating site of surgery with subcutaneous methadone 10 mg. There was no statistical significant difference in the two groups in terms of morphine use; however, mean pain severity was reduced in the subcutaneous methadone group [42]. Individualized pain control is needed, and the anesthesiologist caring for these patients should discuss pain management options before delivery.
Breast-Feeding Guidelines
Buprenorphine is excreted in the breast milk at a ratio of 1:1. Due to its poor oral bioavailability, breast milk exposure of buprenorphine has minimal effects on the neonatal abstinence scoring in infant. Latest guidelines by the Academy of Breastfeeding Medicine Committee recommend breast-feeding for mothers on methadone and buprenorphine if there is no other contraindication [43].
End Goal: Multidimensional Approach to Treatment
Patients on long-term opioid management are seen in the inpatient setting frequently for elective and emergent surgery and for medical illness. A collaborative and multidisciplinary approach involving the patient, anesthesiologist, surgeon, outpatient chronic pain specialist, and treating physician should be utilized.
Involving the patient early gives the treating physician an opportunity to set reasonable expectations in relation with acute pain management. Stress and anxiety in the perioperative period should be addressed promptly. Patients should be reassured that their history of drug addiction and long-term opioid use will not result in under treatment of their pain. Treating acute pain with opioids does not increase rate of relapse. Timeline for resolution of acute pain symptom should be addressed. End point of therapy is to facilitate return of the patient to the community with close to preadmission baseline opioid requirements. McQauy et al. suggest a step down approach to treat acute pain by using a reverse order WHO analgesic ladder until the patients baseline opioid requirements are met [44].
Discharge planning should commence at an early stage. Recovery related activities such as daily reading, journaling, participation in faith meetings; sponsor meetings and family interaction and support groups should be encouraged. Education on pain self-management should be discussed; patients should apply new skills learned to manage their pain and should not be a passive recipient of pain services [45]. Follow up appointments should be scheduled with the treating physician. An open line of communication should be established with the patient’s physician, and information about inpatient opioid and non-opioid use must be shared.
Conclusion
Patients on long-term opioid addiction therapy require special consideration when it comes to perioperative pain management. A collaborative effort between all involved, including the patient, the anesthesiologist, surgeon, chronic pain physician, and other treating physicians, is important to provide a positive perioperative experience. New perioperative techniques and advancements are available to effectively manage postoperative pain in patients on long-term opioid addiction medications. The use of multimodal analgesia helps to decrease postoperative pain and reduce opioid use. Patients on methadone and buprenorphine therapy have options in the perioperative period. The anesthesiologist is the common denominator providing care for the patient from the time of preoperative preparation, into the intraoperative period, and finally, into the postoperative phase of care. Therefore, the anesthesiologist should stay abreast of how to manage the patient on long-term opioid therapy, such as methadone and buprenorphine, presenting for surgery and/or labor and delivery.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
IASP Taxonomy - IASP. [Online]. Available: http://www.iasp-pain.org/Taxonomy?&navItemNumber=576. Accessed 14 Dec 2015.
Peat G, McCarney R, Croft P. Knee pain and osteoarthritis in older adults: a review of community burden and current use of primary health care. Ann Rheum Dis. 2001;60(2):91–7.
King S, Chambers CT, Huguet A, MacNevin RC, McGrath PJ, Parker L, et al. The epidemiology of chronic pain in children and adolescents revisited: a systematic review. Pain. 2011;152(12):2729–38.
Hoy D, Brooks P, Blyth F, Buchbinder R. The epidemiology of low back pain. Best Pract Res Clin Rheumatol. 2010;24(6):769–81.
Reid KJ, Harker J, Bala MM, Truyers C, Kellen E, Bekkering GE, et al. Epidemiology of chronic non-cancer pain in Europe: narrative review of prevalence, pain treatments and pain impact. Curr Med Res Opin. 2011;27(2):449–62.
Gaskin DJ, Richard P. The economic costs of pain in the United States. J Pain. 2012;13(8):715–24.
Relieving pain in America: a blueprint for transforming prevention, care, education, and Research - Institute of Medicine. [Online]. Available: http://iom.nationalacademies.org/reports/2011/relieving-pain-in-america-a-blueprint-for-transforming-prevention-care-education-research.aspx. Accessed 14 Dec 2015. This is an excellent and comprehensive review of pain and how to treat pain. This review includes pain as a public health concern and the diagnosis and treatment of pain as well as discussion on the variety of new treatments for pain that are available today.
Unintentional drug poisoning in the United States. [Online]. Available: http://www.cdc.gov/HomeandRecreationalSafety/pdf/poison-issue-brief.pdf. Accessed 14 Dec 2015.
May JA, White HC, Leonard-White A, Warltier DC, Pagel PS. The patient recovering from alcohol or drug addiction: special issues for the anesthesiologist. Anesth Analg. 2001;92(6):1601–8.
Devin CJ, McGirt MJ. Best evidence in multimodal pain management in spine surgery and means of assessing postoperative pain and functional outcomes. J Clin Neurosci. 2015;22(6):930–8. This acticle discusses the treatment of pain utilizing a multimodal approach which is widely accepted as the new gold standard of care. This article includes a comprehensive analysis of commonly used drugs to treat pain as well as exploring inconsistencies in optimal posoperative treatment procotols.
Dahl V, Raeder JC. Non-opioid postoperative analgesia. Acta Anaesthesiol Scand. 2000;44(10):1191–203.
Khalili G, Janghorbani M, Saryazdi H, Emaminejad A. Effect of preemptive and preventive acetaminophen on postoperative pain score: a randomized, double-blind trial of patients undergoing lower extremity surgery. J Clin Anesth. 2013;25(3):188–92.
Khurana G, Jindal P, Sharma JP, Bansal KK. Postoperative pain and long-term functional outcome after administration of gabapentin and pregabalin in patients undergoing spinal surgery. Spine (Phila Pa 1976). 2014;39(6):E363–8.
Jouguelet-Lacoste J, La Colla L, Schilling D, Chelly JE. The use of intravenous infusion or single dose of low-dose ketamine for postoperative analgesia: a review of the current literature. Pain Med. 2015;16(2):383–403. This article reviews the current literature involving ketamine for postoperative analgesia. This article discusses the importance of the way in which ketamine is administered to the patient, either bolus injection or low dose, which can vary between physicians and hospitals.
Eap CB, Buclin T, Baumann P. Interindividual variability of the clinical pharmacokinetics of methadone: implications for the treatment of opioid dependence. Clin Pharmacokinet. 2002;41(14):1153–93.
Donnadieu S. Use of methadone as analgesic. Ann Med Interne. 2000;151(1):A40–3.
Mattick RP, Breen C, Kimber J, Davoli M. Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence. Cochrane database Syst Rev. 2009;(3):CD002209.
Elkader A, Sproule B. Buprenorphine: clinical pharmacokinetics in the treatment of opioid dependence. Clin Pharmacokinet. 2005;44(7):661–80.
Lutfy K, Cowan A. Buprenorphine: a unique drug with complex pharmacology. Curr Neuropharmacol. 2004;2(4):395–402.
Olofsen E, van Dorp E, Teppema L, Aarts L, Smith TW, Dahan A, et al. Naloxone reversal of morphine- and morphine-6-glucuronide-induced respiratory depression in healthy volunteers: a mechanism-based pharmacokinetic-pharmacodynamic modeling study. Anesthesiology. 2010;112(6):1417–27.
Whelan P, Remski K. Buprenorphine vs methadone treatment: a review of evidence in both developed and developing worlds. J Neurosci Rural Pract. 2012;3(1):45.
Mattick RP, Breen C, Kimber J, Davoli M. Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence. Cochrane Database Syst Rev. 2014;2, CD002207.
Goldberg DS. On the erroneous conflation of opiophobia and the undertreatment of pain. Am J Bioeth. 2010;10(11):20–2.
Dunlop A, Panjari M, O’Sullivan H, Henschke P, Love V, Ritter A, et al. Clinical guidelines for the use of buprenorphine in pregnancy. 2003.
ContentServer-3.pdf.
Bullingham RE, McQuay HJ, Dwyer D, Allen MC, Moore RA. Sublingual buprenorphine used postoperatively: clinical observations and preliminary pharmacokinetic analysis. Br J Clin Pharmacol. 1981;12(2):117–22.
Childers JW, Arnold RM. Treatment of pain in patients taking buprenorphine for opioid addiction #221. J Palliat Med. 2012;15(5):613–4.
Johnson RE, Fudala PJ, Payne R. Buprenorphine: considerations for pain management. J Pain Symptom Manag. 2005;29(3):297–326.
Garcia JBS, Cardoso MGM, Dos-Santos MC. Opioides e o sistema imunológico: relevância clínica. Rev Bras Anestesiol. 2012;62(5):713–8.
Equianalgesic opioid dosing calculation isn’t simple math. [Online]. Available: http://www.hcplive.com/conference-coverage/painweek-2013/equianalgesic-opioid-dosing-calculation-isnt-simple-math. Accessed 05 Jan 2016.
Schneider C, Yale SH, Larson M. Principles of pain management. Clin Med Res. 2003;1(4):337–40.
Rapp SE, Ready LB, Nessly ML. Acute pain management in patients with prior opioid consumption: a case-controlled retrospective review. Pain. 1995;61(2):195–201.
Chelly JE, Grass J, Houseman TW, Minkowitz H, Pue A. The safety and efficacy of a fentanyl patient-controlled transdermal system for acute postoperative analgesia: a multicenter, placebo-controlled trial. Anesth Analg. 2004;98(2):427–33. table of contents.
Viscusi E, Reynolds L, Chung F, Atkinson LE, Khanna S. Hydrochloride vs intravenous morphine pump for postoperative pain. Context. 2004;291(11):1333–41.
Schumacher RE. Neonatal abstinence syndrome and associated health care expenditures United States, 2000–2009 trends in neonatal abstinence syndrome. JAMA, J Am Med Assoc. 2012;307(18):1934.
Kellogg A, Rose CH, Harms RH, Watson WJ. Current trends in narcotic use in pregnancy and neonatal outcomes. Am J Obstet Gynecol. 2011;204(3):259.e1–4.
Arria AM, Baewert A, Heil SH, Kaltenbach K, Martin PR, Coyle MG, et al. HHS Public Access. 2015;107(1).
Thomas CP, Fullerton CA, Kim M, Montejano L, Lyman DR, Dougherty RH, et al. Medication-assisted treatment with buprenorphine: assessing the evidence. Psychiatr Serv. 2014;65(2):158–70.
Jones HE, Johnson RE, Milio L. Post-cesarean pain management of patients maintained on methadone or buprenorphine. Am J Addict. 2006;15(3):258–9.
Meyer M, Wagner K, Benvenuto A, Plante D, Howard D. Intrapartum and postpartum analgesia for women maintained on methadone during pregnancy. Obstet Gynecol. 2007;110(2):261–6.
Abdallah FW, Halpern SH, Margarido CB. Transversus abdominis plane block for postoperative analgesia after caesarean delivery performed under spinal anaesthesia? A systematic review and meta-analysis. Br J Anaesth. 2012;109(5):679–87.
Jabalameli M, Kalantari F. Evaluation of the analgesic effect of subcutaneous methadone after cesarean section. 2014. p. 3–6.
Academy of Breastfeeding Medicine Protocol Committee. ABM protocol and the drug-dependent woman. 2009;4(4):225–228.
McQuay H. Relief of chronic non-malignant. Pain. 2006:1–27.
Jensen MP, Nielson WR, Kerns RD. Toward the development of a motivational model of pain self-management. J Pain. 2003;4(9):477–92.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Sudipta Sen, Sailesh Arulkumar, Elyse M. Cornett, Julie A. Gayle, Ronda R. Flower, Charles J. Fox, and Alan D. Kaye declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Additional information
This article is part of the Topical Collection on Other Pain
Rights and permissions
About this article

Cite this article
Sen, S., Arulkumar, S., Cornett, E.M. et al. New Pain Management Options for the Surgical Patient on Methadone and Buprenorphine. Curr Pain Headache Rep 20, 16 (2016). https://doi.org/10.1007/s11916-016-0549-9
Published:
DOI: https://doi.org/10.1007/s11916-016-0549-9