
Abstract
Chronic traumatic encephalopathy (CTE) is a progressive neurodegenerative disease that occurs in association with repetitive mild traumatic brain injury. It is associated with a variety of clinical symptoms in multiple domains, and there is a distinct pattern of pathological changes. The abnormal tau pathology in CTE occurs uniquely in those regions of the brain that are likely most susceptible to stress concentration during trauma. CTE has been associated with a variety of types of repetitive head trauma, most frequently contact sports. In cases published to date, the mean length of exposure to repetitive head trauma was 15.4 years. The clinical symptoms of the disease began after a mean latency of 14.5 years with a mean age of death of 59.3 years. Most subjects had a reported history of concussions with a mean of 20.3. However, 16 % of published CTE subjects did not have a history of concussion suggesting that subconcussive hits are sufficient to lead to the development of CTE. Overall, the number of years of exposure, not the number of concussions, was significantly associated with worse tau pathology in CTE. This suggests that it is the chronic and repetitive nature of head trauma, irrespective of concussive symptoms, that is the most important driver of disease. CTE and exposure to repetitive head trauma is also associated with a variety of other neurodegenerations, including Alzheimer disease. In fact, amyloid β peptide deposition is altered and accelerated in CTE and is associated with worse disease. Here, we review the current exposure, clinical, and pathological associations of CTE.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Chronic traumatic encephalopathy is a neurodegenerative disease associated with a prolonged period of repetitive mild traumatic brain injury (RTBI). The clinical symptoms of chronic traumatic encephalopathy (CTE) were first described nearly a century ago in boxers, and the disease was originally known as “punch drunk” or “dementia pugilistica” [1]. The clinical features of CTE are varied and typically manifest years or decades after the initial RTBI. The symptoms consist of impairments in mood (depression, suicidality, irritability), behavior (explosivity, violence, impulsivity), cognition (impaired memory, executive dysfunction, diminished concentration), and motor functioning (parkinsonism, dysarthria, gait changes, weakness) [2–4]. Clinical subtypes of CTE have been described in a retrospective study of autopsy-confirmed cases [4] and in a systematic review of possible and probable cases [5]. Based on these findings and others, clinical research criteria have been proposed [2, 6, 7]. Studies designed to establish the reliability and diagnostic accuracy of these clinical criteria in predicting the underlying pathology of CTE are underway. However, thus far, CTE can only be diagnosed at autopsy.
Pathologically, there is a constellation of findings in CTE. The gross findings include atrophy of the cerebral cortex, often greatest in the frontal and temporal lobes, loss of white matter volume, including thinning of the corpus callosum, ventriculomegaly, and cavum Vergae and fenestrated septum pellucidum. Microscopically, there is an accumulation of hyperphosphorylated tau within neurons, glia, and processes in a distinctive pattern. Abnormal tau accumulates within neurons, astrocytes, and cell processes in an irregular and patchy distribution that is perivascular and concentrated within the depths of sulci. In addition, the superficial cortical layers (I–II) are preferentially involved compared to the deeper layers. This unique pattern of tau pathology (i.e., the sulcal depths, around blood vessels, and superficial layers of cortex) is likely a result of force concentration during traumatic injury [8].
Recently, the US National Institute of Neurological Disorders and Stroke convened a panel of expert neuropathologists to establish consensus criteria for the pathological diagnosis of CTE [9]. It was determined that the pathognomonic lesion in CTE was an abnormal perivascular accumulation of tau in neurons, astrocytes, and cell processes in an irregular pattern at the depths of the cortical sulci that could be reliably distinguished from other tauopathies including Alzheimer disease (AD), progressive supranuclear palsy, argyrophilic grain disease, corticobasal degeneration, Guamanian parkinsonism-dementia complex, and primary age-related tauopathy [10] (http://www.ninds.nih.gov/research/tbi/ReportFirstNIHConsensusConference.htm). In addition, the pattern of tau pathology in CTE was clearly distinct from the tau deposition that occurs with aging [11].
Pathological Stages of CTE
As with most neurodegenerative pathologies, there appears to be a progression of tau pathology in CTE. The CTE program at Boston University has the world’s largest postmortem cohort of subjects with CTE. In 2013, 68 subjects were examined and four distinct stages of CTE were described defined by the extent of tau pathology [12••]. Stage I CTE was characterized by isolated perivascular foci of hyperphosphorylated tau within neurons, astrocytes, and cell processes present at the sulcal depths primarily restricted to the frontal lobe. In stage II, the tau pathology extended to involve the superficial cortical layers into the adjacent gyral crests and involves additional foci in the frontal and parietal lobes. In stage III, there was additional involvement of the temporal cortex as well as medial temporal lobe tau pathology (i.e., hippocampus, amygdala, entorhinal cortex). By stage IV, all cortical lobes were involved with severe tau pathology though it was still most severe at the sulcal depths and around blood vessels. In addition, there was abnormal tau accumulation within the diencephalon, brainstem, and cerebellum (reviewed in [13]).
Exposure to RTBI in CTE
Many contact sports have now been linked to CTE, including American football, boxing, hockey, soccer, and rugby. The epidemiology of CTE is not yet clear due to the inability to diagnose it during life. However, former National Football League (NFL) players over 50 years old are five times more likely to have dementia than the national average for men in that age group [14], and mortality due to neurodegenerative disease is increased threefold [15]. Of those former NFL players who have died and donated their brains to research, the percentage of players who have pathologically confirmed CTE is remarkably high (>90 %, pers. observation). In addition, CTE has been found in military personnel exposed to an explosive blast [16, 17]. Hundreds of thousands of soldiers have suffered brain trauma from conventional and improvised explosive devices in Iraq and Afghanistan [18, 19] and may be at risk of developing this disease. While many individuals with CTE who played contact sports or served in the military had a history of repeated concussions, some did not, suggesting that not only repetitive concussions but also multiple subconcussive blows to the head may induce this disease.
Concussions and Subconcussions
In cases that come to autopsy within 6 months of a concussion, there is multifocal axonal injury that can occur in the cerebrum, cerebellum, and brainstem that is often associated with neuroinflammation, including increased microglia and reactive astrocytes [20–22]. Similar pathology is found in military veterans exposed to blast injury [16, 23]. This axonal injury and inflammatory response is markedly perivascular (reviewed in [22]). In addition, in a subset of subjects exposed to blast injury (four of six) examined at the BU CTE Program, there was perivascular accumulation of phosphorylated tau [22]. This perivascular distribution of pathologies and accumulation of abnormal tau after blast exposure is strikingly reminiscent of the pathology seen in CTE years after impact injury. Whether the presence of perivascular tau after blast is related directly to blast exposure, a consequence of previous injury, or a consequence of impact injury secondary to the blast is not known [12••].
The association of concussions with CTE has not been rigorously studied. While it is clear that a single concussion is not sufficient to lead to CTE, the precise threshold, if present, is unknown and likely varies depending on the severity of the injury and between individuals. In the published cases with concussion data, the majority of subjects with CTE have a reported history of concussion (84 %, n = 92). The mean number of concussions was 17.0 (SEM = 3.4, range = 0–200; n = 92; Table 1) overall and was 20.3 (SEM = 3.9, range = 1–200; n = 77) in those CTE subjects whose family members endorsed concussion [24••]. The large number of concussions found in the majority of individuals with CTE suggests that multiple concussions are associated with this disease. However, there is great variability in the reported number of concussions, and subjective estimates may not correlate with the degree of RTBI exposure. Indeed, concussion is not always well defined and not always recognized. When given the current definition of concussion [25], athletes will significantly increase the number of self-reported concussions [26]. Moreover, given the nature of a brain bank there is a retrospective bias as well as a reliance on recall information from family members, which may lead to erroneous numbers. Large prospective studies with clearly defined parameters for diagnosing concussion and follow-up pathological diagnoses or a yet to be developed in vivo diagnostic test will be necessary to firmly establish the association between concussions and CTE.
Many head impacts do not result in a recognized concussion and may not be associated with any symptoms. Such injuries are considered “subconcussive” injuries and can be substantial in some sports. For instance, it has been reported that an offensive lineman in American football can experience over 1000 subconcussive hits over the level of 10g in the course of a single collegiate season [27]. NCAA Division I collegiate offensive linemen develop more postimpact symptoms than other playing positions but do not report these symptoms as a concussion, suggesting that offensive linemen experience more subconcussive injury compared to other positions [28]. A recent study of collegiate football players compared to healthy controls showed decreased hippocampal volume as well as slower reaction times regardless of concussion history but inversely related to the number of years played [29]. Other imaging studies have shown biochemical and cerebral blood flow abnormalities in contact sport athletes without a history of concussion. For instance, magnetic resonance spectroscopy demonstrated increases in choline, a putative marker of membrane turnover, and myo-inositol, a marker of glial activation, in former professional soccer players without a history of concussion [30]. In addition, a study of high school American football players showed alterations in neurochemistry with MR spectroscopy after a single season of play despite no documented concussions [31]. High school football players also showed alterations in cerebral blood flow that persisted postseason although no abnormalities in cognition were detected and any potential functional consequences of these alterations are unknown [32, 33]. Neuropsychological studies following a period of subconcussive injury in soccer have shown mixed results with some studies showing deficits [34–36] and others not [37–39].
Repetitive subconcussive injury can lead to the development of CTE. Despite a history of contact sports play and head impacts, symptoms associated with concussion are not always endorsed in subjects with CTE. In 16 % of subjects diagnosed postmortem with CTE, next-of-kin reported no concussions, suggesting that subconcussive head injury can be sufficient for development of disease. In our reported series of 92 cases of CTE [24••], multiple linear regression analysis demonstrated that CTE tauopathy stage was significantly predicted by years of contact sports play (β = 0.252, p = 0.005) and age (β = 0.505, p < 0.001), but not the number of concussions (β = 0.096, p = 0.284) or history of substance abuse (β = −0.111, p = 0.223). This suggests that a prolonged period of subconcussive head injury drives the progressive development of CTE tau pathology. It further suggests that the recognition of concussion, while important, is not sufficient for properly identifying individuals at risk for CTE.
Clinical Implications
The clinical symptoms of CTE typically develop many years after a period of exposure to head injury. Within the published cases of neuropathologically confirmed CTE [24••, 40], the mean age at onset was 44.3 years (SEM = 1.5, range = 16–83 years, n = 119). On average, the onset of clinical symptoms occurred 14.5 years after retirement (SEM = 1.6, n = 104), although 22 % were symptomatic at the time of retirement. The clinical course was protracted (mean duration = 15.0 years, SEM = 1.2, n = 125). Many subjects with CTE died of suicide or other causes, but approximately 45 % developed dementia (Table 1). Of those subjects over age 60, 66 % developed dementia.
Exposure Measures
Among the published cases of neuropathologically confirmed CTE, the mean length of exposure to contact sports or military service was 15.4 years (SEM = 0.5, n = 138). Interestingly, boxers and football players had similar levels of exposure (boxing: mean = 15.6 years, SEM = 1.3, n = 35; football: mean = 15.3 years, SEM = 0.6, n = 89) while hockey players had significantly more (mean = 23.9 years, SEM = 2.5, n = 4, p = 0.037, t test) and military service veterans with CTE had significantly less (mean = 6.3 years, SEM = 2.8, n = 4, p = 0.043). This may reflect that hockey players begin play at an earlier age in general or that the overall degree of RTBI exposure per year is less than that experienced in boxing or American football. Boxers have a significantly longer course of disease (19.4 years, SEM = 2.1, n = 29) than football players (14.3 years, SEM = 1.5, n = 81, p = 0.05, t-test) although the average age of death is not different (boxers = 60.8 years, football = 60.1 years). In fact, symptoms tend to start earlier in boxers, although the difference is not significant.
Trauma and Alzheimer Disease
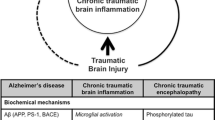
Several epidemiologic studies suggest moderate to severe TBI is a risk factor for Alzheimer disease [15, 41–43]. However, most reports linking TBI and AD have relied on a clinical diagnosis of probable AD without neuropathological verification and a definitive link has yet to be established [44]. It is unknown how repetitive mild TBI may affect the development of AD pathology. Following acute TBI, the amyloid precursor protein (APP) and amyloid β peptide (Aβ) increase in both tissue and CSF, and there can be rapid formation of diffuse Aβ plaques in the cortex [45]. Both APP and Aβ increase within damaged axons, and the release of Aβ into the surrounding tissue may be the basis for plaque formation [46].
Aβ in CTE
The role of Aβ in CTE has been controversial. At one point, Aβ deposition was thought to be a universal feature [47], but subsequent analyses found Aβ pathology within only a subset of individuals. In a cohort of 114 subjects with CTE, 52 % had deposition of Aβ as either diffuse or neuritic plaques, and 14 % met criteria for AD [24••]. When compared to an autopsy community cohort, the deposition of Aβ was altered and accelerated in CTE such that CTE subjects were overall 3.8-fold more likely to have Aβ plaques and developed them 10–15 years earlier. Moreover, when Aβ plaques were present in CTE, they were significantly associated with more severe tau and Lewy body pathology and worse clinical outcome independent of the effect of age [24••].
The degree of RTBI may influence Aβ deposition. CTE subjects with Aβ deposition had a greater reported number of concussions (mean = 24.2, SEM = 6.6, n = 41) than those without Aβ (mean = 11.5, SEM = 3.0, n = 48) though the difference was not significant (p = 0.071) [24••]. Boxers likely experience more head impacts than other sports and have more severe pathology when compared to football and hockey players and military veterans. Previous studies in boxers using anti-Aβ immunohistochemistry with formic acid pretreatment demonstrated diffuse cortical Aβ plaques in 27 of 28 (96.4 %) subjects [47, 48]. In the Boston University CTE cohort, the mean CTE tauopathy stage in boxers was significantly higher than that found in American football or hockey players and military veterans. The percentage of subjects with Aβ deposition was also highest in boxers (70 %) compared to football (51 %) or hockey (40 %) players and military service veterans (41 %) though the difference was not significant [24••].
Apolipoprotein E
Apolipoprotein E (Apo E) is involved in the transport of lipids, the maintenance of cell membrane and vascular integrity, and the clearance of Aβ [49]. There are three alleles (ε2, ε3, and ε4) that code for different isoforms. The APOE ε4 allele is a major risk factor for AD [50, 51] and is associated with increased Aβ levels following TBI [52]. Some studies in boxers [53] and professional football players [54] have demonstrated worse clinical outcomes among ε4 carriers. Other studies did not find an association between the ε4 allele and poor outcome after single mild to moderate TBI [55–57]. No association between the ε4 allele and the development of concussions was found in a prospective study of 822 collegiate athletes [58]. However, the G219T polymorphism in the APOE promoter region has been found to be associated with a history of concussions [59, 60].
Within CTE, an examination of the published cases showed no significant difference between the numbers of reported concussions in CTE subjects with an APOE ε4 allele (mean = 10.9, SEM = 4.4, n = 23) compared to those without ε4 (mean = 17.0, SEM = 5.6, n = 42, p = 0.393, t test). There was also no difference in the years of exposure between CTE subjects with ε4 (mean = 16.3, SEM = 1.3, n = 31) and those without ε4 (mean = 15.8, SEM = 0.9, n = 49). This suggests that APOE ε4 does not influence how long athletes with CTE play or how many concussions they experience. However, the APOE ε4 allele was significantly associated with Aβ deposition in CTE, and subjects with Aβ were worse pathologically and clinically compared to subjects without Aβ [24••]. Although Aβ-independent effects of the ε4 allele cannot be ruled out, it may be that the ε4 allele increases the likelihood of Aβ accumulation and deposition following RTBI and this, in turn, worsens the pathological and clinical outcomes.
Conclusions
Experiencing a few well-managed concussions is not sufficient for the development of CTE. However, experiencing many concussions over a lifetime—especially if they are not recognized or adequately treated—may be a risk factor for CTE. Indeed, continuing to play after a concussion may expose the injured brain to persistent subconcussive injury during a period of heightened vulnerability.
Independent of the number of concussions, the length of exposure to contact sports is strongly associated with more severe CTE pathology. Furthermore, 16 % of individuals with pathologically documented CTE had no history of concussion. This suggests that the chronicity and repetitive nature of impacts to the head, including subconcussive impacts, are key factors in CTE development. Further studies are needed to determine whether there are genetic modifiers of disease expression for a given amount of RTBI, such as the APOE ε4 allele. Future prospective studies utilizing accurate measures of the type and severity of head impacts together with in vivo biomarkers and postmortem neuropathological examination will be necessary to determine the prevalence and threshold of head injury exposure necessary for the development of CTE. In the meantime, awareness and prevention of both concussive and subconcussive impacts are crucial for the prevention of later neurodegeneration.
References
Papers of particular interest, published recently, have been highlighted as:•• Of major importance
Martland HS. Punch drunk. JAMA. 1928;91:1103–7.
Montenigro PH, Baugh CM, Daneshvar DH, Mez J, Budson AE, Au R, et al. Clinical subtypes of chronic traumatic encephalopathy: literature review and proposed research diagnostic criteria for traumatic encephalopathy syndrome. Alzheimer’s Res Ther. 2014;6:68.
Montenigro PH, Corp DT, Stein TD, Cantu RC, Stern RA. Chronic traumatic encephalopathy: historical origins and current perspective. Annu Rev Clin Psychol. 2015.
Stern RA, Daneshvar DH, Baugh CM, Seichepine DR, Montenigro PH, Riley DO, et al. Clinical presentation of chronic traumatic encephalopathy. Neurology. 2013;81:1122–9.
Montenigro PH, Baugh CM, Daneshvar DH, Mez J, Budson AE, Au R, et al. Clinical subtypes of chronic traumatic encephalopathy: literature review and proposed research diagnostic criteria for traumatic encephalopathy syndrome. Alzheimer’s Research & therapy. in press.
Victoroff J. Traumatic encephalopathy: review and provisional research diagnostic criteria. NeuroRehabilitation. 2013;32:211–24.
Jordan BD. The clinical spectrum of sport-related traumatic brain injury. Nature Publishing Group. Nature Publishing Group. 2013;9:222–30.
Smith DH, Chen XH, Xu BN, McIntosh TK, Gennarelli TA, Meaney DF. Characterization of diffuse axonal pathology and selective hippocampal damage following inertial brain trauma in the pig. J Neuropathol Exp Neurol. 1997;56:822–34.
Shen H. Researchers seek definition of head-trauma disorder. Nature. 2015;26:466–7.
Crary JF, Trojanowski JQ, Schneider JA, Abisambra JF, Abner EL, Alafuzoff I, et al. Primary age-related tauopathy (PART): a common pathology associated with human aging. Acta Neuropathol. 2014;128:755–66.
Braak H, Thal DR, Ghebremedhin E, Del Tredici K. Stages of the pathologic process in Alzheimer disease: age categories from 1 to 100 years. J Neuropathol Exp Neurol. 2011;70:960–9.
McKee AC, Stern RA, Nowinski CJ, Stein TD, Alvarez VE, Daneshvar DH, et al. The spectrum of disease in chronic traumatic encephalopathy. Brain. 2013;136:43–64. This study was the first to describe an exposure and age-dependent progression of tau pathology in CTE.
Stein TD, Alvarez VE, McKee AC. Chronic traumatic encephalopathy: a spectrum of neuropathological changes following repetitive brain trauma in athletes and military personnel. Alzheimer’s Res Ther. 2014;6:4.
Weir D, Jackson J. National Football League Player Care Foundation: study of retired NFL players. Institute for Social Research. 2009.
Lehman EJ, Hein MJ, Baron SL, Gersic CM. Neurodegenerative causes of death among retired National Football League players. Neurology. 2012;79:1970–4.
Goldstein LE, Fisher AM, Tagge CA, Zhang X-L, Velisek L, Sullivan JA, et al. Chronic traumatic encephalopathy in blast-exposed military veterans and a blast neurotrauma mouse model. Sci Transl Med. 2012;4:134–60.
McKee AC, Robinson ME. Military-related traumatic brain injury and neurodegeneration. Alzheimers Dement. 2014;10:S242–53.
TL T, LH J, editors. Invisible wounds of war: psychological and cognitive injuries, their consequences, and services to assist recovery [Internet]. Santa Monica, CA: RAND; 2008. Available from: http://www.rand.org/pubs/monographs/MG720.html.
Helmick KM, Spells CA, Malik SZ, Davies CA, Marion DW, Hinds SR. Traumatic brain injury in the US military: epidemiology and key clinical and research programs. Brain Imaging Behav. 2015.
Blumbergs PC, Scott G, Manavis J, Wainwright H, Simpson DA, McLean AJ. Staining of amyloid precursor protein to study axonal damage in mild head injury. Lancet. 1994;344:1055–6.
Oppenheimer DR. Microscopic lesions in the brain following head injury. J Neurol Neurosurg Psychiatr. 1968;31:299–306.
McKee AC, Daneshvar DH, Alvarez VE, Stein TD. The neuropathology of sport. Acta Neuropathol. 2014;127:29–51.
Ryu J, Horkayne-Szakaly I, Xu L, Pletnikova O, Leri F, Eberhart C, et al. The problem of axonal injury in the brains of veterans with histories of blast exposure. Acta Neuropathol Commun. 2014;2:153.
Stein TD, Montenigro PH, Alvarez VE, Xia W, Crary JF, Tripodis Y, et al. Beta-amyloid deposition in chronic traumatic encephalopathy. Acta Neuropathol. 2015;130:21–34. This study demonstrated an accelerated age-dependent deposition of Aβ in CTE and showed that CTE subjects with Aβ had worse pathology and clinical outcomes.
McCrory P, Meeuwisse W, Johnston K, Dvorak J, Aubry M, Molloy M, et al. Consensus statement on concussion in sport—the 3rd International Conference on concussion in sport, held in Zurich, November 2008. J Clin Neurosci. 2009. pp. 755–63.
Robbins CA, Daneshvar DH, Picano JD, Gavett BE, Baugh CM, Riley DO, et al. Self-reported concussion history: impact of providing a definition of concussion. Open Access J Sports Med. 2014;5:99–103.
Crisco JJ, Fiore R, Beckwith JG, Chu JJ, Brolinson PG, Duma S, et al. Frequency and location of head impact exposures in individual collegiate football players. J Athl Train. 2010;45:549–59.
Baugh CM, Kiernan PT, Kroshus E, Daneshvar DH, Montenigro PH, McKee AC, et al. Frequency of head-impact-related outcomes by position in NCAA Division I collegiate football players. J Neurotrauma. 2015;32:314–26.
Singh R, Meier TB, Kuplicki R, Savitz J, Mukai I, Cavanagh L, et al. Relationship of collegiate football experience and concussion with hippocampal volume and cognitive outcomes. JAMA. 2014;311:1883–8.
Koerte IK, Lin AP, Muehlmann M, Merugumala S, Liao H, Starr T, et al. Altered neurochemistry in former professional soccer players without a history of concussion. Journal of Neurotrauma. 2015.
Poole VN, Abbas K, Shenk TE, Breedlove EL, Breedlove KM, Robinson ME, et al. MR spectroscopic evidence of brain injury in the non-diagnosed collision sport athlete. Dev Neuropsychol. 2014;39:459–73.
Abbas K, Shenk TE, Poole VN, Breedlove EL, Leverenz LJ, Nauman EA, et al. Alteration of default mode network in high school football athletes due to repetitive subconcussive mild traumatic brain injury: a resting-state functional magnetic resonance imaging study. Brain Connect. 2015;5:91–101.
Nauman EA, Breedlove KM, Breedlove EL, Talavage TM, Robinson ME, Leverenz LJ. Post-season neurophysiological deficits assessed by ImPACT and fMRI in athletes competing in american football. Dev Neuropsychol. 2015;40:85–91.
Matser JT, Kessels AG, Lezak MD, Troost J. A dose-response relation of headers and concussions with cognitive impairment in professional soccer players. J Clin Exp Neuropsychol. 2001;23:770–4.
Witol AD, Webbe FM. Soccer heading frequency predicts neuropsychological deficits. Arch Clin Neuropsychol. 2003;18:397–417.
Zhang MR, Red SD, Lin AH, Patel SS, Sereno AB. Evidence of cognitive dysfunction after soccer playing with ball heading using a novel tablet-based approach. PLoS One. 2013;8, e57364.
Rutherford A, Stephens R, Potter D. The neuropsychology of heading and head trauma in Association Football (soccer): a review. Neuropsychol Rev. 2003;13:153–79.
Kontos AP, Dolese A, Elbin RJ, Covassin T, Warren BL. Relationship of soccer heading to computerized neurocognitive performance and symptoms among female and male youth soccer players. Brain Inj. 2011;25:1234–41.
Belanger HG, Vanderploeg RD, McAllister T. Subconcussive blows to the head: a formative review of short-term clinical outcomes. J Head Trauma Rehabil. 2015.
McKee AC, Cantu RC, Nowinski CJ, Hedley-Whyte ET, Gavett BE, Budson AE, et al. Chronic traumatic encephalopathy in athletes: progressive tauopathy after repetitive head injury. J Neuropathol Exp Neurol. 2009;68:709–35.
Heyman A, Wilkinson WE, Stafford JA, Helms MJ, Sigmon AH, Weinberg T. Alzheimer’s disease: a study of epidemiological aspects. Ann Neurol. 1984;15:335–41.
Mayeux R, Ottman R, Tang MX, Noboa-Bauza L, Marder K, Gurland B, et al. Genetic susceptibility and head injury as risk factors for Alzheimer’s disease among community-dwelling elderly persons and their first-degree relatives. Ann Neurol. 1993;33:494–501.
Plassman BL, Havlik RJ, Steffens DC, Helms MJ, Newman TN, Drosdick D, et al. Documented head injury in early adulthood and risk of Alzheimer’s disease and other dementias. Neurology. 2000;55:1158–66.
Johnson VE, Stewart W, Smith DH. Traumatic brain injury and amyloid-β pathology: a link to Alzheimer’s disease? Nat Rev Neurosci. 2010;11:361–70.
Ikonomovic MD, Uryu K, Abrahamson EE, Ciallella JR, Trojanowski JQ, Lee VMY, et al. Alzheimer’s pathology in human temporal cortex surgically excised after severe brain injury. Exp Neurol. 2004;190:192–203.
Smith DH, Chen X-H, Iwata A, Graham DI. Amyloid beta accumulation in axons after traumatic brain injury in humans. J Neurosurg. 2003;98:1072–7.
Roberts GW, Allsop D, Bruton C. The occult aftermath of boxing. J Neurol Neurosurg Psychiatr. 1990;53:373–8.
Tokuda T, Ikeda S, Yanagisawa N, Ihara Y, Glenner GG. Re-examination of ex-boxers’ brains using immunohistochemistry with antibodies to amyloid beta-protein and tau protein. Acta Neuropathol. 1991;82:280–5.
Yu J-T, Tan L, Hardy J. Apolipoprotein E in Alzheimer’s disease: an update. Annu Rev Neurosci. 2014;37:79–100.
Gandy S, DeKosky ST. APOE 4 status and traumatic brain injury on the gridiron or the battlefield. Sci Transl Med. 2012;4:134.
Mayeux R, Ottman R, Maestre G, Ngai C, Tang MX, Ginsberg H, et al. Synergistic effects of traumatic head injury and apolipoprotein-epsilon 4 in patients with Alzheimer’s disease. Neurology. 1995;45:555–7.
DeKosky ST, Abrahamson EE, Ciallella JR, Paljug WR, Wisniewski SR, Clark RSB, et al. Association of increased cortical soluble abeta42 levels with diffuse plaques after severe brain injury in humans. Arch Neurol. 2007;64:541–4.
Jordan BD, Relkin NR, Ravdin LD, Jacobs AR, Bennett A, Gandy S. Apolipoprotein E epsilon4 associated with chronic traumatic brain injury in boxing. JAMA. 1997;278:136–40.
Kutner KC, Erlanger DM, Tsai J, Jordan B, Relkin NR. Lower cognitive performance of older football players possessing apolipoprotein E epsilon4. Neurosurgery. 2000;47:651–7. discussion657–8.
Pruthi N, Chandramouli BA, Kuttappa TB, Rao SL, Subbakrishna DK, Abraham MP, et al. Apolipoprotein E polymorphism and outcome after mild to moderate traumatic brain injury: a study of patient population in India. Neurol India. 2010;58:264–9.
Chamelian L, Reis M, Feinstein A. Six-month recovery from mild to moderate traumatic brain injury: the role of APOE-epsilon4 allele. Brain. 2004;127:2621–8.
Moran LM, Taylor HG, Ganesalingam K, Gastier-Foster JM, Frick J, Bangert B, et al. Apolipoprotein E4 as a predictor of outcomes in pediatric mild traumatic brain injury. J Neurotrauma. 2009;26:1489–95.
Kristman VL, Tator CH, Kreiger N, Richards D, Mainwaring L, Jaglal S, et al. Does the apolipoprotein epsilon 4 allele predispose varsity athletes to concussion? A prospective cohort study. Clin J Sport Med. 2008;18:322–8.
Terrell TR, Bostick RM, Abramson R, Xie D, Barfield W, Cantu R, et al. APOE, APOE promoter, and Tau genotypes and risk for concussion in college athletes. Clin J Sport Med. 2008;18:10–7.
Tierney RT, Mansell JL, Higgins M, McDevitt JK, Toone N, Gaughan JP, et al. Apolipoprotein E genotype and concussion in college athletes. Clin J Sport Med. 2010;20:464–8.
Acknowledgments
We gratefully acknowledge the use of resources and facilities at the Edith Nourse Rogers Memorial Veterans Hospital (Bedford, MA) as well as all the individuals whose participation and contributions made this work possible. This work was supported by the Department of Veterans Affairs, Veterans Health Administration, Clinical Sciences Research and Development Merit Award; Alzheimer’s Association (NIRG-305779); National Institute of Neurological Disorders and Stroke, National Institute of Biomedical Imaging and Bioengineering (U01NS086659-01); National Institute of Aging Boston University AD Center (P30AG13846; supplement 0572063345-5); and Sports Legacy Institute. This work was also supported by unrestricted gifts from the Andlinger Foundation and WWE.
Compliance with Ethics Guidelines
ᅘ
Conflict of Interest
Thor D. Stein, Victor E. Alvarez, and Ann C. McKee each declare no potential conflicts of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Concussion and Head Injury
Rights and permissions
About this article

Cite this article
Stein, T.D., Alvarez, V.E. & McKee, A.C. Concussion in Chronic Traumatic Encephalopathy. Curr Pain Headache Rep 19, 47 (2015). https://doi.org/10.1007/s11916-015-0522-z
Published:
DOI: https://doi.org/10.1007/s11916-015-0522-z