
Abstract
Migraine and temporomandibular disorders (TMD) are highly prevalent conditions that frequently coexist in the same patient. The relationship between migraine and TMD is complex. Migraineurs often have pain in the TMD area; TMD sufferers, in turn, often experience headaches in addition to the pain in the jaw. Finally, migraine and TMD are comorbid, and the final phenotype of patients with the comorbidity may represent the aggregated contribution of both. Herein we briefly discuss the clinical commonalities of migraine and TMD, and the differential diagnosis of these conditions with other causes of facial pain. We close by presenting our experience in the treatment of patients with the comorbidity.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Headaches are the most prevalent neurological disorders, representing a major health problem worldwide [1, 2]. Among the headache syndromes, migraine affects around 12 % of adults in western Countries [2, 3]. Migraine is a disabling health condition, burdening the sufferer, their family and society [4].
Facial pain involving the muscles of mastication and temporomandibular joints (TMJs) is a typical feature of the temporomandibular disorders (TMDs), which is also accompanied by other symptoms and signs, including headache, TMJ sounds and deviation or restriction of mandibular range of motion. Like migraine, TMD is highly prevalent [5] and more common in women, particularly during their child-bearing years. Migraine headache affects 17-18 % of women and 6 % of men [2, 3]; while TMD affects up to 14 % of women and up to 10 % of men [6].
The relationship between migraine and TMD is complex from pathophysiological and clinical perspectives. From a clinical perspective, migraineurs often have pain in the TMD area, in addition to the headache [7–9]. TMD, in turn, is associated not only with pain in the jaw but also often with headache pain, a condition classified as headache attributed to TMJ disorders according to the Second Edition of the International Classification of Headache Disorders (ICHD-2) [10]. Additionally, migraine and TMD are comorbid [11–13], and the final phenotype of patients with the comorbidity may represent the aggregated contribution of migraine and TMD (therefore being enhanced and not fully representative of any of the conditions in isolation) [6, 9]. Finally, in individuals with migraine, TMD is a risk factor for increased headache frequency, and for the development of chronic migraine (CM) [14••, 15••, 16].
While the efficient treatment of patients with migraine and TMD requires a multidisciplinary approach, health providers should be prepared to identify and diagnose different painful syndromes after accounting for the presence of comorbidity. In many aspects, comorbidities force us to violate the medical principle of parsimony (by which we are trained to explain a myriad of symptoms as coming from a single disease). When comorbidity exists, diagnosing one disease indeed raises suspicion about another. Exploring this topic is the scope of this review. We first briefly discuss the clinical features of migraine and TMD. We then focus on the differential diagnosis of these conditions with other causes of facial pain. We end by presenting our experience in the treatment of patients with the comorbidity.
Diagnosing Migraine, TMD, and Headaches Attributed to TMD
Migraine and TMD are characterized by intermittent head and face pain and have internationally accepted criteria for diagnosis. They are both diagnoses of inclusion, in that specific features need to present to make the diagnosis, and diagnoses of exclusion, meaning that other disorders must be excluded before diagnosis are firmly established.
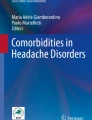
Migraines, as other headaches, are classified according to the criteria of the ICHD-2 [10]. To establish the diagnosis of migraine, five lifetime attacks with a combination of two of four pain features and nausea or photophobia and phonophobia are required. In addition, the headache cannot be attributed to another disorder. Accordingly, in patients with TMD and a phenotype of migraine, where there is a headache resolution after the treatment of TMD, the final diagnosis is not migraine, but headaches attributed to TMD. This phenotypical convergence and overlapping is sometimes difficult to navigate either by experienced providers. Nonetheless, the task can only be accomplished by obtaining detailed history and physical examination (including TMD assessment), and sometimes by the appropriate use of diagnostic tests or if another disorder is present, by the temporal dissociation between migraine and the other disorder.
TMDs are characterized by pain in the muscles of mastication, the TMJs, or both. In addition, pain on palpation and/or pain on jaw movement may be present. Signs often include joint sounds, such as clicking or crepitation, and limitations or deviation upon mandibular opening [5]. The relationship between dysfunction at the TMJs, muscle disorders (that cause the dysfunction or that arise as a consequence of the dysfunction), and pain are poorly understood [17]. There are two widely accepted diagnostic criteria for TMD; the Research Diagnostic Criteria for TMD (RDC/TMD) [18] and the criteria from the American Academy of Orofacial Pain (AAOP) [5]. Each system has advantages and disadvantages. The AAOP criteria are well suited for clinical use and for measuring treatment outcomes [5]. The RDC/TMD offers a classification system that has been extensively tested and is universally accepted for use in research. Both systems subdivide TMD into muscle disorders or articular disorders, with subcategories (Table 1).
It is worth emphasizing that while for migraine the physical exam serves primarily to exclude other disorders, for TMD, abnormalities are supportive of the diagnosis.
As mentioned, TMD may also cause a secondary headache. From an anatomical perspective, headache is the pain manifested above the orbitomeatal line [10]. It is common, in patients with TMD and headache, to reproduce the headache by moving the jaw or by pressing masticatory muscles [18]. Since the temporalis muscle is involved in mastication and is above the orbitomeatal line, it is not surprising that TMD may cause headaches [10]. In addition to the peripheral contribution of the temporalis muscle, it is well established that pain in the three branches of the trigeminal nerve may happen when the trigeminal nucleus caudalis is activated for any reason.
Nonetheless, the diagnosis of headache attributed to TMD requires headache of any characteristics accompanied by pain in areas related to TMD (e.g., muscle, jaw, TMJ); evidence of disorders on these structures (evidence of TMD); worsening of pain with TMJ movement; close temporal relation (headaches worsened in parallel to symptoms of TMD); and headache resolution within 3 months after successful treatment of the other condition [10]. The sensitivity and specificity of these criteria in differentiating headaches attributed to TMD from migraine in patients with TMD have not been established.
Although the syndromic definition of TMD or migraine is not difficult, nuances obviously exist, especially when both coexist in a single patient. As mentioned, before diagnosing TMD and/or migraine, other sources of pain should be excluded. According to the AAOP, there are several orofacial pain conditions to be considered during the diagnostic process as intracranial pain disorders (neoplasm, edema, etc.), neuropathic pain disorders (episodic neuralgias, continuous neuropathic pains, sympathetically maintained pain), intraoral pain disorders (dental, periodontium or soft tissue), cervical pain disorders, pain from associated structures (ears, eyes, nose, paranasal sinuses, throat, lymph nodes, salivary glands) [5]. Generalized musculoskeletal pain conditions can also be a source of orofacial pain. For example, fibromyalgia, a widespread pain that can also affect the masticatory muscles and are comorbid with TMD [19, 20••]. However, most of these disorders are easily excluded by the oral and facial careful exam, and by the careful semiology of pain characteristics (including aggravating and ameliorating factors).
TMD and Migraine: Possible Sources of Misdiagnosis
In this section we further explore the interrelationship between migraine and TMD from an anatomical and pathophysiological perspective.
Although migraine pain is often manifested in the area of the ophthalmic branch of the trigeminal nerve (V1), symptoms in the maxillary (V2) and mandibular (V3) areas may sometimes be prominent and explain sinus and TMD symptoms in migraineurs [9], and these symptoms are often relieved by sumatriptan, a specific migraine treatment [21]. They are also characterized by elevated calcitonin gene-related peptide (CGRP) levels in nasal secretion, which follows the same patterns seen in migraine pain [22]. The clinical implication is that, in migraineurs, pain in the V2 and V3 areas is common [7–9], and can be easily misinterpreted as TMD pain.
Additionally, during migraine attacks, allodynia (pain that happens when non-painful stimuli are applied) is a common symptom [23–26]. The prevalence is higher in chronic than in episodic migraine, and is very low in tension-type headache, therefore suggesting that facial allodynia is a fairly specific physiological marker of migraine [27]. Therefore, not only can migraine cause pain in the V2 and V3 areas, but it may cause allodynia, which is a source of discomfort and pain in trivial situations, and is often misdiagnosed as TMD. Although the relationship between facial pain and allodynia is still little explored, previous studies reported increased sensitivity on masticatory and pericranial muscles during migraine attacks [7, 8, 28, 29, 30•], including pressure allodynia as measured by algometry [31].
Since most physicians are unlikely to see their patients during a migraine attack, they may be able to elicit a history of increased skin sensitivity through relevant questioning that inquires whether activities such as brushing hair, touching the scalp, shaving, and wearing glasses, contact lenses, earrings, or wearing tight clothes hurt patients during migraine attacks [32]. Nonetheless, the key message is that symptoms suggestive of TMD may reflect migraine (pain and allodynia); and symptoms suggestive of migraine may reflect TMD. Therefore, symptoms of TMD must be assessed when patients do not have headache and formal diagnostic criteria must be fulfilled before assigning the diagnosis.
The Treatment of Patients with Migraine and TMD: Personal Experience
Effective treatments for migraine and therapies for TMD exist and have been extensively published. Reviewing them in detail is outside the scope of this paper and certainly unnecessary for the reader of this journal. Nonetheless, the best approach for patients with both disorders is a point of controversy. Should one be treated first (and if so, which), or is treating both necessary?
In order to disentangle the best treatment for patients with migraine and TMD, we conducted a four-arm, randomized, double-blind, controlled trial [33•]. All patients had migraine according to the ICHD-2 and TMD according to the RDC/TMD - Axis I. Primary endpoint was change in headache days from baseline and secondary endpoint was change in days with at least moderate headache from baseline. Migraine-related disability was evaluated using the “Migraine Disability Assessment Test” (MIDAS) [34]. Frequency and intensity of pain were assessed using daily headache calendars. TMD parameters as intensity [visual analogical scale (VAS)] and grade of TMD chronic pain (RDC/TMD – Axis II) were also obtained.
The sample consisted of 89 women with both conditions. They were randomized to receive one of four treatments: (1) Group I: propranolol 30 mg/day (tid) and stabilization splints (SS) [35]. Propranolol was started at the dose of 30 mg/day (qd) and dose was increased to 30 mg bid in the second week and 30 mg tid from the third week; (2) Group 2: propranolol and non-occlusal (placebo) splint (NOS); (3) Group III: placebo and SS; (4) Group IV: placebo and NOS. Evaluations were made at baseline, at the end of the blinded-phase (3 months) and at the end of the open extension (6 months).
We independently assessed migraine improvement and TMD improvement. For reduction of headache days at 3 months (primary endpoint) treating both conditions yielded significantly better results (−5.4 days) relative to other groups (propranolol only: -3.2; occlusal splints only: -4.1 and placebo: -3.5; P < 0.05). For the secondary endpoint, differences were also significant after 3 months of treatment (P = 0.011) with those treating both conditions having additional benefits relative to all other groups. As for disability, those treating both conditions also had significant improvements relative to all other groups (P = 0.016). Data are summarized in Table 2. Figure 1 illustrates the monthly headache frequency as a function of treatment group, at the blinded and open-extension phase. Differences were significant at 2, 3, 5 and 6 months.

Average frequency of headache according to the treatment group at baseline and after 1–6 months of treatment. SS stabilization occlusal splint, NOS nonocclusal splint (placebo)
For TMD assessments, treatment groups yielded virtually identical results at 3 and 6 months. No separation from placebo was seen. All groups presented a reduction of facial pain average from baseline, but significant differences were not found. Nonetheless, 48.3 % of completers were classified as Grade I or no TMD chronic pain at the end of treatment (Table 2).
Our findings suggested that in patients with the comorbidity, best migraine outcomes happen when the TMD is also treated. For TMD, all groups yielded improvement but no differences were seen across groups. The clinical message is optimistic nonetheless, since treating both conditions will translate into optimal migraine improvement and meaningful TMD improvement.
Conclusions
In patients presenting facial pain and headache, standard criteria should be applied for a precise differential diagnosis, since comorbidity of TMD and migraine is frequent as well an overlapping on its signs and symptoms. When TMD and migraine are simultaneously present, better outcomes will be achieved by the concomitant treatment.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Jensen R, Stovner LJ. Epidemiology and comorbidity of headache. Lancet Neurol. 2008;7:354–61.
Stovner Lj, Hagen K, Jensen R, et al. The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia. 2007;27(3):193–210.
Silberstein S, Loder E, Diamond S, Reed ML, AMPP Advisory Group, et al. Probable migraine in the United States: results of the American Migraine Prevalence and Prevention (AMPP) study. Cephalalgia. 2007;27(3):220–34.
World Health Organization. The global burden of disease: 2004 Update. Available at: http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf. Accessed February 2012.
De Leeuw R. Temporomandibular Disorders. In: De Leeuw R, editor. Orofacial pain: guidelines for assessment, diagnoses and management. Hanover Park: Quintessence Publishing; 2008. p. 129–204.
DeRossi SS, Stoopler ET, Sollecito TP. Temporomandibular disorders and migraine headache: comorbid conditions? The Internet Journal of Dental Science 2005, Volume 2, Number 1. http://www.ispub.com.
Tfelt-Hansen P, Lous I, Olesen J. Prevalence and significance of muscle tenderness during common migraine attacks. Headache. 1981;21(2):49–54.
Jensen R, Rasmussen BK, Pedersen B, Olesen J. Muscle tenderness and pressure pain thresholds in headache. A population study. Pain. 1993;52(2):193–9.
Cady R. The convergence hypothesis. Headache. 2007;47 Suppl 1:S44–51.
Headache Classification Subcommittee of the International Headache Society: The International Classification of Headache Disorders, 2nd ed. Cephalalgia 2004, Volume 24 Supplement 1.
Gonçalves DA, Bigal ME, Jales LC, Camparis CM, Speciali JG. Headache and symptoms of temporomandibular disorder: an epidemiological study. Headache. 2010;50(2):231–41.
Franco AL, Gonçalves DA, Castanharo SM, et al. Migraine is the most prevalent primary headache in individuals with temporomandibular disorders. J Orofac Pain. 2010;24(3):287–92.
Stuginski-Barbosa J, Macedo HR, Bigal ME, Speciali JG. Signs of temporomandibular disorders in migraine patients: a prospective, controlled study. Clin J Pain. 2010;26(5):418–21.
•• Bevilaqua-Grossi D, Lipton R, Bigal ME. Temporomandibular disorders and migraine chronification. Curr Pain Headache Rep. 2009;13:314–8. This paper discusses interesting hypotheses about the influence of TMD on migraine chronification and point for the relevance of the simultaneous treatment of both.
•• Gonçalves DA, Speciali JG, Jales LC, Camparis CM, Bigal ME. Temporomandibular symptoms, migraine, and chronic daily headaches in the population. Neurology. 2009;73(8):645–6. This paper points to the relevance of TMD on migraine chronification based on a population epidemiological data.
Gonçalves DA, Camparis CM, Speciali JG, et al. Temporomandibular disorders are differentially associated with headache diagnoses: a controlled study. Clin J Pain. 2011;27(7):611–5.
LeResche L, Mancl LA, Drangsholt MT, Huang G, Von Korff M. Predictors of onset of facial pain and temporomandibular disorders in early adolescence. Pain. 2007;129(3):269–78.
Dworkin SF, LeResche L. Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord. 1992;6(4):301–55.
Hoffmann RG, Kotchen JM, Kotchen TA, et al. Temporomandibular disorders and associated clinical comorbidities. Clin J Pain. 2011;27(3):268–74.
•• Woolf CJ. Central sensitization: implications for the diagnosis and treatment of pain. Pain. 2011;152(3 Suppl):S2–S15. This paper discusses the importance of central sensitization on different pain conditions and the pathophysiological mechanisms of the comorbidity with great implication on clinical practice.
Cady RK, Schreiber CP. Sinus headache: a clinical conundrum. Otolaryngol Clin North Am. 2004;37:267–88.
Bellamy JL, Cady RK, Durham PL. Salivary levels of CGRP and VIP in rhinosinusitis and migraine patients. Headache. 2006;46:24–33.
Burstein R, Jakubowski M. Analgesic triptan action in an animal model of intracranial pain: a race against the development of central sensitization. Ann Neurol. 2004;55:27–36.
Burstein R, Collins B, Jakubowski M. Defeating migraine pain with triptans: a race against the development of cutaneous allodynia. Ann Neurol. 2004;55:19–26.
Merskey H, Bogduk N. Classification of chronic pain. 2nd ed. Seattle: IASP Press; 1994, p. 240.
Lipton RB, Bigal ME, Ashina S, et al. Cutaneous allodynia in the migraine population. Ann Neurol. 2008;63(2):148–58.
Bigal ME, Lipton RB. Clinical course in migraine: conceptualizing migraine transformation. Neurology. 2008;71(11):848–55.
Lous I, Olesen J. Evaluation of pericranial tenderness and oral function in patients with common migraine, muscle contraction headache and ‘combination headache’. Pain. 1982;12(4):385–93.
Jensen R, Bendtsen L, Olesen J. Muscular factors are of importance in tension-type headache. Headache. 1998;38(1):10–7.
• Bevilaqua-Grossi D, Lipton RB, Napchan U, et al. Temporomandibular disorders and cutaneous allodynia are associated in individuals with migraine. Cephalalgia. 2010;30(4):425–32. This paper shows the interaction of migraine, TMD, and allodynia and discusses an interesting hypothesis for shared mechanisms involved in TMD and migraine.
Smith R, Hasse LA, Vonder Meulen MB. Scalp and forearm tenderness during the different phases of the migraine cycle. Headache Care. 2004;2:15–22.
Burstein R, Yarnitsky D, Goor-Aryeh I, Ransil BJ, Bajwa ZH. An association between migraine and cutaneous allodynia. Ann Neurol. 2000;47(5):614–24.
• Gonçalves DAG, Camparis CM, Speciali JG, et al. Migraine and temporomandibular disorders: a 4-arm, double-blind, randomized, placebo-controlled pilot study. Data in preparation. This was the first randomized, blinded, and controlled study to test best treatment for patients with migraine. Migraine improved best when TMD was also treated.
Lipton RB, Stewart WF. The Migraine Disability Assessment Test. Available on: http://uhs.berkeley.edu/home/healthtopics/pdf/assessment.pdf. Accessed on February 2012.
Ash MM, Ramfjord SP. An introduction to functional occlusion: a workshop and guide for the study of articulators, diagnostic waxing, and occlusal bite plane splints. Philadelphia: WB Saunders; 1982.
Disclosures
D. A. G. Gonçalves: none; C. M. Camparis: none; A. L. Franco: none; G. Fernandes: none; J. G. Speciali: none. Marcelo E. Bigal is an employee of Merck & Co., and holds stock interest in the company.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gonçalves, D.A.G., Camparis, C.M., Franco, A.L. et al. How to Investigate and Treat: Migraine in Patients with Temporomandibular Disorders. Curr Pain Headache Rep 16, 359–364 (2012). https://doi.org/10.1007/s11916-012-0268-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11916-012-0268-9