
Abstract
Primary cough headache, primary exertional headache, primary sexual headache, and idiopathic stabbing headache are included in “Other Primary Headaches” (Group 4) in the International Classification of Headache Disorders, 2nd edition (ICHD-II). Headaches provoked by cough, exertion, and sex have different age distributions, but they do share some clinical and pathogenic characteristics. The triggering activities frequently involve Valsalva-like maneuvers, which may explain part of the pathogenesis. Primary stabbing headache is common and characterized by ultra-short stabbing headaches. All these headache disorders respond well to indomethacin, and they are commonly comorbid with migraine except for primary cough headache. Of note, some patients with sexual headache had reversible cerebral vasoconstriction syndromes. Recent large-scaled studies have revealed that the ICHD-II criteria of these four headache disorders cannot be completely fulfilled. Further revisions for the ICHD-II criteria are required based on these results of the evidence-based studies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
It has been recognized for decades that headaches can occur during exertion, cough, and sexual activities [1]. These headache disorders share many pathophysiologic and clinical characteristics. Provoking activities frequently involve a Valsalva-like maneuver [2]. Some patients have more than one of the above headache triggers. All these headache disorders frequently respond to indomethacin [3]. Most importantly, these headache disorders can be divided into idiopathic or symptomatic. Therefore, investigation of secondary causes is mandatory for patients with these headaches.
Primary stabbing headache (PSH) is characterized by transient, sharp jabbing pains that occur within a small, localized area of the scalp [4, 5]. Many terms have been used in the literature to describe the symptoms of stabbing headache, including “ice pick-like pains,” “sharp short-lived head pains,” “needle-in-the-eye syndrome,” and “jabs and jolts syndrome” [4–6]. PSH is common, and almost all of them are idiopathic. It also responds to indomethacin [3].
The International Classification of Headache Disorders, 2nd edition (ICHD-II) includes all these four headache disorders in Group 4, “Other Primary Headaches” [7]. The pathogenesis of these headache disorders is still poorly understood, and relevant studies are limited. The diagnostic criteria proposed by ICHD-II need further validation. In recent years, several large-scaled community-based or clinic-based studies [8••, 9••, 10, 11••, 12–15••] were published, which provide us an opportunity to revisit these headache disorders.
Epidemiology
Table 1 shows the prevalence and the clinical characteristics of the four primary headache disorders discussed in this article.
Primary Cough Headache
One earlier cross-sectional epidemiologic study found the lifetime prevalence of primary cough headache (PCH) to be about 1% [16]. Three recent studies showed about 0.4–1% of headache patients consulted a medical clinic because of cough headache [8••, 9••, 17]. The frequency of secondary cough headache patients is lower in Asians than in Westerners (10.8% vs 58.8%, respectively). Because the most common secondary causes of cough headache are Chiari malformation type I and posterior fossa lesion [8••, 9••], the lower prevalence of Chiari malformation type I in Asians may account for this discrepancy [9••]. PCH is more prevalent in men [1, 8••, 9••] and usually occurs later than 40 years of age [1, 8••, 9••].
Primary Exertional Headache
One earlier population-based study estimated the prevalence of primary exertional headache (EH) at about 1% [16]. The later Vågå study found that the prevalence of EH in adults was 12.3% [10], whereas a recent report on Taiwanese adolescences found a prevalence of 30.4% [11••]. The discrepancies in the reported prevalence might be due to recall bias of early life experiences and being less physically active in adults. A trend of decreasing prevalence with increasing age was disclosed in the adolescent study [11••], and the age of onset was usually younger than 30 years old in the Vågå study [10]. These two large-scaled studies both found a female predominance, in contrast to the finding of significant male preponderance in previous hospital-based studies [1, 18]. EH accounted for about 5.3% of patients in a headache clinic in Turkey [17].
Primary Headache Associated with Sexual Activity
Only population-based study has reported the lifetime prevalence of headache associated with sexual activity (HSA) to be about 1% [16]. Two clinic-based studies reported that HSA accounted for 1% of all patients [13, 17]. More men than women have this disorder, with a ratio of 3 to 4:1 [13, 19, 20•, 21]. The mean age of onset was between the 30th and 40th years of life [13, 19, 20•, 21]. Orgasmic headache was the most common subtype [13, 20•].
Primary Stabbing Headache
One earlier population study based on personal examination estimated the prevalence of PSH to be 2% [16]. However, one large-scale population study evaluating the prevalence of PSH reported 35.2% of the 18 to 65-year-old subjects were found to have such jabs [14]. The overall prevalence of PSH was higher among women, with a female-to-male ratio in the range of 1.5 to 2.3 [14, 15••]. The mean age of onset was around 28 years in the community-based study [14] and 48 years old in the clinic-based study [15••]. Most of the patients had low frequencies of attacks, so they seldom visited a doctor. The prevalence of PSH was about 13% in Taiwan and Turkey headache clinics [14, 17]. The high prevalence might be due to the lack of a referral system in Taiwan.
Clinical Characteristics and ICHD-II Diagnosis
Primary Cough Headache
PCH represents the headache provoked by cough without any intracranial disorder. The diagnostic criteria for PCH proposed by the ICHD-II include the following [7]:
-
A)
Headache fulfilling criteria B and C
-
B)
Sudden onset, lasting from 1 s to 30 min
-
C)
Brought on by and occurring only in association with coughing, straining, and/or Valsalva maneuver
-
D)
Not attributed to another disorder
PCH is moderate to severe in intensity with mostly explosive or dull pain at onset but could be pulsatile, stabbing, or sharp sometimes. The duration of headache is usually short-lasting. However, different from the ICHD-II criteria, as recently reported 10.8% of PCH patients had headache durations of more than 30 min [9••]. Most patients suffered headaches bilaterally, located usually in the occipital but also in the frontal, temporal, or vertex area. Associated features, such as nausea, vomiting, photophobia, and phonophobia, were uncommon. Besides cough, many patients had other triggers for their headaches, including straining at stool, bending down, heavy lifting, Valsalva maneuver, laughing, sneezing, crying, exertion, and sexual activity [1, 8••, 9••]. The exertion and heavy lifting were less common in PCH patients than those with secondary etiologies [9••].
Primary Exertional Headache
The definition of “exertion” was imprecise historically [1, 18]. Some used the term EH to describe headaches precipitated mainly by Valsalva-like maneuvers, which had a prompt mode of onset and lasted for seconds to minutes [18]; others specifically referred to EH as headaches that occurred during or after sustained physical exercise, which tended to be less abrupt in onset and would last longer [1]. There hasn’t been a unified consensus, but both the ICHD-II criteria [7] and two large epidemiological studies [10, 11••] adopted the latter one.
The diagnostic criteria in the ICHD-II for primary EH include the following [7]:
-
A)
Pulsating headache fulfilling criteria B and C
-
B)
Lasting from 5 min to 48 h
-
C)
Brought on by and occurring only during or after physical exertion
-
D)
Not attributed to another disorder
Exertional headaches are commonly bilateral, pulsating, and short-lasting; however, these characteristics are not invariable. The ICHD-II criteria are simple but might not be exhaustive in diagnosing EH, especially in adolescents. Criterion A necessitates a “pulsating” headache, which could be found in 87% of EH sufferers in the Vågå study [12] but only disclosed in 59% of adolescent patients [11••]. In addition, the duration of EH was less than 5 min in 46% of adolescent sufferers, making criterion B less applicable. Further revision of the ICHD criteria is required to cover the possible implicit characteristics of EH in adolescents such as nonpulsating and shorter headache duration [22].
Comorbidity with migraine is quite common in EH. The Vågå study found that 46% of patients had both EH and migraine [10]. The Taiwan adolescent headache study also found that 48% of migraineurs had EH [11••]. Subjects who have comorbid migraine would have EH bearing more migrainous features [11••].
Primary Headache Associated with Sexual Activity
Primary sexual headache was previously called benign orgasmic cephalgia, benign coital headache, or benign sexual headache [19, 23, 24]. The ICHD-II uses the term primary HSA [7] because these headaches are not only precipitated during sexual intercourse or orgasm, but also because similar headaches can occur during masturbation and nocturnal emission [24]. Even though a secondary cause is less common (7–11%) for HSA, it is mandatory to exclude possible underlying causes, such as subarachnoid hemorrhage [1, 8••].
The typical pain of HSA is bilateral and occipital, usually lasting from 10 min to 6 h [13]. These headaches are occasionally associated with nausea, vomiting, and mood disturbance [13]. Comorbidity with other primary headaches, such as migraine, benign exertional headache, and tension-type headache, is common [13, 21]. The ICHD-II proposed the diagnostic criteria for two subtypes of HSA: preorgasmic headache (4.4.1) and orgasmic headache (4.4.2) [7].
Preorgasmic Headache (4.4.1)
-
A)
Dull ache in the head and neck associated with awareness of neck and/or jaw muscle contraction and fulfilling criterion B
-
B)
Occurs during sexual activity and increases with sexual excitement
-
C)
Not attributed to another disorder
Orgasmic Headache (4.4.2)
-
A)
Sudden severe (‘explosive’) headache fulfilling criterion B
-
B)
Occurs at orgasm
-
C)
Not attributed to another disorder
However, the only comparative study between the two subtypes found no significant differences in demographics, clinical features, comorbidities, and prognosis, except for the mode of headache onset [13, 20•]. It is believed that they are different manifestations of the same disorder [13]. HSA is also commonly associated with migraine. The prevalence varied from 19% to 47% [13, 25, 26].
Primary Stabbing Headache
The ICHD-II diagnostic criteria for PSH are as follows [7]:
-
A)
Head pain occurring as a single stab or a series of stabs
-
B)
Exclusively or predominantly felt in the distribution of the first division of the trigeminal nerve (orbit, temple, and parietal area)
-
C)
Stabs last for up to a few seconds and recur with irregular frequency, ranging from one to many per day
-
D)
No accompanying symptoms
-
E)
Not attributed to another disorders
Nevertheless, one recent large-scaled study found the pain was most frequently localized posteriorly, especially in the occipital and nuchal areas (58%), followed by parietal (49%) [15••]. Only 30% patients fulfilled criterion B of the ICHD-II criteria proposed for PSH, in which the pain is “exclusively or predominantly in the distribution of the first division of the trigeminal nerve.” About 15% patients could not fulfill criterion C of the ICHD-II criteria proposed for PSH, in which patients should have “no accompanying symptoms.”
Most PSH patients have very brief attacks (<3 s). Nevertheless, long-lasting cephalic jabs had been reported [27]. Clinic-based studies showed PSH occurred more often in migraineurs [5, 6, 15••]. One patient with a past history of migraine reported PSH occurring associated with monocular visual loss with scintillating scotoma [28].
Pathophysiology
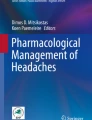
The pathophysiology of all these headache disorders is still unclear. It has been proposed that the transient increase of intracranial hypertension due to Valsalva maneuver might be the common underlying mechanism of the primary cough, exertional, and sexual headache disorders [2]. Valsalva maneuver causes the increase of intrathoracic and intra-abdominal pressure and then impedes venous return to the right atrium and, thus, increases central venous pressure. Because the epidural venous plexus and jugular venous system do not have valves, intracranial venous pressure is increased, with an immediate rise in intracranial pressure. It is also possible that some receptors in venous vessels are hypersensitive to intracranial pressure alteration [29] (Fig. 1).

Proposed pathogenesis of Valsalva maneuver-induced headache
In addition to the transient increased intracranial pressure, crowdedness of the posterior fossa and cerebrospinal fluid (CSF) hypervolemia have also been postulated to be potential causes of PCH [30, 31]. Some have proposed that impaired myogenic cerebrovascular autoregulation might be the central mechanism for EH, whereby EH might be caused by an aberrant vasodilatation during or following exercise [32]. An incompetent internal jugular valve, which leads to transient retrograde venous flow and increased intracranial pressure, has also been proposed to be important in the pathogenesis of EH [33]. However, this seems to be more plausible in patients with headaches during or after Valsalva-like maneuvers rather than prolonged strenuous exercise. To clarify the pathogenesis of EH, a more clear definition of “exertion” is required.
Preorgasmic headache is regarded as a variant of tension-type headache based on the similar dull ache and the awareness of muscle contraction [34], but this hypothesis has never been examined by experimental studies. Orgasmic headache is presumed to be of vascular origin [34], and one cerebral hemodynamic study via acetazolamide test and stress transcranial Doppler sonography suggested impaired metabolic cerebrovascular autoregulation [35]. Several cases of orgasmic headache and one patient with both EH and HSA were reported to have transient cerebral vasoconstrictions, that is, reversible cerebral vasoconstriction syndrome (RCVS) [36–38], but this finding requires further investigations.
The pathophysiology of PSH is still poorly understood and controversial. The spontaneous activation of the peripheral branches of the trigeminal or other nerves has been proposed [4]. However, an intermittent deficit in central pain control mechanisms that permits the spontaneous synchronous discharge of neurons receiving impulses from the area to which stabbing pain is referred is more likely [4, 15••]. Because EH, HAS, and PSH are more common in patients with migraine, this suggests that trigeminal vascular system might play a role for these three headache disorders.
Treatment
All four of these headache disorders are considered indomethacin-responsive headaches. The dosage usually ranges from 50 to 150 mg per day [5, 39]. The therapeutic effect of indomethacin may result from a sustained decrease in intracranial pressure [3]. PCH patients with age at onset of less than 50 years usually have a better response compared with those with later age onset [9••].
Primary Cough Headache
Acetazolamide has been reported to be an effective treatment for patients with PCH. The maximum dose ranges from 1125 to 2000 mg per day, and maintenance of dosage can be adjusted based on responsiveness [31]. The CSF drainage should be reserved as the second-line treatment only after failure of medications because of the invasiveness of the procedure [39].
Primary Exertional Headache
There is no treatment guideline for EH. Conventional approaches include nonpharmacological and pharmacological interventions. Nonpharmacological interventions include biobehavioral strategies such as sports training, proper warm-up before exercise, or hydration with sports drinks. Pharmacological interventions might be tailored to clinical characteristics of EH. Acetaminophen or NSAIDs, especially indomethacin [40], might be considered in patients with mild to moderate EH. Specific antimigrainous treatment, such as triptans, might be used in EH sufferers bearing more migrainous features. Nonetheless, large-scaled controlled studies are required to provide more evidence for decision making.
Primary Headache Associated with Sexual Activity
Some patients can lessen the severity of this type of headache by stopping sexual activity when the headaches begin or by taking a more passive role [13]. The attacks are usually frequent when patients resume sexual activities; therefore, some authors suggest remaining sexually inactive in an acute stage [13]. Indomethacin has positive results on preemptive treatment [20•]. β-Blockers, such as propranolol, metoprolol, and bisoprolol, showed efficacy for prophylaxis [20•].
Primary Stabbing Headache
In addition to indomethacin, some case reports also showed treatment efficacy with celecoxib, rofecoxib, nifedipine, melatonin, and gabapentin in patients with PSH [15••, 41–44]. The chemical structure of melatonin is very similar to that of indomethacin and is found to have antinociceptive and anti-inflammatory properties in animal studies [42]. It may explain its efficacy in patients with PSH.
Prognosis
The disease course of PCH is generally self-limited. Whether responsive to indomethacin or not, PCH usually subsides within 6 months to 2 years, and recurrence is uncommon [9••]. PCH patients with a poor response to indomethacin treatment predicts a poor outcome at follow-up [9••]. One study reported that patients with primary EH usually experienced the condition during a circumscribed period in their early life [12]. Nevertheless, some patients might have headaches for more than 30 years. About 33–50% of patients with HSA have relapsing bouts or run a chronic course (≥1 year); however, 69% of those with a chronic course finally obtain remission at a longer follow-up [19, 20•, 21].
Conclusions
According to recent clinical studies, modification of ICHD-II criteria for these headache disorders is warranted. PCH, primary EH, and primary HSA have different peak ages of onset, but they share similar pathogenesis and treatment. PSH has different clinical characteristics compared with these provoked headache disorders; however, it also responds to indomethacin as do the other headache disorders. The coexistence with migraine is common in primary EH, primary HSA, and PSH. Of note, RCVS, as an emerging diagnosis, should be highly suspect in patients with these headache disorders. A better understanding of the mechanism of these headaches will help us develop more efficient treatment.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Pascual J, Iglesias F, Oterino A, et al.: Cough, exertional, and sexual headaches: an analysis of 72 benign and symptomatic cases. Neurology 1996, 46:1520–1524.
Queiroz LP: Symptoms and therapies: exertional and sexual headaches. Curr Pain Headache Rep 2001, 5:275–278.
Dodick DW: Indomethacin-responsive headache syndromes. Curr Pain Headache Rep 2004, 8:19–26.
Selekler HM, Budak F: Idiopathic stabbing headache and experimental ice cream headache (short-lived headaches). Eur Neurol 2004, 51:6–9.
Pareja JA, Ruiz J, de Isla C, et al.: Idiopathic stabbing headache (jabs and jolts syndrome). Cephalalgia 1996, 16:93–96.
Raskin NH, Schwartz RK: Ice pick-like pain. Neurology 1980, 30:203–205.
Headache Classification Subcommittee of the International Headache Society Classification Subcommittee: The International Classification of Headache Disorders, 2nd edn. Cephalalgia 2004, 24(Suppl 1):1–160.
•• Pascual J, González-Mandly A, Martín R, Oterino A: Headaches precipitated by cough, prolonged exercise or sexual activity: a prospective etiological and clinical study. J Headache Pain 2008, 9:259–266. This study prospectively evaluated a large sample of patients with these headache disorders and comprehensively recorded the clinical pictures.
•• Chen PK, Fuh JL, Wang SJ: Cough headache: a study of 83 consecutive patients. Cephalalgia 2009, 29:1079–1085. This most recent large-scaled study provided the differences between primary and secondary cough headaches and field-tested the ICHD-II criteria of PCH.
Sjaastad O, Bakketeig LS: Exertional headache I. The Vågå study of headache epidemiology. Cephalalgia 2002, 22:784–790.
•• Chen SP, Fuh JL, Lu SR, Wang SJ: Exertional headache: a survey of 1963 adolescents. Cephalalgia 2009, 29:401–407. This is the first large-scaled epidemiologic study of EH in adolescence. It is also the first systematic study to investigate the applicability of ICHD-II criteria for this headache disorder.
Sjaastad O, Bakketeig LS: Exertional headache-II. Clinical features Vågå study of headache epidemiology. Cephalalgia 2003, 23:803–807.
Frese A, Eikermann A, Frese K, et al.: Headache associated with sexual activity: demography, clinical features and comorbidity. Neurology 2003, 61:796–800.
Sjaastad O, Pettersen H, Bakketeig LS: The Vågå study of headache epidemiology II. Jabs: clinical manifestations. Acta Neurol Scand 2002, 105:25–31.
•• Fuh JL, Kuo KH, Wang SJ: Primary stabbing headache in a headache clinic. Cephalalgia 2007; 27:1005–1009. This article presents the most recent large-scale comprehensive and prospective study in the headache clinic.
Rasmussen BK, Olesen J: Symptomatic and nonsymptomatic headaches in a general population. Neurology 1992, 42:1225–1231.
Tuğba T, Serap U, Esra O, et al.: Features of stabbing, cough, exertional and sexual headaches in a Turkish population of headache patients. J Clin Neurosci 2008, 15:774–777.
Rooke D: Benign exertional headache. Med Clin North Am 1968, 52:801–808.
Ostergaard JR, Kraft M: Benign coital headache. Cephalalgia 1992, 12:353–355.
• Frese A, Rahmann A, Gregor N, et al.: Headache associated with sexual activity: prognosis and treatment options. Cephalalgia 2007, 27:1265–1270. This is the most recent large-scaled study for long-term prognosis and treatment outcome in patients with primary sexual headache.
Silbert PL, Edis RH, Stewart-Wynne EG, Gubbay SS: Benign vascular sexual headache and exertional headache: interrelationships and long term prognosis. J Neurol Neurosurg Psychiatry 1991, 54:417–421.
Olesen J: The future of headache classification and classification research. Cephalalgia 2009 Aug 10 (Epub ahead of print).
Paulson GW, Klawns HL: Benign orgasmic cephalgia. Headache 1974, 13:181–187.
Lance JW: Benign masturbatory cephalalgia. Arch Neurol 1983, 40:393.
Østergaard JR, Kraft M: Natural course of benign coital headache. BMJ 1992, 305:1129.
Østergaard JR, Kraft M: Benign coital headache. Cephalalgia 1992, 12:353–355.
Sjaastad, O, Pettersen, H, Bakketeig LS: Long-lasting cephalic jabs (?) The Vågå study of headache epidemiology. Cephalalgia 2005, 25:581–592.
Ammache Z, Graber M, Davis P: Idiopathic stabbing headache associated with monocular visual loss. Arch Neurol 2000, 57:745–746.
Raskin NH: Short-lived head pains. Neurol Clin 1997, 15:143–152.
Chen YY, Ling JF, Fuh JL, et al.: Primary cough headache is associated with posterior fossa crowdedness: a morphometric MRI study. Cephalalgia 2004, 24:694–699.
Wang SJ, Fuh JL, Lu SR: Benign cough headache is responsive to acetazolamide. Neurology 2000, 55:149–150.
Raskin NH: The cough headache syndrome: treatment. Neurology 1995, 45:1784.
Heckmann JG, Hilz MJ, Mück-Weymann M, Neundörfer B: Benign exertional headache/benign sexual headache: a disorder of myogenic cerebrovascular autoregulation? Headache 1997, 37:597–598.
Doepp F, Valdueza JM, Schreiber SJ: Incompetence of internal jugular valve in patients with primary exertional headache: a risk factor? Cephalalgia 2008, 28:182–185.
Lance JW: Headaches related to sexual activity. J Neurol Neurosurg Psychiatry 1976, 39:1226–1230.
Evers S, Schmidt O, Frese A, et al.: The cerebral hemodynamics of headache associated with sexual activity. Pain 2003, 102:73–78.
Silbert PL, Hankey GJ, Prentice DA, Apsimon HT: Angiographically demonstrated arterial spasm in a case of benign sexual headache and benign exertional headache. Aust N Z Med 1989, 19:466–468.
Chen SP, Fuh JL, Lirng JF, et al.: Recurrent primary thunderclap headache and benign CNS angiopathy: spectra of the same disorder? Neurology 2006, 67:2164–2169.
Keyrouz S, Dhar R, Axelrod Y: Call-Fleming syndrome and orgasmic cephalalgia. Headache 2008, 48:967–971.
Diamond S: Prolonged benign exertional headache: its clinical characteristics and response to indomethacin. Headache 1982, 22:96–98.
Jacome DE: Exploding head syndrome and idiopathic stabbing headache relieved by nifedipine. Cephalalgia 2001; 21:617–618.
Rozen TD: Melatonin as a treatment for indomethacin-responsive headaches. Neurology 2003, 61:865–866.
Piovesan EJ, Zukerman E, Kowacs PA, Werneck LC: COX-2 inhibitor for the treatment of idiopathic stabbing headache secondary to cerebrovascular diseases. Cephalalgia 2002, 22:197–200.
Franca MC Jr, Costa AL, Maciel JA Jr: Gabapentin-responsive idiopathic stabbing headache. Cephalalgia 2004, 24:993–996.
Disclosure
Dr. Shuu-Jiun Wang has served on scientific advisory boards for Pfizer, Inc., Merck Serono, and Allergan, Inc.; has received speaker honoraria from Novartis, GlaxoSmithKline, Pfizer, Inc., Eli Lilly and Company, Janssen-Cilag, Boehringer Ingelheim, Merck Serono, Allergan, Inc., and Wyeth; and receives research support from Merck Serono.
No other potential conflicts of interest relevant to this article were reported.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Wang, SJ., Fuh, JL. The “Other” Headaches: Primary Cough, Exertion, Sex, and Primary Stabbing Headaches. Curr Pain Headache Rep 14, 41–46 (2010). https://doi.org/10.1007/s11916-009-0083-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11916-009-0083-0