
Abstract
Angiogenesis is central to the growth of normal tissues and tumors. Inhibiting this pathway has been a strategy for drug development for tumors not responsive to most agents used in chemotherapy. Notably, signaling mediated by vascular endothelial growth factor (VEGF) is a key target because aberrant signaling via this pathway is frequently associated with neoangiogenesis in tumors. The drug-discovery effort to blunt VEGF signaling has led to the approval of bevacizumab and several receptor tyrosine kinase inhibitors (TKIs) that have shown efficacy in the clinical management of breast, colorectal, lung, and kidney cancer. Understanding the genetic variability in VEGF and VEGF receptor has led to identifying genotypic variations (single nucleotide polymorphisms [SNPs]) associated with treatment outcome and toxicity. Notably, identification of SNPs in VEGF associated with angiogenesis inhibitor treatment-induced hypertension and outcome provides exciting opportunities for personalized medicine to improve outcome and reduced toxicity with these novel TKIs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Because angiogenesis is central to the growth of normal tissues and tumors, inhibiting this pathway has been a strategy for drug development [1]. Notably, signaling mediated by vascular endothelial growth factor (VEGF) has been a target because aberrant signaling via this pathway is frequently associated with neoangiogenesis in tumors. The forerunner to this drug-discovery effort to blunt VEGF signaling is the antibody, bevacizumab, which is approved for use in the treatment of breast, colorectal, lung, and kidney cancer [1]. Although the mechanism of action of bevacizumab involves binding to VEGF, the complexity of the VEGF pathway suggests a requirement for a more comprehensive approach to inhibit this key signaling pathway [2]. This effort has led to the development of VEGF receptor (VEGFR) tyrosine kinase inhibitors (TKIs). These small molecule inhibitors that are essentially multi-kinase inhibitors have rapidly entered the clinical arena because of their efficacy in treating cancers, particularly renal cancer that is generally not responsive to therapy effective in several other tumor types [2].
Among the tumors in which TKIs are effective, most studies have focused on renal cell carcinoma (RCC) possibly because of the remarkable effects of sorafenib and sunitinib in the clinical management of this disease. The TKIs (also referred to as multi-kinase inhibitors) inhibit several receptor tyrosine kinases including but not restricted to VEGFR-1, -2, and -3, platelet-derived growth factor receptor (PDGFR)-α, PDGFR-β, and c-Kit [2]. The success of these TKIs in the treatment of RCC is further exemplified by the recent approval of pazopanib, which is also an inhibitor of several receptor tyrosine kinases (R5). Although it is not entirely clear, the efficacy of these TKIs in inhibiting several receptor tyrosine kinases (RTKs) in the angiogenesis signaling pathway could be responsible for both their efficacy and toxicity.
Several excellent reviews on the clinical efficacy and toxicity of TKIs have been published. This article focuses on the mechanistic basis for the efficacy/toxicity of TKIs with emphasis on VEGF polymorphisms. Although bevacizumab is an angiogenesis inhibitor and not a TKI, this review discusses this agent along with the TKIs because there is possible overlap in VEGF polymorphisms that are involved with regard to treatment outcome and toxicity.
VEGF Levels and TKIs
The central role for VEGF, a critical angiogenic molecule, is exemplified by its role in development, normal physiology, and in certain pathologic conditions. Because the angiogenesis inhibitors target the VEGF signaling pathway, efficacy of toxicity of TKIs and other angiogenesis inhibitors could be related to the effect on circulating VEGF levels that could impact on normal homeostasis. In the case of bevacizumab that can bind to and consequently inhibit the biologic activity of human VEGF, the general effect of treatment with this agent is decreased circulating VEGF levels. However, with the TKIs that target the RTKs (eg, sunitinib), an increase in VEGF levels and a decrease in soluble VEGFR-2 (sVEGFR-2) and sVEGFR-3 was observed in cytokine refractory patients with metastatic RCC (mRCC) [3••]. Interestingly, these changes in VEGF and sVEGFR were observed during treatment with sunitinib, and levels tended to return to near-baseline after 2 weeks off treatment, indicating that these effects were dependent on drug exposure. Further, significantly larger changes in VEGF, sVEGFR-2, and sVEGFR-3 levels were observed in patients exhibiting objective tumor response compared with those exhibiting stable disease or disease progression (P < 0.05 for each analyte).
Elucidation of the mechanism(s) responsible for VEGF and placenta growth factor (PlGF) induction will require further study, but treatment-related increases in tumor hypoxia may be involved, perhaps via increased activity of hypoxia-inducible factor (HIF)-1α or other HIFs. However, the induction may not be completely tumor dependent because laboratory studies in nontumor-bearing mice suggest that VEGF induction following treatment with anti-VEGFR2 monoclonal antibodies is dose-dependent and normalized after discontinuation of therapy [4••]. These results suggest that observed sunitinib-induced plasma changes in VEGF signaling intermediates represent a systemic tumor-independent response to therapy and may correlate with the most efficacious antitumor doses, potentially having utility for defining the optimal biologic dose range for this drug class but not as predictive markers of tumor response or clinical benefit. It is also likely that these changes in VEGF and VEGFR may also be relevant to drug-associated toxicities, drug resistance, and observed rapid tumor (re)growth seen after cessation of therapy.
Another clinical trial examining antitumor activity of sunitinib in patients with bevacizumab refractory mRCC showed that mean plasma VEGFA and PlGF levels significantly increased, whereas VEGFC and sVEGFR3 levels decreased with sunitinib treatment in this patient cohort with subsequent restoration to near-baseline during off-treatment periods [5]. Furthermore, lower baseline levels of sVEGFR3 and VEGFC were found to be associated with longer progression-free survival and objective response rate, suggesting that baseline levels of sVEGFR3 and VEGFC may have potential utility as biomarkers of clinical efficacy in this clinical setting. Interestingly, in a more recent study by Feldman et al. [6] evaluating sunitinib plus bevacizumab, although VEGF levels were found to be inversely correlated with response, the rise in VEGF levels was not similar to that previously reported with sunitinib monotherapy [6]. Further understanding of the biologic basis for these observations is needed, but it is of interest to note that preeclampsia is associated with increased VEGF levels and the potential link to genetic polymorphisms, toxicity, and TKI therapy will be discussed later.
Toxicity Associated with TKI Therapy
Because VEGF pathway and angiogenesis are central to growth and development as well as physiologic processes of normal organ function and maintenance, it is not completely surprising that adverse effects could be expected by inhibition of this key signaling pathway [7]. Adverse effects associated with these agents include hypertension, renal dysfunction, arterial thromboembolic events, bowel perforation, reversible posterior leukoencephalopathy syndrome, wound complications, and hemorrhage. The exact molecular mechanisms of the adverse effects of VEGF/VEGFR inhibitors are not fully understood. Although bevacizumab and TKIs have distinctive targets and mechanism(s) of action, they do share the class adverse effects as a result of VEGF or VEGFR inhibition.
Hypertension
Hypertension is the most common side effect of VEGF pathway inhibitors. VEGFR2 signaling generates nitric oxide and prostaglandin I2, which induces endothelial cell-dependent arteriole and venous vasodilatation, thereby controlling blood pressure [8, 9]. Inhibition of VEGF pathway, therefore, could lead to vasoconstriction and, thereby, hypertension. Furthermore, direct endothelial cell apoptosis by VEGF blockage and resulting rarefaction (decreased arteriole and capillary densities) has also been hypothesized as a mechanism of hypertension induced by anti-VEGF therapy [10]. Degree of hypertension caused by these agents has been shown to be dose-dependent [11, 12]. In addition to dose and inherent differences between agents, host susceptibility can also affect the rate of hypertension. Preexisting hypertension has been seen to be a risk factor in further elevation in blood pressure with these agents. Although the etiology is unclear, of particular significance is the higher incidence for development of hypertension in patients with mRCC, compared with patients with other tumors [13].
Cardiomyopathy
Cardiomyopathy and congestive heart failure (CHF) have been reported with the use of VEGF- and VEGFR targeting agents, although lack of prospective monitoring precludes definitive causality. Ventricular dysfunction with VEGF/VEGFR inhibitors is suggested in cardiomyocyte-specific VEGF knockout murine models, which present with dilated cardiomyopathy [14]. Furthermore, cardiomyopathy has been associated with sunitinib in an early phase 1/2 trial with this agent in imatinib refractory gastrointestinal stromal tumor (GIST) patients, which incorporated careful cardiac monitoring [15••]. Twenty percent of patients showed a drop in left ventricular ejection fraction below the normal range (<50%) and 8% developed clinical CHF, which was reversible upon cessation of therapy. Refractory CHF with fatal outcomes has rarely been reported in trials of anti-angiogenic agents.
Renal Damage and Proteinuria
Proteinuria has been observed in all studies with bevacizumab treatment. However, it is rarely reported in clinical trials with VEGFR TKIs, such as sunitinib or sorafenib. With axitinib, however, 32% of patients (17 of 52) with mRCC developed grade 2 or higher proteinuria and a few patients had proteinuria more than 1 g per 24 h urine [16]. Underlying mechanisms of proteinuria and renal damage may be caused by the filtration barrier of the renal glomeruli, which is formed partly by endothelial cells. It has been suggested that VEGF/VEGFR2 interaction is important in repair of the renal system [17, 18]. Furthermore, in murine models, heterozygous deletion of VEGF led to loss of endothelial cell fenestration, loss of podocytes, mesangiolysis, and proteinuria. Importantly, VEGF has also been shown to have a critical protective role in the pathogenesis of microangiopathic process [19]. Pathologic findings in the past have included proliferative glomerulonephritis, interstitial nephritis, and thrombotic microangiopathy [20–22].
Hemorrhage
The risk of bleeding is increased in patients with the use of VEGF pathway inhibitor therapy. Both mucocutaneous and tumor-related bleeding have been reported. Mild epistaxis and mucocutaneous bleeding comprise the most common presentation (20–40%) with bevacizumab therapy. They have also been described with sunitinib and other TKIs [23]. Fatal hemorrhage has been most prevalent in tumors of the lung and gastrointestinal tract. Life-threatening hemoptysis has been shown to occur with lung cancer with squamous histology (a current contraindication for bevacizumab therapy) [24]. In a phase 3 trial of advanced colorectal cancer, gastrointestinal hemorrhage was 24% in the bevacizumab plus chemotherapy group compared with 6% in the chemotherapy control group. Tumor-related bleeding has also been shown with sunitinib-treated GIST patients including central nervous system bleeding [25].
Overall, it is apparent that interfering with a VEGF signaling pathway either with a VEGF-targeted antibody or TKIs is associated with a pattern of toxicity that is also observed in patients with preeclampsia.
VEGF SNPs
Given the central role for VEGF in angiogenesis and the association of VEGF levels with certain pathologic conditions, there has been considerable effort in identifying a link to genetic variability. Although the role of VEGF levels and their impact on outcome and toxicity has been addressed, these studies for the most part are correlations without genotype data, making it difficult to assess the impact of genetic polymorphisms. The VEGF gene is quite complex, with several alternatively spliced isoforms, and the regulation of expression could differ between normal and tumor tissue. Interestingly, because all identified polymorphisms in VEGF are not in the coding region, possible mechanisms for their role in gene expression have been proposed. Table 1 outlines single nucleotide polymorphisms (SNPs), with emphasis on their role in different types of human malignancies [26–28••, 29–37]. As a footnote, we also indicate other noncancer-related pathologic states that have been associated with VEGF SNPs [38–47].
Although many transcription factors bind to the promoter regions of VEGF [48], none occur at the common polymorphic sites associated with VEGF expression. Nevertheless, these SNPs have been reported to cause changes in VEGF expression levels [49] and have been correlated with different cancers (Table 1). However, the mechanism for these associations remains to be determined.
In terms of the role of SNPs and their impact on VEGF levels, the 936C>T polymorphism (rs3025039) occurs in the 3′ untranslated region (UTR). Studies have shown an association between this SNP, VEGF levels and cancer (Table 1) [49]. This SNP occurs at a potential AP-4 binding site [50], which may affect mRNA stability. The other SNP, –634G>C (rs2010963), occurs in the 5′-UTR and this polymorphism occurs in the internal ribosome entry site (IRES)-B domain critical for expression of one of the VEGF isoforms [51••]. Currently, it is not apparent how these SNPs affect VEGF levels in patients with TKIs and the impact on outcome or toxicity. However, with regard to TKI-induced toxicity and VEGF SNPs, we will focus on hypertension because this is a major toxicity associated with TKI therapy.
As indicated earlier, the association of VEGF polymorphisms with outcome and toxicity will also include data with bevacizumab because there is overlap both in toxicity profile and treatment-induced hypertension. With regard to TKI treatment-induced hypertension that is not associated with VEGF polymorphisms, there is compelling evidence that this is related to potency and, particularly, the affinity of the agent for binding to VEGFR2 [2]. This proposed correlation is further strengthened by the recent finding that treatment with a specific VEGFR2 antibody in vivo leads to a sustained and rapid increase in blood pressure [52]. Based on this observation it was inferred that VEGF acting through VEGFR2 can play a critical role in blood pressure control by promoting nitric oxide synthase expression and nitric oxide activity [52]. From these observations, it can be surmised that interfering with VEGF signaling by sequestering VEGF with bevacizumab or inhibiting VEGFR2 receptor activity with a TKI can lead to hypertension induced by these agents that interfere with angiogenesis.
VEGF SNPs and Toxicity with Angiogenesis Inhibitors or TKIs
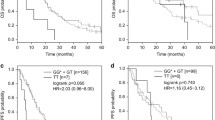
In a pioneering study evaluating a panel of VEGF genotype polymorphisms in tumor DNA (–2578 C/A, –1498 C/T, –1154 G/A, –634 G/C, and 936 C/T), Schneider et al. [28••] reported specific VEGF genotypes that correlated with bevacizumab-induced hypertension. Specifically, the genotypes VEGF –634 CC and VEGF –1498 TT compared with alternate genotypes were found to be associated with significantly less grade 3 or 4 hypertension in patients with metastatic breast cancer that were treated with paclitaxel plus bevacizumab (P = 0.005 and P = 0.022, respectively). Interestingly, this correlation of VEGF genotype with hypertension was not associated with VEGF expression in the tumor. However, this study did not report the impact of circulating VEGF levels, which would have been of interest because the VEGF 936 C/T polymorphism has been linked to plasma VEGF levels [50]. More recently, Kim et al. [53] have evaluated the role of VEGF genotype polymorphisms on sunitinib-induced hypertension in patients with mRCC. In this retrospective study, patients with mRCC treated with sunitinib (50 mg, 4 weeks on/2 weeks off) and who had available blood pressure data were analyzed. Specifically, using genomic DNA isolated from peripheral blood lymphocytes, VEGF SNPs –634 C/G and –1498 C/T were amplified using primers designed to flanking sequences for the respective SNPs. Genotypes were subsequently assigned following sequence analysis. Among a cohort of 64 patients with 63 analyzable, 89% patients had prior nephrectomy and 63% were previously treated with cytokines and/or a TKI. In this cohort, 57% patients were on antihypertensive therapy at baseline with baseline systolic and diastolic blood pressure of 139 mm Hg (range, 93–190) and 80 mm Hg (range, 47–103), respectively. For the VEGF –634 genotype (Fig. 1), the distribution of patients was C/C (10%), C/G (33%), and G/G (57%). Further, VEGF –634 C/C < C/G < G/G genotypes were found to be associated with increasing frequency and duration of hypertension (defined as diastolic >90 mm Hg and/or systolic >150 mm Hg) during treatment with sunitinib (P = 0.03 and P = 0.007, respectively). Further, the significance of these findings persisted even after adjusting for baseline blood pressure and the use of antihypertensive medications (P = 0.05 and P = 0.02, respectively). In contrast, a similar correlation for the VEGF –1498 VEGF genotype was not found. It is of interest to note that, although the correlation of VEGF –634 genotype with hypertension was observed with bevacizumab [28••] and sunitinib [53], the VEGF –1498 genotype was correlated only with bevacizumab treatment. It is difficult to define a mechanistic basis, but one potential reason could be the larger patient cohort with the bevacizumab trial [28••]. A potential problem with the study by Kim et al. [53] is absence of data on plasma VEGF levels and their relationship to the VEGF SNP genotype for additional correlative data. Evaluation of other VEGF SNPs (–2578 C/A, –2459 in/del18, 1154 G/A, and 936 C/T), as well as VEGFR-2 SNPs (889 G/A [rs2305948] and 1416 A/T [rs1870377] in mRCC patients treated with sunitinib for association with outcome and toxicity are ongoing at the Taussig Cancer Institute, Cleveland Clinic Foundation.

Association of vascular endothelial growth factor single nucleotide polymorphism –634 genotype and duration of hypertension in metastatic renal cell carcinoma patients (n = 63) treated with sunitinib [53]. DBP diastolic blood pressure; SBP systolic blood pressure
VEGF SNPs and Outcome with Angiogenesis Inhibitors or TKIs
In the study by Schneider et al. [28••] following treatment with paclitaxel or paclitaxel plus bevacizumab, the association of VEGF SNPs with treatment outcome was also determined. In particular VEGF –2578 A/A was found to associated with superior median overall survival in patients treated in the combination arm (plus bevacizumab) compared with alternate genotypes combined. Further, with VEGF –1154, the A allele was correlated with a superior median overall survival and an additive effect of each active allele only for patients treated in the combination arm (plus bevacizumab). Interestingly, no significant associations with other VEGF or VEGFR-2 genotypes and efficacy were observed in this study [28••]. The only other report on VEGF genotype and treatment outcome is by Schultheis et al. [54], identifying that the VEGF 936 C/T genotype had a longer median progression-free survival compared with C/C and T/T genotype (P = 0.061) in patients with recurrent/metastatic epithelial ovarian cancer treated with cyclophosphamide plus bevacizumab. A problem with this study is the absence of a treatment arm without bevacizumab for comparison. No data on association of VEGF genotype and toxicity was reported in this study. In the Kim et al. [53] study, VEGF –634 and –1498 genotypes were not found to be associated with tumor volume reduction or progression-free survival.
Future Directions
The role of VEGF/VEGFR genotype and correlations with outcome and toxicity in patients treated with angiogenesis inhibitors is still in its infancy. As this review has outlined, a substantial amount of published information exists on VEGF and/or VEGFR SNPs and the association with both nonmalignant and malignant disease conditions. Although this is helpful information, it is lacking data on the correlation between VEGF and/or VEGFR SNPS associated with prognosis/progression of a cancer type and response to the angiogenesis inhibitor treatment. Obviously, a more comprehensive analysis of both SNPs and expression of biomarkers in the VEGF signaling pathway will be important to critically understand whether association of outcome and toxicity with angiogenesis inhibitors is exclusively treatment related. Although studies have used genomic DNA from either peripheral blood mononuclear cells or tumor, our ongoing studies suggest a more than 98% concordance in paired samples. However, for correlations with expression and outcome, tumor material is important. Another unanswered question is whether the metastatic tumor that is being treated maintains the genotype and expression pattern for VEGF signaling determined with the primary tumor, so that meaningful correlative associations with outcome can be derived. Overall, these are exciting times when unique opportunities for personalized medicine with angiogenesis inhibitors are a reality with significant promise to improve treatment outcome and reduce toxicity.
References
Papers of particular interest, published recently, have been highlighted as: •• Of major importance
Folkman J: Angiogenesis. Annu Rev Med 2006, 57:1–8.
Bhargava P: VEGF kinase inhibitors: how do they cause hypertension? Am J Physiol Regul Integr Comp Physiol 2009, 297:R1–R5.
DePrimo SE, Bello CL, Smeraglia J, et al.: Circulating protein biomarkers of pharmacodynamic activity of sunitinib in patients with metastatic renal cell carcinoma: modulation of VEGF and VEGF-related proteins. J Transl Med 2007, 5:32–43. This informative article discusses circulating biomarkers in mRCC patients treated with sunitinib.
Ebos JML, Lee CR, Christensen JG, et al.: Multiple circulating proangiogenic factors induced by sunitinib malate are tumor-independent and correlate with antitumor efficacy. PNAS 2007, 104:17069–17074. This article discusses possible tumor-independence of circulating proangiogenic factors during treatment with sunitinib.
Rini BI, Dror Michaelson M, Rosenberg JE, et al.: Antitumor activity and biomarker analysis of sunitinib in patients with bevacizumab-refractory metastatic renal cell carcinoma. J Clin Oncol 2008, 26:3743–3748.
Feldman DR, Baum MS, Ginsberg MS, et al.: Phase I trial of bevacizumab plus escalated doses of sunitinib in patients with metastatic renal cell carcinoma. J Clin Oncol 2009, 27:1432–1439.
Sane DC, Anton L, Brosnihan B: Angiogenic growth factors and hypertension. Angiogenesis 2004, 7:193–201.
Hood JD, Meininger CJ, Ziche M, et al.: VEGF upregulates ecNOS message, protein, and NO production in human endothelial cells. Am J Physiol 1998, 274:H1054–H1058.
Horowitz JR, Rivard A, van der Zee R, et al.: Vascular endothelial growth factor/vascular permeability factor produces nitric oxide-dependent hypotension. Arterioscler Thromb Vasc Biol 1997, 17:2793–2800.
Ciuffetti G, Schillaci G, Innocente S, et al.: Capillary rarefaction and abnormal cardiovascular reactivity in hypertension. J Hypertens 2003, 21:2297–2303.
Yang JC, Haworth L, Sherry RM, et al.: A randomized trial of bevacizumab, an anti-vascular endothelial growth factor antibody, for metastatic renal cancer. N Engl J Med 2003, 349:427–434.
Maitland ML, Moshier K, Imperial J, et al.: Blood pressure (BP) as a biomarker for sorafenib (S), an inhibitor of the vascular endothelial growth factor (VEGF) signaling pathway. J Clin Oncol 2006, 24:2035.
Llovet JM, Ricci S, Mazzaferro V, et al.: Sorafenib in advanced hepatocellular carcinoma. N Engl J Med 2008, 359: 378–390.
Giordano FJ, Gerber HP, Williams SP, et al.: A cardiac myocyte vascular endothelial growth factor paracrine pathway is required to maintain cardiac function. PNAS 2001, 98:5780–5785.
Chu TF, Rupnick MA, Kerkela R, et al.: Cardiotoxicity associated with tyrosine kinase inhibitor sunitinib. Lancet Oncol 2007, 370:2011–2019. This article reviews TKI-associated cardiotoxicity.
Rixe O, Bukowski RM, Dror Michaelson M, et al.: Axitinib treatment in patients with cytokine-refractory metastatic renal-cell cancer: a phase II study. Lancet Oncol 2007, 8:975–984.
Eremina V, Sood M, Haigh J, et al.: Glomerular-specific alterations of VEGF-A expression lead to distinct congenital and acquired renal diseases. J Clin Invest 2003, 111:707–716.
Schrijvers BF, Flyvbjerg A, DeVrise AS: The role of vascular endothelial growth factor (VEGF) in renal pathophysiology. Kidney Int 2004, 65:2003–2017.
Eremina V, Jefferson JA, Kowalewska J, et al.: VEGF inhibition and renal thrombotic microangiopathy. N Engl J Med 2008, 358:1129–1136.
Barakat RK, Singh N, Lal R, et al.: Interstitial nephritis secondary to bevacizumab treatment in metastatic meiomyosarcoma. Ann Pharmacother 2007, 41:707–710.
Frankie C, Leachier C, Medina J, et al.: Renal thrombosis microangiopathy caused by anti-VEGF-antibody treatment for metastatic renal-cell carcinoma. Lancet Oncol 2007, 8:177–178.
Roncone D, Sattskar A, Nadasdy T, et al.: Proteinuria in a patient receiving anti-VEGF therapy for metastatic renal cell carcinoma. Nat Clin Pract 2007, 3:287–293.
Motzer RJ, Hutson TE, Tomczak P, et al.: Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med 356:115–124.
Johnson DH, Fehrenbacher L, Novotny WF, et al.: Randomized phase II trial comparing bevacizumab plus carboplatin and paclitaxel with carboplatin and paclitaxel alone in previously untreated locally advanced or metastatic non-small-cell lung cancer. J Clin Oncol 2004, 22:2184–2191
McDermott DF, Soman JA, Gonzalez R, et al.: Double-blind randomized phase II study of the combination of sorafenib and dacarbazine in patients with advanced melanoma: a report from the 11715 study group. J Clin Oncol 2008, 26:2178–2185.
Kawai Y, Sakano S, Korenaga Y, et al.: Associations of single nucleotide polymorphisms in the vascular endothelial growth factor gene with the characteristics and prognosis of renal cell carcinomas. Eur Urol 2007, 52:1147–1155.
Kim DH, Lee NY, Lee MH, et al.: Vascular endothelial growth factor (VEGF) gene (VEGFA) polymorphism can predict the prognosis in acute myeloid leukaemia patients. Br J Haematol 2007, 140:71–79.
Schneider BP, Wang M, Radovich M, et al.: Association of vascular endothelial growth factor and vascular endothelial growth factor receptor-2 genetic polymorphisms with outcome in trial of paclitaxel compared with paclitaxel compared with pacitaxel plus bevacizumab in advanced breast cancer: ECOG 2100. J Clin Oncol 2008, 20:4672–4678. This publication provides important information on VEGF SNPs that are associated with outcome and toxicity in patients treated with bevacizumab.
Hsiao PJ, Lu MY, Chiang FY, et al.: Vascular endothelial growth factor gene polymorphisms in thyroid cancer. J Endocrinol 2007, 195:265–270.
Jacobs EJ, Feigelson HS, Bain EB, et al.: Polymorphisms in the vascular endothelial growth factor gene and breast cancer in the Cancer Prevention Study II cohort. Breast Cancer Res 2006, 8:R22.
Zhai R, Liu G, Asomaning K, et al.: Genetic polymorphisms of VEGF, interactions with cigarette smoking exposure and esophageal adenocarcinoma risk. Carcinogenesis 2008, 29:2330–2334.
Cacev T, Loncar B, Seiwerth S, et al.: Vascular endothelial growth factor polymorphisms -1154G/A and -460C/T are not associated with VEGF mRNA expression and susceptibility to sporadic colon cancer. DNA Cell Biol 2008, 27:569–574.
Heist RS, Zhai R, Lui G, et al.: VEGF polymorphisms and survival in early-stage non-small-cell lung cancer. J Clin Oncol 2008, 26:856–862.
Ricketts C, Zeegers MP, Lubinski J, et al.: Analysis of germline variants in CDH1, IGFBBP3, MMP1, MMP3, STK15 and VEGF in familial and sporadic renal cell carcinoma. PloS One 2009, 4:e6037.
Smerdel MP, Waldstrom M, Brandslund I, et al.: Prognostic importance of vascular endothelial growth factor-A expression and vascular endothelial growth factor polymorphisms in epithelial ovarian cancer. Int J Gynecol Cancer 2009, 19:578–584.
Garcia-Closas M, Malats N, Real FX, et al.: Large-scale evaluation of candidate genes identifies associations between VEGF polymorphisms and bladder cancer risk. PLoS Genet 2007, 3:e29.
Bae SJ, Ahn DH, Hong SP, et al.: Gender-specific association between polymorphism of vascular endothelial growth factor (VEGF 936C>T) gene and patient with stomach cancer. Yonsei Med J 2008, 29:783–791.
Churchill AJ, Carter JG, Ramsden C, et al.: VEGF Polymorphisms are associated with severity of diabetic retinopathy. Invest Ophtalmol Vis Sci 2008, 49:3611–3616.
Nakanishi K, Watanabe C: Single nucleotide polymorphisms of vascular endothelial growth factor gene intron 2 are markers for early progression of diabetic retinopathy in Japanese with type 1 diabetes. Clin Chim Acta 2009, 402:171–175.
Breunis WB, Biezeveld MH, Geissler J, et al.: Vascular endothelial growth factor gene haplotypes in Kawasaki disease. Arthritis Rheum 2009, 54:1588–1594.
Yuan Q, Zuo X, Jia J: Association between promoter polymorphisms of vascular endothelial growth factor gene and sporadic Alzheimer’s disease among northern Chinese Han. Neurosci Lett 2009, 457:133–136.
Salvarani C, Boiardi L, Casali B, et al.: Vascular endothelial growth factor gene polymorphisms in Behcet’s disease. J Rheumatol 2004, 31:1785–1789.
Galazioz G, Papazoglou D, Tsikouras P, et al.: Vascular endothelial growth factor gene polymorphisms and pregnancy. J Matern Fetal Neonatal Med 2009, 22:371–378.
Lin LM, Wan L, Tsai YY, et al.: Vascular endothelial growth factor gene polymorphisms in age-related macular degeneration. Am J Opthalmol 2008, 145:1045–1051.
Butt C, Lim S, Greenwood C, et al.: VEGF, FGF1, FGF2 and EGF gene polymorphisms and psoriatic arthritis. BMC Musculoskelet Disord 2007, 8:1.
Rueda B, Lopez-Nevot MA, Lopez-Diaz MJ, et al.: A functional variant of vascular endothelial growth factor is associated with severe ischemic complications in giant cell arteritis. J Rheumatol 2005, 32:1737–1743.
Doi K, Noiri E, Nakao A, et al.: Functional polymorphisms in the vascular endothelial growth factor gene are associated with development of end-stage renal disease in males. J Am Soc Nephrol 2006, 17:823–830.
Pages G, Puyssegur J: Transcriptional regulation of the vascular endothelial growth factor gene—a concert of activating factors. Cardiovascular Res 2005, 65:564–573.
Pander J, Gelderblom H, Guchelaar HJ: Pharmacogenetics of EGFR and VEGF inhibition. Drug Discov Today 2007, 12:1054–1060.
Renner W, Kotschan S, Hoffmann, C, et al.: A common 936 C/T Mutation in the gene for vascular endothelial growth factor is associated with vascular endothelial growth factor plasma levels. J Vasc Res 2000, 37:443–448.
Bastide A, Karaa K, Bornes S, et al.: An upstream open reading frame with in an IRES controls expression of specific VEGF-A isoform. Nucleic Acids Res 2008, 36:2434–2445. This article identifies a region in the 5′UTR of VEGF (IRESB) that is critical in the expression of a VEGF isoform. The -634G>C SNP occurs in this region. This paper highlights the complex level of regulation of VEGF expression at the transcription and translation levels.
Facemire CS, Nixon, AB, Griffiths R, et al.: Vascular endothelial growth factor receptor 2 controls blood pressure by regulating nitric oxide synthase expression. Hypertension 2009, 54:652–658.
Kim JJ, Vaziri SA, Elson BI, et al.: VEGF single nucleotide polymorphisms (SNPs) and correlation to sunitinib-induced hypertension (HTN) in metastatic renal cell carcinoma (mRCC) patients (pts). J Clin Oncol 2009, 27:15s.
Schultheis AM, Lurje G, Rhodes KE, et al.: Polymorphisms and clinical outcome in recurrent ovarian cancer treated with cyclophosphamide and bevacizumab. Clin Can Res 2008, 14:7554–7563.
Disclosure
No potential conflicts of interest relevant to this article were reported.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vaziri, S.A.J., Kim, J., Ganapathi, M.K. et al. Vascular Endothelial Growth Factor Polymorphisms: Role in Response and Toxicity of Tyrosine Kinase Inhibitors. Curr Oncol Rep 12, 102–108 (2010). https://doi.org/10.1007/s11912-010-0085-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11912-010-0085-4