
Abstract
Rabies has the highest case fatality of any infectious disease. Pathobiological and clinical insights have questioned the assertion that death is inevitable after onset of acute encephalomyelitis. Relying upon national laboratory-based surveillance, we reviewed records of human rabies acquired in the United States during 1960–2009. Changes in the epidemiology of human rabies were notable, due to improved animal management, safer and more efficacious biologics, and revisions in prevention guidelines. Historically, domestic animals were the most important source of infection. Since the 1990s, more human cases were associated with rabid bats. Prior to 1980, postexposure prophylaxis failures were reported. After development of modern rabies immune globulin and vaccines, none occurred. Of 75 human cases identified, only four patients survived. Rabies remains an extremely high consequence zoonosis, but the disease is not uniformly fatal, per se. Rabies is essentially preventable when primary exposures are averted, or appropriate prophylaxis occurs before illness.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Rabies is one of the most feared infectious diseases. Annually, tens of thousands of people die from rabies worldwide. Most deaths occur within Asia and Africa, typically following a rabid dog bite. In the United States, aggressive campaigns to vaccinate dogs against rabies began after World War II. As a result, sustained rabies virus transmission in dogs was eliminated, and the last suspected dog bite-associated human rabies case in the U.S. occurred near the Mexican border in the early 1990s. Clearly, the epidemiology of rabies in the United States changed dramatically over the 20th century, as well as basic knowledge towards its prevention and potential treatment. The objective of this paper is to summarize reported human cases of rabies acquired in the United States from 1960 to 2009 [1–59]. Moreover, considering the extreme case fatality associated with this zoonosis, our primary purpose is to review the epidemiology, rabies postexposure prophylaxis (PEP) failures, clinical presentations, laboratory findings, and outcomes of human rabies cases acquired in the United States over the past 50 years, to provide an insight to the question if rabies should be considered a uniformly lethal disease.
Methods
We identified human cases of rabies acquired in the United States in the Morbidity and Mortality Weekly Report from 1960 to 2009 and records at CDC. Additionally, we conducted literature searches for other cases over this period. Case reports were tabulated.
Exposure histories were characterized as domestic animal bites, non-domestic (wild) animal bites, domestic or wild animal contact without an identified bite, bat related exposures (including bat bites, bat contact without an identified bite, a bat in the house, or other close proximity to a bat), laboratory exposures, transplant exposures, or no identified exposure. Imported human rabies cases from exposures abroad or rabies virus variants found outside the United States were excluded.
The clinical course was separated into three categories: 1) encephalitic form characterized by loss of cognitive functions, usually with agitation; 2) paralytic form, characterized by focal or quadriparesis with initial normal cognitive function; and 3) atypical presentation, characterized by focal pain, cranial nerve palsies, and seizures [60].
All cases were confirmed through laboratory diagnostic testing (performed by CDC and/or a state laboratory) by one of the following: 1) detection of rabies virus antibodies in the serum of an individual with no history of rabies immunization or in CSF, regardless of immunization status; 2) detection of rabies virus antigens by immunofluorescence (FA) or histology/electron microscopy in a skin biopsy of the neck, corneal impressions, or brain tissue; 3) detection of rabies virus RNA by RT-PCR in saliva, skin biopsy, or brain tissues; and 4) rabies virus isolation from saliva, tears, skin biopsy, or brain tissues [60–65].
Results
Human Rabies Cases Acquired in the United States (1960–2009)
From 1960 to 2009, records were reviewed from 75 cases of human rabies (Table 1). These included cases with an identified bite from a rabid or potentially rabid animal (29 cases), cases secondary to laboratory exposures (2 cases), cases due to tissue transplantation (5 cases from 2 separate donors), cases of contact with a sick or wild animal without an identified exposure (6 cases), cases with bat contact but without an identified exposure (14 cases), cases with a history of a bat in the house without identified exposure (2 cases), cases with bats observed out of the home without identified exposure (4 cases), and cases with no known exposures (13 cases).
Cases from known domestic or wild carnivore bites occurred only in the first and second decades (1960–1979). Patients developed rabies after bat bites in all five decades (1960–2009). Rabies following bat contact, but without a reported bite, occurred in recent decades (1990–2010). Cases without an identified exposure were found over the last four decades. Overall, 24/75 (32 %) were in the pediatric age group (≤ 18 years of age) and 12 of these 24 (50 %) were <10 years of age. The mean age was 29 years (range 2 to 82 years of age). A male gender-bias was apparent in all five decades, while children predominated in the first (1960–1969) decade.
Initial symptoms were listed for 65 of 75 patients (clinical descriptions were not obtained for 10 patients). Many of these 65 patients presented first to emergency care or primary care with non-specific complaints, including focal pain and/or paresthesias (34/65, 52 %), vomiting and headache (13/65, 20 %), sore throat or dysphagia (10/65, 15 %), malaise (5/65, 8 %), and confusion and/or agitation (3/65, 5 %). Most of these 65 patients were discharged home, including 15 who were diagnosed with upper respiratory infections, given antibiotics, and discharged. All 65 patients were hospitalized ultimately, usually within 7 days of their presentation.
Documented Bites Preceding Rabies and Failures of Prophylaxis
Documented bites from carnivores and development of rabies (13 cases) occurred from 1960 to 1979. Animals included dogs (5 cases), a cat (1 case), skunks (4 cases), foxes (2 cases), and a bobcat (1 case). Documented bat bites resulting in rabies (16 cases) occurred over all five decades. Of these 29 subjects who developed rabies following bites, 14 (48 %) did not receive rabies PEP, 12 (41 %) received partial rabies PEP, and 3 (10 %) received the recommended PEP. The partial rabies PEP included duck embryo vaccine (DEV) without rabies immune globulin (RIG). The last patient to develop rabies after PEP was in 1979. Since 1979, DEV was replaced by more effective tissue culture vaccines, and no documented rabies PEP failures have been reported in the United States.
Initial Suspicion and Laboratory Findings
For 63 patients, some description was obtained of clinical course after hospitalization. On admission, temperature was reported in 42 patients and 37 (88 %) were febrile. The initial serum white blood cell count (WBC) was reported for 23 patients and mean WBC was 13,880/mm² (range 7,700–20,000/mm²) with 78 % polys (range 65–91 %). The initial CSF findings were reported for 45 patients, and for 39 (87 %) the CSF was abnormal. The WBC was elevated (> 5/mm²) for 34/45 patients with a mean of 98 (range 6–1,000/mm²) and 19 % polys (range 0–67 %). The CSF protein was elevated (> for 40 mg/dL) for 27/32 subjects, with a mean of 99 (range 50–178 mg/dL). One patient had a low CSF glucose (24 mg/dL) but simultaneous serum glucose was not reported.
Initial diagnosis at the time of hospitalization included encephalitis of unknown etiology, meningitis, stroke, weakness, transverse myelitis, Guillain-Barré syndrome, subarachnoid hemorrhage, myocardial infarction, vomiting/dehydration, abdominal obstruction, glossitis/pharyngitis, and tetanus. Over the course of hospitalization, patients evolved clinically (63 patients) into what fit best as encephalitic rabies (46 patients), paralytic rabies (9 cases), or atypical rabies (8 cases). Rabies was not suspected during the hospitalization for 17 of these patients. Hence, encephalitic/paralytic/atypical rabies was not considered until postmortem.
Seven of 46 patients with encephalitic rabies were combative and required sedation or restraints. In addition, a 2-year-old boy (patient #10) “in a sudden outburst of rage” bit his mother. His mother received rabies PEP and remained well. This was the only official report of any of the 75 subjects with rabies biting another human. Most of the 46 subjects with encephalitic rabies were described as disoriented, agitated, and/or lethargic.
Clinical manifestations of nine patients fit best into the category of paralytic rabies. They were initially thought to have strokes, transverse myelitis, myelitis, or Guillain-Barré syndrome.
Eight patients had so-called atypical clinical manifestations of rabies. These included focal neuropathies, cranial nerve palsies, and an initially clear sensorium that evolved into seizures.
Rabies Diagnostic Confirmation
Rabies was confirmed by documenting rabies virus antigens or isolates in corneal impressions, saliva, neck skin biopsy, or brain biopsy. Multiple tests were usually conducted for each of the 75 patients. The diagnosis was attempted antemortem in 43 patients, with supportive results in 37 (86 %) (Table 2). The sensitivity of antemortem testing by decade was: 2/3 in 1960–1969; 7/8 in 1970–1979; 2/2 in 1980–1989; 11/14 in 1990–1999; and 15/16 in 2000–2009. Detection using corneal impressions occurred in 7/12 (58 %) samples; virus isolation and/or PCR from saliva in 19/30 (63 %); nuchal skin biopsies in 14/27 (52 %); and brain biopsies in 2/4 (50 %). Four patients survived and in each case rabies was confirmed by antibody testing only.
Postmortem evaluation of brain tissue included detection of antigens or amplicons in 36/38 (95 %); microscopic neuronal intracytoplasmic inclusions or virions detected by electron microscopy 23/28 (82 %); and isolation in 13/15 (87 %). In addition, positive postmortem findings occurred in 2/3 saliva samples, 1/2 corneal impressions, and 2/4 nuchal skin biopsies.
Rabies Virus Variants
Monoclonal antibody typing or molecular sequencing was used for determining the rabies virus variant for 51/75 (68 %) patients. Forty-five were associated with bats, two with skunks, two with dogs, one with a raccoon, and one with a coyote rabies virus variant. Two were likely laboratory strains (subjects #30 and #31), and 22 were not determined because testing was not available or no viral isolate was recovered for testing. Bat viruses were the majority (45/51, 88 %) of the identified variants. Clinically, bat contacts were involved with 35/75 (47 %) patients. Of these 35, 29 had viral characterization and all were bat rabies virus variants. In addition, 5 patients with transplant-related rabies were bat-associated.
Bat bites preceding rabies (16 patients) occurred at least once in all five decades of study. Bat contact without a known bite preceded rabies (14 patients) in only the last two decades.
Thirteen patients had undefined exposures. These occurred in the last four decades. The rabies virus variant was identified in 12 of these 13 patients and included bat rabies viruses in nine, and one each with skunk, dog and a raccoon variant.
Survivors
Case 1 (Patient #13).
A 6-year-old boy was bitten by a bat on his left thumb in October, 1970. The bat remained attached until the father removed it. The bat was diagnosed rabid. The child was given 14 doses of DEV, but no RIG. Two days after completing DEV, the patient developed neck pain, fever, vomiting and was hospitalized. Rabies was initially not suspected until the child developed a left-sided weakness followed by unresponsiveness. Rabies virus antibodies were detected in the serum and CSF. Serum neutralization titers peaked at 1:63,000 whereas most people demonstrated titers of 1:32 (and rarely above 1:600) after DEV immunization. This antibody response was considered indicative of clinical rabies and not a post-vaccine effect. No inclusions (Negri bodies) were found in a brain biopsy and no rabies virus was isolated from viral culture of brain tissue. The child was intubated and comatose for 10 days, was extubated and gradually returned to normalcy over the next 3 months.
Case 2 (Patient #31).
In March, 1977, a 32-year-old laboratory technician was exposed to a rabies virus aerosol. Two weeks later, he developed malaise, headaches, fever, lethargy, and was hospitalized. During the next 3 days, he became comatose and was intubated. He had received pre-exposure rabies vaccination during 1968, followed by yearly boosters. His last rabies vaccine booster was November, 1976. Two weeks after this booster his rabies virus serum neutralization titer was 1:32. Upon illness, rabies virus antibodies were detected in his serum (1:64,000) and CSF (1:16,225), supportive of an acute rabies virus infection. No rabies virus antigens were detected in corneal impressions or a nuchal skin biopsy. The patient survived, but with severe neurologic sequelae.
Case 3 (Patient #26).
In September, 2004 a 15-year-old girl was bitten on the left index finger while handling a bat. The wound was washed, but no medical care was sought. One month later, she developed fatigue and left hand paresthesia. Over the next 3 days, she experienced vomiting, 6th cranial nerve palsies, fever, lethargy, and was hospitalized. Rabies virus antibodies were found in her CSF, increasing from 1:32 to 1:2,048. No rabies virus antigens were detected in a nuchal skin biopsy. Specific treatment included induction of coma, ketamine, midazolam, ribavirin, and amantadine (later termed the ‘Milwaukee protocol’). No rabies vaccine or immunoglobulin was administered. After 4 weeks of induced coma, her medications were tapered and after intensive rehabilitative therapy over the next year she made a complete recovery.
Case 4 (Patient #55).
In February, 2009, a 17-year-old female presented to the emergency department with a 2 week history of headache, fever, vomiting, and paresthesias. A lumbar puncture revealed lymphocytic meningitis (WBC of 163/mm3, 97 % lymphocytes). She was hospitalized, 3 days later felt better, no isolates were obtained from routine cultures, and she was discharged. A week later she returned with headache, vomiting and left-sided weakness. A repeat lumbar puncture showed lymphocytic meningitis (WBC of 185/mm3, 95 % lymphocytes) and her CSF pressure was increased. She reported a history of contact with flying bats after entering a cave in Texas 2 months before illness onset but had never received rabies prophylaxis. Rabies virus antibodies were found in her serum (1:8,192) and CSF (1:32), indicative of an acute rabies virus infection. Neither viral antigens nor amplicons were detected in submitted samples. One dose of rabies vaccine and 1,500 IU of HRIG were administered following detection of rabies virus antibodies but additional doses were held due to concerns for possible adverse events from immune stimulation. She was treated supportively without intensive care and was discharged a week later. She returned the next week with worsening headache. A third lumbar puncture was performed, which relieved the headache. After this last visit she was lost to follow-up.
Case 5 (Reference #100).
In May 2011, an 8-year-old girl in California presented to a local emergency department with a 1-week history of progressive sore throat, difficulty swallowing, and weakness. After developing flaccid paralysis and encephalitis, diagnostic laboratory testing detected of rabies virus–specific antibodies in serum and CSF. Despite extensive testing, no likely alternative diagnosis was identified. The patient recovered after receiving advanced supportive care, including treatment with therapeutic coma. The patient had no history of rabies vaccination and received no rabies biologics during the course of her treatment. Scratches from at least two free-roaming, unvaccinated cats at the patient’s school were identified as a possible source of infection.
Discussion
“Rabies” comes from a Latin term, meaning rage or fury, and is one of the oldest recorded infectious diseases. Rabies virus is a highly neurotropic RNA virus in the family Rhabdoviridae and genus Lyssavirus, and the only lyssavirus detected in the New World [60, 64]. To date, more than a dozen putative lyssavirus species/genotypes have been recorded. All lyssaviruses result in an acute, progressive encephalitis, and most have been documented as human pathogens. After a bite or mucous membrane exposure, virions infect peripheral nerves, uncoat, and travel via retrograde axoplasmic transport to the spinal cord and brain at a rate of 50 to 100 mm/day [64]. After replication in the central nervous system, viral spread occurs throughout the body, including the salivary glands, cornea, the skin of the neck, and other innervated areas. Incubation period is usually 4 to 6 weeks, but periods of longer than a year have been reported. Incubation periods of 2 weeks or less have been observed in patients with severe bites to the head and face [66, 67].
Death is an expected, but not uniform, outcome, occurring on average 2 weeks after onset of symptoms [68]. Manifestations of the acute neurological phase are grouped into three forms: encephalitic (“furious rabies”), paralytic (“dumb rabies”) or atypical rabies. A severe encephalitic form matches the stereotypical image of the “mad” dog and is uncommon in humans [69]. Humans with encephalitic rabies may show agitation, altered mental state, hydrophobia, dysphagia, hyper salivation, and signs of autonomic dysfunction. In the paralytic form patients exhibit muscle weakness that rapidly deteriorates into flaccid paralysis. Early signs and symptoms for both presentations are non-specific, including fever, malaise, focal or generalized weakness, difficulty swallowing, headache, and pain or paresthesias in the area of the wound [60, 69].
Dogs are the most important global reservoirs from a public health perspective. Important wild carnivores include foxes, skunks, raccoons, mongooses and jackals. Infected Chiroptera have been documented on all inhabited continents, including insectivorous, frugivorous, and vampire bats (Latin America) [70].
Rabies Epidemiology
During 1950–1959, 99 cases of human rabies were acquired in the United States. Most were the result of a bite from a rabid domestic animal. In the 1950s and 1960s intense public health efforts to vaccinate dogs made canine rabies uncommon, and cases in humans plummeted [71, 72]. Over the last five decades, rabies cases in humans evolved from an infection acquired via exposure to rabid domestic or wild carnivores (usually in children) to an infection acquired from bats (children and adults, in equal proportion).
Bats were first reported rabid in the United States during the 1950s [73]. The importance of bat rabies was better appreciated after the development of monoclonal antibody typing techniques that allowed identification of the likely reservoir source of infection. Domestic or wild carnivores rarely are found infected with bat rabies viruses [73]. The last human rabies cases involving documented bites from a domestic animal occurred in 1975–1979, identified as rabies virus variants associated with skunks and dogs. Of 19 cases involving bat exposures without a documented bite (1990–2009), 17 were bat-associated variants, and 2 did not have a rabies virus variant identified.
Rabies Diagnosis
Human rabies is a rare disease in the United States. Not surprisingly, rabies is often not considered during early course of illness. Furthermore, initial signs are often nonspecific, including focal pain and/or paresthesias, headache, vomiting, sore throat and/or dysphagia. Even after hospitalization, rabies may not be considered. For two patients (one who died of presumed Guillain-Barré syndrome, and the other of presumed subarachnoid hemorrhage) rabies was only considered when recipients of their tissues developed rabies. Presumably, other cases of human rabies have occurred in the United States and were not identified.
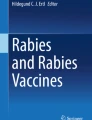
Specific laboratory diagnosis requires demonstration of rabies virus antigens, isolates, detection of rabies virus nucleic acids, or the presence of rabies virus antibodies in the serum of unvaccinated individuals, or CSF, irrespective of vaccination status. Postmortem examination of the brain reaches 100 % sensitivity. During the last 50 years, antemortem detection of rabies virus was attempted in less than half of patients reported with rabies. Saliva samples were useful in 13/16 (81 %), corneal impressions in 9/13 (69 %), and nuchal skin biopsies in 14/25 (56 %) (Fig. 1). Over this period, methods for detecting rabies virus infection have improved. Tissue culture for the isolation of virus has replaced laboratory animals, RT-PCR with sequencing augments antigen testing, and electron microscopy can identify virions during pathogen detection. Testing of antemortem nuchal biopsies was ≥98 % sensitive, and three successive saliva specimens were 100 % sensitive in one study using a heminested RT-PCR assay [74].

Microscopic image of a cryostat section of a human skin biopsy showing fluorescent rabies virus inclusions in a hair follicle (photograph courtesy of Michael Niezgoda)
Bat-Associated Rabies (1990–2010)
Over the last two decades (1990–2010), 45 human cases of rabies were acquired in the United States. Of these, 42 (89 %) were rabies virus variants associated with bats. Ten were due to bat bites, 14 had bat contact, 6 had bats in their homes or neighborhoods, 4 followed transplants from a donor with a bat bite, and 6 had no documented exposures. In addition, patient #32 had contact with a sick cow and patient #35 had contact with a sick kitten.
In 1995, a 4-year-old child in Washington and a 13-year-old child from Connecticut died of rabies [37, 38]. The 4-year-old had a bat in her room and the 13-year-old had a bat downstairs while she slept upstairs. Neither had identified bat contact. Before 1995, rabies PEP was recommended for a bat exposure only when a bite or non-bite exposure had occurred. Following these cases, CDC updated recommendations to include consideration of PEP “in situations in which a bat is physically present and the persons(s) cannot exclude the possibility of a bite” unless prompt testing of the bat has ruled out rabies. Thus, a bat in the house with a child or a sleeping family member could result in PEP. Unfortunately, a bat in the house is a common scenario. In 2009, De Serres et al. reviewed the risks of house bat exposures without identified contact and concluded that more than one million people would need PEP at a cost of over a billion dollars to prevent a case of rabies [73]. Current Advisory Committee on Immunization Practices (ACIP) guidelines for human rabies prevention state: “situations that might qualify as exposures include finding a bat in the same room as a person who might be unaware that a bite or direct contact has occurred” [61]. Thus, simply finding a bat in the house does not require PEP, but a bat found in the same room as a person should be investigated thoroughly.
Rabies Postexposure Prophylaxis
Rabies is preventable with proper administration of modern rabies PEP, combining active and passive immunization [61, 62, 75–77]. Two rabies vaccines are commercially available in the United States: the human diploid cell culture vaccine (HDCV) and the purified chick embryo vaccine (PCEV). These vaccines are highly effective and safe, rarely causing serious adverse events [61, 62]. The older vaccine DEV was used during the 1960–70s, a period when at least 27 people developed rabies. Eleven of these received vaccinations with DEV alone, but no RIG, while five patients received vaccination with DEV plus RIG. Since introduction of modern cell culture rabies vaccines and RIG during the 1980s, no failures of rabies PEP have been reported in the United States. Rabies PEP is composed of one dose of RIG and four or five doses of HDCV or PCEC vaccine. A 4-dose vaccine regimen is recommended by the ACIP [76•].
Indications for PEP have changed little over the last five decades in the United States. Rabies PEP is recommended for bite exposures from suspect rabid animals or non-bite exposures involving contamination of an open wound, scratch, or mucous membrane with saliva or nervous tissue from a potentially rabid animal [61]. Evaluation is indicated for direct bat contact, since a person may not recognize the risk and lesions could be minimal [78]. Changes in recommendations for rabies PEP in the last two decades include: 1) rabies PEP may not be needed for a provoked bite by a well-appearing stray dog in some areas of the United States which are free of rabies in carnivores, 2) rabies PEP should be considered if a bat is found in the room of a sleeping person or a person who cannot report contact [76•].
Historically, rabies vaccines derived from nerve tissue (NTV) caused severe swelling and was administered subcutaneously in the abdomen. These NTV were associated with rare but serious neuroparalytic reactions and were less potent than modern cell culture vaccines. While NTV have been discontinued gradually over the past 50 years they are still used in some developing countries [61, 63, 65]. Patient # 10, who failed PEP with DEV plus RIG, bit his mother. His mother was given PEP with DEV and NTV plus RIG and survived. Likely, the NTV was selected because her son failed PEP with DEV.
Unfortunately, after even the remotest of rabies virus exposures (e.g. washing saliva from any pet) some medical providers may advocate rabies PEP. A clear understanding of rabies virus pathogenesis, current PEP guidelines, and basic rabies epidemiology can be used to reassure patients and avoid unnecessary PEP.
Survivors of Rabies
Historically, rabies was recognized as a fatal infection in humans. Without medical intervention, exposed persons develop severe encephalopathy, paresis, and death, usually within 7–14 days. With intensive care, the longest fatal case (patient #10) survived 133 days prior to succumbing to infection. Besides patients in the United States, several other patients have survived rabies [79]. Of these survivors, most received some form of rabies vaccination before developing symptoms. Two patients survived rabies and did not receive any PEP prior to onset of symptoms (patients #25 and #53). The first reported survivor without rabies vaccination was treated with induction of coma and anti-viral drugs, while her immune response developed [80]. Initially, she had motor abnormalities which resolved over a year through physical rehabilitation [81]. Unfortunately, attempts to apply this protocol to scores of other rabid patients have failed (http://www.chw.org/display/PPF/DocID/33223/router.asp). Patient #53 survived without intensive care or antiviral agents and is the first reported case of presumptive abortive human rabies.
Conclusions
Rabies remains a high consequence zoonosis, requiring a thorough medical evaluation after animal bite, predicated in part by the species, circumstances, severity, and epizootiology in question. Human cases of rabies are rare in developed countries, such as the United States, despite the presence of enzootic rabies perpetuation among wildlife [82•]. Application of modern prevention and control strategies can limit the extreme mortality associated with this encephalitis [83•]. For example, from 1960 to 1984, human rabies cases acquired in the United States secondary to exposures to carnivores, such as dogs, decreased, while cases associated with wildlife, such as bats, increased, from 1985 to the present time. Moreover, bites by stray dogs prior to the 1970s required the consideration of rabies PEP, while today the United States is free of canine rabies virus transmission, and bites from dogs unavailable for risk assessment (in areas that free of rabies in carnivores) may not require PEP. In contrast, bat exposures need thorough investigation to determine the need for rabies PEP, especially if the bat is not available for diagnostic testing. Rabies PEP in the naïve patient should always entail immediate wound care, RIG infiltration, and administration of rabies vaccine. Following such established guidelines in the United States since 1980, no PEP failures have occurred, despite thousands of human exposures to rabid animals annually. The lapse of medical education about rabies and the ease of global travel present a challenge for developed and developing countries alike [84•, 85, 86]. Despite case reports of a few survivors, rabies is still considered incurable, with no proven treatment [87•, 88•]. However, although controversial, this disease should be viewed as a continuum and basic research and applied clinical insights into viral pathogenesis, animal model development, and experimental therapy may provide the primary evidence necessary for new anti-viral drugs and improved intensive care and management of the rabid patient [89–99, 100•]. Prevention of exposures and proper PEP are key elements to avoid or prevent rabies infection.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
CDC. Human rabies. MMWR. 1960;9:2.
CDC. Human rabies-Kentucky. MMWR. 1961;10:2.
CDC. Rabies-California. MMWR. 1961;10:2.
CDC. Rabies death-Kentucky. MMWR. 1961;10:8.
CDC. Rabies-Texas. MMWR. 1962;11:58.
CDC. Human rabies-Idaho. MMWR. 1962;11:395.
CDC. Human rabies death-Alabama. MMWR. 1963;12:300.
Gomez MR, Siekert RG, Hermann EC. A human case of skunk rabies. JAMA. 1965;194:101–335.
CDC. Human rabies death-West Virginia. MMWR. 1966;15:195.
Bell RG. Death from rabies in a 10 year old boy. South Dakota J Med. 1967;20:28–30.
Rubin RH, Sullivan L, Summers R, Gregg MB, Sikes RK. A case of human rabies in Kansas. J Infect Dis. 1970;122:318–22.
Emmons RW, Leonard LL, DeGenaro F, et al. A case of human rabies with prolonged survival. Intervirology. 1973;1:60–72.
Hattwick MAW, Hochberg FW, Landrigan PJ, Gregg MB. Skunk-associated human rabies. JAMA. 1972;222:44–7.
Hattwick MAW, Weis TT, Stechschute CJ, Baer GM, Gregg MB. Recovery from rabies. Ann Intern Med. 1972;76:931–42.
CDC. Human rabies-New Jersey. MMWR. 1971;20:459–60.
Winkler WB, Fashinell TR, Leffingwell L, Howard P, Conomy JP. Airborne rabies transmission in a laboratory worker. JAMA. 1973;226:1219–21.
CDC. Human rabies-Kentucky. MMWR. 1973;22:325–6.
Sung JH, Hayano M, Mastri AG, Okagaki T. A case of human rabies and ultrastructure of the negri bodies. J Neuropathol Exp Neurol. 1976;35:541–59.
CDC. Human rabies-Maryland. MMWR. 1976;25:235–6.
CDC. Rabies in a laboratory worker-New York. 1977;26:183–184.
CDC. Human-to-human transmission of rabies by a corneal transplant-Idaho. 1979;28:109–11
CDC. Human rabies-Pennsylvania. MMWR. 1979;28:75–7.
CDC. Two suspected cases of human rabies-TX, WA. MMWR. 1979;28:292:297–8.
CDC. Human rabies-Oklahoma. MMWR. 1979;28:476–81.
CDC. Human rabies-Kentucky. MMWR. 1979;28:590–1.
CDC. Two suspected cases of human rabies-Texas, Washington. MMWR. 1979;28:292–8.
CDC. Human rabies-Oklahoma. MMWR. 1981;30:343–9.
CDC. Human rabies-Michigan. MMWR. 1983;32:159–60.
CDC. Human rabies-Pennsylvania. MMWR. 1984;33:633–5.
CDC. Human rabies-Texas. MMWR. 1991;40:132–3.
CDC. Human rabies-Texas, Arkansas, Georgia. MMWR. 1991;40:765–9.
CDC. Human rabies-Texas and California. MMWR. 1994;43:93–6.
CDC. Human rabies-New York. MMWR. 1993;42:799–806.
CDC. Human rabies-Alabama, Tennessee, and Texas. MMWR. 1995;44:269–72.
CDC. Human rabies-California. MMWR. 1994;43:455–7.
CDC. Human rabies-West Virginia. MMWR. 1995;44:86–7.
CDC. Human rabies-Washington. MMWR. 1995;44:625–7.
CDC. Human rabies-Connecticut. MMWR. 1996;45:207–9.
CDC. Human rabies-California. MMWR. 1996;45:353–6.
CDC. Human rabies-Kentucky and Montana. MMWR. 1997;46:397–400.
CDC. Human rabies-Montana and Washington. MMWR. 1997;46:770–4.
CDC. Human rabies-Texas and New Jersey. MMWR. 1998;47:1–4.
CDC. Human rabies- Virginia. MMWR. 1999;48:95–7.
CDC. Human rabies-California, Georgia, Minnesota, Ney York, and Wisconsin. MMWR. 2000;49:111–6.
CDC. Human rabies-Tennessee. MMWR. 2002;51:828–9.
CDC. Human rabies-California. MMWR. 2002;51:686–8.
CDC. Human rabies-Iowa. MMWR. 2003;52:47–8.
CDC. First human death associated with raccoon rabies-Virginia. MMWR. 2003;52:1102–3.
CDC. Human death associated with bat rabies-California, 2003. MMWR. 2004;53:33–5.
CDC. Investigation of rabies Infections in organ donor and transplant recipients-Alabama, Arkansas, Oklahoma, and Texas. MMWR. 2004;53:586–9.
CDC. Recovery of a patient from clinical rabies-Wisconsin. MMWR. 2004;53:1171–3.
CDC. Human rabies-Mississippi. MMWR. 2006;55:207–8.
CDC. http://www.cdc.gov/rabies/resources/news/2006-05-10.html
CDC. Human rabies-Indiana and California. MMWR. 2007;56:361–5.
CDC. Human rabies-Minnesota. MMWR. 2008;57:460–2.
CDC. Human rabies—Missouri. MMWR. 2008;58:1207–9.
CDC. Human rabies-Kentucky/Indiana. MMWR. 2008;59:393–6.
• CDC. Presumptive abortive human rabies-Texas. MMWR. 2010;59:185–190. Report of a teenager exposed to bats in a Texas cave. First suggestion of abortive rabies and recovery without intensive care, possibly related to a low viral dose and non-bite exposure route of infection.
CDC. Human rabies-Michigan. MMWR. 2011;60:437–40.
Hemachudha T, Laothamatas J, Rupprecht CE. Human rabies: a disease of complex neuropathogenetic mechanisms and diagnostic challenges. Lancet Neurol. 2002;1:101–9.
CDC. Human rabies prevention-United States, 2008: recommendations of the Advisory Committee on Immunization Practices. MMWR. 2008;57(No. RR-03):1–26,28.
American Academy of Pediatrics. Rabies. In: Pickering LK, Baker CJ, Long SS, McMillan, editors. Red book report of the committee on infectious diseases, 28th ed. Elk Grove Village, IL: 2009. pages 552–559.
Fishbein DB, Robinson LE. Current Concepts: Rabies. N Engl J Med. 1993;329:1632–8.
Warrell MJ, Warrell DA. Rabies and other lyssavirus diseases. Lancet. 2004;363:959–69.
Plotkin SA. Rabies. Clin Infect Dis. 2000;30:4–12.
Wilde H. Failures of post-exposure rabies prophylaxis. Vaccine. 2007;25:7605–9.
Sudarshan MK, Madhusudana SN, Mahendra BJ, et al. Assessing the burden of human rabies in India: results of a national multi-center epidemiological survey. Int J Infect Dis. 2007;11:29–35.
Soun VV, Eidson M, Trimarchi CV, et al. Antemortem diagnosis of New York human rabies case and review of US cases. Int J Biomed Sci. 2006;2:433–44.
Hemachudha T, Wacharapluesadee S, Mitrabhakdi E, Wilde H, Morimoto K, Lewis RA. Pathophysiology of human paralytic rabies. J Neurovirol. 2005;11:93–100.
World Health Organization. WHO Expert Consultation on Rabies. WHO Tech Rep Ser. 2005;931.
Blanton JD, Robertson K, Palmer D, Rupprecht CE. Rabies surveillance in the United States during 2008. JAVMA. 2009;235:676–89.
Velasco-Villa A, Reeder SA, et al. Enzootic rabies elimination from dogs and reemergence in wild terrestrial carnivores, United States. Emerg Infect Dis. 2008;14:1849–54.
DeSerres G, Dallaire F, Cote M, Skowronski DM. Bat rabies in the United States and Canada from 1950 to 2007: human cases with and without bat contact. Clin Infect Dis. 2008;46:1329–37.
Dacheau L, Reynes J-M, Buchy P, et al. A reliable diagnosis of rabies based on analysis of skin biopsy specimens. Clin Infect Dis. 2008;47:1410–7.
Blanton JD, Bowden NY, Eidson M, Wyatt JD, Hanlon CA. Rabies postexposure prophylaxis, New York, 1995–2000. EID. 2005;11:1921–7.
• CDC. Use of a reduced (4-dose) vaccine schedule for postexposure prophylaxis to prevent human rabies: recommendations of the advisory committee on immunization practices. MMWR. 2010;59(RR-2):1–9. Current guide for human rabies postexposure prophylaxis in the United States. Essential recommendations in managing the exposed patient for use by clinicians.
Rupprecht CE, Gibbons RV. Prophylaxis against rabies. N Engl J Med. 2004;351:2626–35.
Feder Jr HM, Nelson RS, Reiher HW. Bat bite? Lancet. 1997;350:1300.
Jackson AC. Recovery from rabies. N Engl J Med. 2005;352:2549–50.
Willoughby RE, Tieves KS, Hoffman GM, et al. Survival after treatment of rabies with induction of coma. N Engl J Med. 2005;352:2508–14.
Hu WT, Willoughby Jr RE, Dhonau H, Mack KJ. Long-term follow-up after treatment of rabies by induction of coma. N Engl J Med. 2007;357:945–6.
• Blanton JD, Palmer D, Dyer J, Rupprecht CE. Rabies surveillance in the United States during 2010. J Am Vet Med Assoc. 2011;239:773–83. Summarizes the current laboratory-based surveillance of rabies in The United States. Lists the spatial occurrence of animal cases and provides an update of human rabies cases for 2010–11.
• Dacheux L, Delmas O, Bourhy H. Human rabies encephalitis prevention and treatment: progress since Pasteur's discovery. Infect Disord Drug Targets. 2011;11:251–99. Presents a historical and global overview of the progress in human rabies prophylaxis over the past century. Discusses some of the available options to human rabies diagnosis and management.
• Malerczyk C, Detora L, Gniel D. Imported human rabies cases in Europe, the United States, and Japan, 1990 to 2010. J Trav Med. 2011;18:402–7. Details several cases of imported human rabies in both the New and Old World. Suggests that globalization and translocation of cases will continue to create clinical challenges for medical personnel in developed countries unfamiliar with rabies.
• Johnson N, Brookes SM, Healy DM, Spencer Y, Hicks D, Nunez A, Wells G, Fooks AR. Pathology associated with a human case of rabies in the United Kingdom caused by European Bat Lyssavirus Type-2. Intervirology. 2011 Dec 6. [Epub ahead of publication]. Presents a case of human rabies due to a rabies-related lyssavirus. Demonstrates the limitations of the concept of a ‘rabies-free’ country, given the ubiquity of lyssaviruses in bats.
CDC. Human rabies from exposure to a vampire bat in Mexico–Louisiana, 2010. MMWR. 2011;60:1050–2.
• Aramburo A, Willoughby RE, Bollen AW, Glaser CA, Hsieh CJ, Davis SL, Martin KW, Roy-Burman A. Failure of the Milwaukee protocol in a child with rabies. Clin Infect Dis. 2011;53:572–4. Describes treatment of a case of rabies in California. Despite application of an experimental protocol, the child succumbed after 30 days of hospitalization and intensive care.
• Jackson AC. Rabies in the critical care unit: diagnostic and therapeutic approaches. Can J Neurol Sci. 2011;38:689–95. Discusses some of the current controversies in rabies clinical therapy. Reviews potential options for future intervention.
Rawat AK, Rao SK. Survival of a rabies patient. Indian Pediatr. 2011;48:574.
Hooper DC, Roy A, Kean RB, Phares TW, Barkhouse DA. Therapeutic immune clearance of rabies virus from the CNS. Future Virol. 2011;6:387–97.
Smith TG, Wu X, Franka R, Rupprecht CE. Design of future rabies biologics and antiviral drugs. Adv Virus Res. 2011;79:345–63.
• Franka R, Rupprecht CE. Treatment of rabies in the 21st century: curing the incurable? Future Microbiol. 2011;6:1135–40. Lists some of the approaches used to treat human rabies cases. Presents a comparison of variables related to virus, dose, route, and host characteristics, in support of the thesis that rabies is a continuum of outcomes related to the complex temporal and biomedical dynamics of each case.
Willoughby RE, Roy-Burman A, Martin KW, Christensen JC, Westenkirschner DF, Fleck JD, Glaser C, Hyland K, Rupprecht CE. Generalised cranial artery spasm in human rabies. Dev Biol (Basel). 2008;131:367–75.
Willoughby RE, Opladen T, Maier T, Rhead W, Schmiedel S, Hoyer J, Drosten C, Rupprecht CE, Hyland K, Hoffmann GF. Tetrahydrobiopterin deficiency in human rabies. J Inherit Metab Dis. 2009;32:65–72.
Rubin J, David D, Willoughby Jr RE, Rupprecht CE, Garcia C, Guarda DC, Zohar Z, Stamler A. Applying the Milwaukee protocol to treat canine rabies in Equatorial Guinea. Scand J Infect Dis. 2009;41:372–5.
• Hunter M, Johnson N, Hedderwick S, McCaughey C, Lowry K, McConville J, Herron B, McQuaid S, Marston D, Goddard T, Harkess G, Goharriz H, Voller K, Solomon T, Willoughby RE, Fooks AR. Immunovirological correlates in human rabies treated with therapeutic coma. J Med Virol. 2010;82:1255–65. A case is described of a 37-year-old woman exposed to rabies virus in South Africa. The patient was treated with a therapeutic coma according to the “Milwaukee protocol,” which failed to prevent her death. Rabies virus was isolated from CSF and saliva, antibody was demonstrated in serum and csf, and postmortem specimens demonstrated the presence of antigens, viral RNA, and rabies virus isolates in the CNS.
• Hamir AN, Niezgoda M, Rupprecht CE. Recovery from and clearance of rabies virus in a domestic ferret. J Am Assoc Lab Anim Sci. 2011;50:248–51. Describes a case of spontaneous recovery after experimental rabies virus infection. Provides evidence of viral clearance from the CNS.
Jackson AC, Warrell MJ, Rupprecht CE, Ertl HC, Dietzschold B, O’Reilly M, Leach RP, Fu ZF, Wunner WH, Bleck TP, Wilde H. Management of rabies in humans. Clin Infect Dis. 2003;36:60–3.
Willoughby Jr RE. A cure for a rabies? Sci Am. 2007;296:88–95.
• CDC. Recovery of a patient from clinical rabies - California, 2011. MMWR 2012;61:61–5. This report details the latest survivor from rabies in the United States, after application of experimental treatment. The child was exposed to a suspect cat that was lost to follow-up. Treatment included extreme intensive care, coma induction, and anti-viral drugs.
Acknowledgments
The authors thank all of the local, state, and national health care professionals and health departments whose combined efforts have contributed to the surveillance, diagnosis and care of human rabies patients, and those researchers whose work support biomedical insights into the prevention, control, and treatment of rabies.
The views expressed in this paper represent the authors and not necessarily their home institutions.
Use of commercial or trade names is for comparison purposes only and does not constitute endorsement by the authors or their institutions.
Disclosure
No potential conflicts of interest relevant to this article were reported.
Author information
Authors and Affiliations
Corresponding authors
Rights and permissions
About this article
Cite this article
Feder, H.M., Petersen, B.W., Robertson, K.L. et al. Rabies: Still a Uniformly Fatal Disease? Historical Occurrence, Epidemiological Trends, and Paradigm Shifts. Curr Infect Dis Rep 14, 408–422 (2012). https://doi.org/10.1007/s11908-012-0268-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11908-012-0268-2