
Abstract
This report details the development, validation, and utility of the Diabetes Prevention Trial-Type 1 (DPT-1) Risk Score (DPTRS) for type 1 diabetes (T1D). Proportional hazards regression was used to develop the DPTRS model which includes the glucose and C-peptide sums from oral glucose tolerance tests at 30, 60, 90, and 120 min, the log fasting C-peptide, age, and the log BMI. The DPTRS was externally validated in the TrialNet Natural History Study cohort (TNNHS). In a study of the application of the DPTRS, the findings showed that it could be used to identify normoglycemic individuals who were at a similar risk for T1D as those with dysglycemia. The DPTRS could also be used to identify lower risk dysglycemic individuals. Risk estimates of individuals deemed to be at higher risk according to DPTRS values did not differ significantly between the DPT-1 and the TNNHS; whereas, the risk estimates for those with dysglycemia were significantly higher in DPT-1. Individuals with very high DPTRS values were found to be at such marked risk for T1D that they could reasonably be considered to be in a pre-diabetic state. The findings indicate that the DPTRS has utility in T1D prevention trials and for identifying pre-diabetic individuals.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Determining the risk of type 1 diabetes (T1D) is essential for establishing inclusion criteria for T1D prevention trials [1, 2•, 3•], since individuals must be at sufficient risk to warrant exposure to the experimental interventions. This is a particularly important consideration in children. Moreover, as an indicator of the extent of progression to T1D, risk could help define stages of progression in which an intervention might be most efficacious and useful.
The risk of T1D is related to immunologic, genetic, and metabolic factors. Earlier studies have shown that pancreatic autoantibodies, HLA haplotypes, the first-phase insulin response (FPIR), and impaired glucose tolerance are predictive of T1D [4–7]. More recently, Ziegler et al. [8] pooled data from several studies [Colorado Diabetes Autoimmune Study in the Young (DAISY), Finnish Type 1 Diabetes Prediction and Prevention (DIPP), BABYDIAB, and BABYDIET] to show that the risk of T1D increases according to the number of autoantibodies that develop after seroconversion in children. Children who developed multiple autoantibodies were at a very high 10-year risk of progression to T1D. These findings are consistent with a previous study of Diabetes Prevention Trial-Type 1 (DPT-1) and the TrialNet Natural History Study (TNNHS) participants [9]. In the study of Ziegler et al. [8], following seroconversion, HLA genotypes were further predictive of risk. DPT-1 findings have revealed that in addition to glucose abnormalities such as impaired glucose tolerance, glycemia within the normal range is predictive of T1D [10]. C-peptide indices have also been shown to be predictive of T1D [10].
Previous prevention trials [1, 2•, 3•] have utilized such findings, especially with regard to autoantibodies and glycemia, to define T1D risks of potential participants. Thresholds of individual risk factors, sometimes combined in complex algorithms, have been utilized for this purpose. In order to simplify and provide a more accurate assessment of T1D risk, we have developed a risk score for T1D from DPT-1 data. The DPT-1 risk score (DPTRS) incorporates several predictors of T1D into one measure [11•]. The development, validation, and utility of the DPTRS are detailed below.
Development of the DPTRS
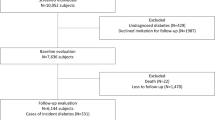
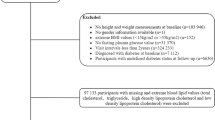
DPT-1 consisted of two clinical trials: the parenteral insulin (n = 339) and oral insulin trials (n = 372) [2•, 3•]. The main objective of each trial was to test whether the intervention could delay the development of T1D in islet cell antibody (ICA)-positive non-diabetic relatives of patients with T1D (age range 1–45 years). Participants in the parenteral trial either had dysglycemia [impaired fasting glucose, impaired glucose tolerance, and/or a glucose level ≥200 mg/dl at 30, 60, or 90 min of an oral glucose tolerance test (OGTT)] or a low FPIR. Oral insulin trial participants were required to have a normal OGTT and insulin autoantibodies (in addition to ICA). Diagnoses were made through 2-h oral glucose tolerance test surveillance at 6-month intervals or by clinical presentation. In both trials, 92 % of those included were first-degree relatives. No overall therapeutic effect was evident in either trial.
In an analysis of DPT-1 data [10], it was evident that the area under the curve (AUC) glucose from OGTTs was a more accurate predictor of T1D than the standard fasting and 2-h glucose indices. Also, among DPT-1 participants within the normal range of glycemia, glucose levels strongly predicted T1D. Moreover, log fasting C-peptide values were positively predictive and AUC C-peptide values were negatively predictive of T1D.
This information was taken into account when the DPTRS [11•] was developed with proportional hazards modeling. We used the metabolic measures from the prior study (sums from baseline OGTT values at 30, 60, 90, and 120 min were used instead of the AUC glucose, since they correlated almost perfectly with the AUC measures and were easier to calculate.) The entirety of the non-diabetic range of glycemia was used rather than categories of glycemia. The final proportional hazards model included age (negatively predictive), log BMI (positively predictive), log fasting C-peptide (positively predictive), and glucose (positively predictive) and C-peptide sums (negatively predictive). The full proportional hazards model for the DPTRS is shown in Table 1. The DPTRS can be calculated in the following manner:
Although the FPIR was also a predictor of T1D, it was not included in the final DPTRS model for two reasons. Firstly, the FPIR had little impact on prediction when the other variables were included in the DPTRS model, and secondly, it would have necessitated the performance of intravenous glucose tolerance tests.
Validation of the DPTRS
An internal split-sample validation within the DPT-1 data showed that the DPTRS model, developed in one sample of the DPT-1 participants, was accurately predictive of T1D in the other samples. The final DPTRS [11•] was based on the same variables but derived from all of the individuals studied.
An external validation was performed using the TrialNet Natural History Study (TNNHS) cohort [12]. The TNNHS is the central core of TrialNet, an international consortium of researchers studying the prevention of T1D. As in DPT-1, TNNHS participants are also autoantibody-positive relatives (91 % first-degree) of patients with T1D (age range 1–45 years). However, in the TNNHS, entry is based on positivity of GAD65, IA2A, and mIAA autoantibodies. More recently, ZnT8A autoantibodies have also been measured. TNNHS participants who qualify can participate in prevention trials; otherwise, TNNHS participants did not receive experimental interventions. The diagnostic surveillance of T1D with OGTTs was similar to DPT-1.
Figure 1 shows that when the DPTRS was used for prediction in the TNNHS cohort (mean ± SD age = 18.5 ± 13.3 years), the 2 and 3-year risks for DPTRS values were similar to those in the DPT-1 cohort (age = 13.9 ± 9.6 years) [12]. There were no significant differences in the cumulative incidence curves between DPT-1 and the TNNHS at any of the DPTRS intervals. Since the autoantibody criteria for entry into the TNNHS differed from DPT-1, the findings suggested that the DPTRS could be accurately predictive across autoantibody-positive populations.

Shown are the 2-year (a) and 3-year (b) risk estimates for T1D according to intervals of the DPTRS in DPT-1 and the TNNHS. There were no significant differences between DPT-1 and the TNNHS at any of the DPTRS intervals. (With permission from: Copyright 2014 American Diabetes Association. From Diabetes Care®, Vol. 34, 2011; 1785–1787. Reprinted by permission of The American Diabetes Association) [12]
Applications of the DPTRS
Selecting Target Populations for Prevention Trials
Since autoantibody positivity occurs infrequently, even in relatives of patients with T1D, it is essential to include as many individuals as possible who truly qualify for entry into prevention trials. Also, since the experimental interventions could have adverse reactions, the erroneous inclusion of individuals in trials must be avoided. Thus, it is important to minimize risk misclassification and the DPTRS can be helpful in this regard.
The utility of the DPTRS for identifying potential prevention trial participants was examined in the TNNHS cohort [13]. Those with normoglycemia and DPTRS values >7.00 were found to have a similar degree of risk as those with dysglycemia (Fig. 2). Moreover, the DPTRS identified a number of individuals with dysglycemia who were actually not at high risk. Those with dysglycemia and a DPTRS value <7.00 [94/221 (43 %)] had an overall 3-year risk estimate of only 0.16.

Shown are cumulative incidence curves for T1D for those normoglycemic with DPTRS values >7.00 and those with dysglycemia. The curves were not significantly different. (With permission from: Copyright 2014 American Diabetes Association. From Diabetes Care®, Vol. 37, 2014; 979–984. Reprinted by permission of The American Diabetes Association) [13]
The normoglycemic TNNHS participants with DPTRS values >7.00 were much younger than those with dysglycemia (8.1 ± 4.9 years vs. 19.6 ± 14.3 years; p < 0.001). In an additional analysis, we have found that among the TNNHS participants with dysglycemia, those with DPTRS values >7.00 were much younger than those with values <7.00 (11.6 ± 8.1 years vs. 30.4 ± 13.8 years; p < 0.001). Thus, the findings showed that the DPTRS can be used to identify those higher risk children who would be missed by using dysglycemia as an indicator of risk, and among those with dysglycemia, it can help to identify those adults who are less likely to progress to T1D. It is apparent that through the inclusion of age, the DPTRS can refine risk estimates.
The findings also showed that the DPTRS was a more consistent indicator of risk than dysglycemia across autoantibody populations. This is evident in Fig. 3 [13] which shows that there was appreciably less difference between the DPT-1 and TNNHS cumulative incidence curves for T1D among those with DPTRS values >7.00 (n.s.) than for those with dysglycemia (p < 0.001).

Shown are comparisons of cumulative incidence curves for T1D between the DPT-1 and TNNHS cohorts for individuals with DPTRS values >7.00 (a) and individuals with dysglycemia (b). The curves are more consistent between DPT-1 and the TNNHS for those with DPTRS values >7.00 than for those with dysglycemia. Whereas the curves for dysglycemia were significantly different between the cohorts, the curves for those with DPTRS values >7.00 were not significantly different. (With permission from: Copyright 2014 American Diabetes Association. From Diabetes Care®, Vol. 37, 2014; 979–984. Reprinted by permission of The American Diabetes Association) [13]
Table 2 shows how DPTRS thresholds could be used to select potential participants for prevention trials [13]. The DPTRS could define high-risk populations in a more flexible and efficient manner than the use of dysglycemia alone. For example, although the risk of T1D in the TNNHS was similar between those with a DPTRS threshold >6.50 and those with dysglycemia, there were many more individuals with a DPTRS threshold >6.50 DPTRS (n = 344) than those with dysglycemia (n = 221).
Identification of Individuals at Very High Risk for T1D
An inspection of Fig. 1 [12] shows that the risk of T1D increases markedly with small increments in DPTRS values above a value of 7.00. This suggested that DPTRS thresholds could identify individuals who would almost inevitably progress to T1D. This possibility was examined in DPT-1 and TNNHS participants with DPTRS values >9.00 [14]. The findings showed that when the 9.00 DPTRS value was exceeded during follow-up, the subsequent 2-year risk of T1D was extremely high (0.88 in DPT-1 and 0.77 in the TNNHS). This suggests that a very high DPTRS threshold could define a pre-clinical state of T1D, if not T1D itself. Thus, there appears to be a point of transition at which a predictor actually becomes an indicator of T1D.
Limitations
There are limitations to the use of the DPTRS. It should be emphasized that since the DPTRS was developed and validated in autoantibody positive populations, it might not be applicable to other populations. Since there can be marked heterogeneity even among autoantibody-positive populations [15], the DPTRS might not always be applicable to specific subgroups. In addition, HLA haplotypes were not assessed for inclusion in the DPTRS. It is possible that they could have provided additional predictive information.
Conclusions and Implications for the Future
The utility of the DPTRS for predicting T1D should provide an impetus for the development of even more accurate risk predictors. In a recent study, combining an autoantibody risk score with the DPTRS provided a slightly more accurate prediction of T1D than the DPTRS alone [16]. The autoantibody risk score accounts for the specific autoantibodies that are positive along with their levels or titers.
The very strong likelihood of being diagnosed with T1D for those above high DPTRS thresholds suggests that risk scores can also contribute to refining the definition of T1D. Even though the DPTRS is useful for present purposes, it is likely to be a forerunner of other risk scores that will be utilized for the prediction of T1D. Such risk scores could be applicable to more populations. In addition, they could more precisely identify those who will develop T1D and when it will occur.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance
Gale EA, Bingley PJ, Emmett CL, Collier T, the European Nicotinamide Diabetes Intervention Trial (ENDIT) Group. European Nicotinamide Diabetes Intervention Trial (ENDIT): a randomised controlled trial of intervention before the onset of type 1. Lancet. 2004;363:925–31.
Diabetes Prevention Trial-Type 1 Diabetes Study Group. Effects of oral insulin in relatives of patients with type 1 diabetes. Diabetes Care. 2005;28:1068–76. This was one of the prevention trials from which the DPTRS was derived.
Diabetes Prevention Trial-Type 1 Diabetes Study Group. Effects of insulin in relatives of patients with type 1 diabetes mellitus. N Engl J Med. 2002;346:1685–91. This was one of the prevention trials from which the DPTRS was derived.
Bottazzo JF, Mann JI, Thorogood M, Baum JD, Doniach D. Autoimmunity in juvenile diabetics and their families. Br Med J. 1978;2(6131):165–8.
Cudworth AG, Woodrow JC. Evidence of HL-A linked genes in “juvenile” diabetes mellitus. Br Med J. 1975;3(5976):133–5.
Vardi P, Crisa L, Jackson RA. Predictive value of intravenous glucose tolerance test insulin secretion less than or greater than the first percentile in islet cell antibody positive relatives of type 1 (insulin-dependent) diabetic patients. Diabetologia. 1991;34:93–102.
Rosenbloom AL, Hunt SS, Rosenbloom EK, Maclaren NK. Ten-year prognosis of impaired glucose tolerance in siblings of patients with insulin-dependent diabetes. Diabetes. 1982;31:385–7.
Ziegler AG, Rewers M, Simell O, Simell T, Lempainen J, Steck A, et al. Seroconversion to multiple islet autoantibodies and risk of progression to diabetes in children. JAMA. 2013;309:2473–9.
Orban T, Sosenko JM, Cuthbertson D, Krischer JP, Skyler JS, Jackson R, et al. Pancreatic islet autoantibodies as predictors of type 1 diabetes in the Diabetes Prevention Trial-Type 1 (DPT-1). Diabetes Care. 2009;32:2269–74.
Sosenko J, Palmer JP, Greenbaum CJ, Mahon J, Cowie C, Krischer JP, et al. Increasing the accuracy of oral glucose tolerance testing and extending its application to individuals with normal glucose tolerance for the prediction of type 1 diabetes. Diabetes Care. 2007;30:38–42.
Sosenko JM, Krischer JP, Palmer JP, Mahon J, Cowie C, Greenbaum CJ, et al. A risk score for type 1 diabetes derived from autoantibody positive participants in The Diabetes Prevention Trial-Type 1. Diabetes Care. 2008;31:528–33. This is the first article to describe the development of the DPTRS.
Sosenko JM, Skyler JS, Mahon J, Krischer JP, Beam CA, Boulware DC, et al. Validation of the Diabetes Prevention Trial-Type 1 Risk Score (DPTRS) in the TrialNet Natural History Study. Diabetes Care. 2011;34:1785–7.
Sosenko JM, Skyler JS, Mahon J, Krischer JP, Greenbaum CJ, Rafkin LE, et al. The use of the Diabetes Prevention Trial-Type 1 Risk Score (DPTRS) for improving the accuracy of the risk classification of type 1 diabetes. Diabetes Care. 2014;37:979–84.
Sosenko JM, Skyler JS, Mahon J, Krischer JP, Beam CA, Boulware DC, et al. The application of the type 1 diabetes risk score for identifying a preclinical state of type 1 diabetes. Diabetes Care. 2012;35:1552–5.
Ilonen J, Hammais A, Laine A, Lempainen J, Vaarala O, Veijola R, et al. Patterns of β-cell autoantibody appearance and genetic associations during the first years of life. Diabetes. 2013;62:3636–40.
Sosenko JM, Skyler JS, Palmer JP, Krischer JP, Yu L, Mahon J, et al. The prediction of type 1 diabetes by multiple autoantibody levels and their incorporation into an autoantibody risk score in relatives of type 1 diabetic patients. Diabetes Care. 2013;36:2615–20.
Acknowledgments
This work was funded by the National Institutes of Health through the National Institute of Diabetes and Digestive and Kidney Diseases, National Institute of Allergy and Infectious Diseases, Eunice Kennedy Shriver National Institute for Child Health and Human Development and National Center for Research Resources; the Juvenile Diabetes Research Foundation International; and the American Diabetes Association. Dr. Jay Sosenko is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
The sponsor of the trial was the Type 1 Diabetes TrialNet Study Group (see Appendix 1). Type 1 Diabetes TrialNet Study Group is a clinical trial network funded by the National Institutes of Health (NIH) through the National Institute of Diabetes and Digestive and Kidney Diseases, the National Institute of Allergy and Infectious Diseases, and The Eunice Kennedy Shriver National Institute of Child Health and Human Development, through the cooperative agreements U01 DK061010, U01 DK061016, U01 DK061034, U01 DK061036, U01 DK061040, U01 DK061041, U01 DK061042, U01 DK061055, U01 DK061058, U01 DK084565, U01 DK085453, U01 DK085461, U01 DK085463, U01 DK085466, U01 DK085499, U01 DK085505, U01 DK085509, and a contract HHSN267200800019C; the National Center for Research Resources, through Clinical Translational Science Awards UL1 RR024131, UL1 RR024139, UL1 RR024153, UL1 RR024975, UL1 RR024982, UL1 RR025744, UL1 RR025761, UL1 RR025780, UL1 RR029890, UL1 RR031986, P30 DK017047, and General Clinical Research Center Award M01 RR00400; the Juvenile Diabetes Research Foundation International (JDRF); and the American Diabetes Association (ADA). The contents of this article are solely the responsibility of the authors and do not necessarily represent the official views of the NIH, JDRF, or ADA.
Compliance with Ethics Guidelines
ᅟ
Conflict of Interest
Jay M. Sosenko, Jay S. Skyler, and Jerry P. Palmer declare that they have no conflict of interest.
Human and Animal Rights and Informed Consent
All procedures performed in the studies involving human participants were in accordance with the ethical standards of the institutional review boards and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Author Contributions
Jay Sosenko contributed by writing the manuscript, Jay Skyler contributed by reviewing the manuscript, and Jerry Palmer contributed by reviewing the manuscript.
This article is part of the Topical Collection on Pathogenesis of Type 1 Diabetes
The Diabetes Type 1 TrialNet and Diabetes Prevention Trial-Type 1 Study Groups (see Appendix 1)
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOCX 41 kb)
Rights and permissions
About this article

Cite this article
Sosenko, J.M., Skyler, J.S., Palmer, J.P. et al. The Development, Validation, and Utility of the Diabetes Prevention Trial-Type 1 Risk Score (DPTRS). Curr Diab Rep 15, 49 (2015). https://doi.org/10.1007/s11892-015-0626-1
Published:
DOI: https://doi.org/10.1007/s11892-015-0626-1