
Abstract
For women with type 1 diabetes (T1DM), type 2 diabetes (T2DM), and gestational diabetes (GDM), poor maternal glycemic control can significantly increase maternal and fetal risk for adverse outcomes. Outpatient medical and nutrition therapy is recommended for all women with diabetes in order to facilitate euglycemia during the antepartum period. Despite intensive outpatient therapy, women with diabetes often require inpatient diabetes management prior to delivery as maternal hyperglycemia can significantly increase neonatal risk of hypoglycemia. Consensus guidelines recommend maternal glucose range of 80–110 mg/dL in labor. The most optimal inpatient strategies for the prevention of hyperglycemia and hypoglycemia proximate to delivery remain unclear and will depend upon factors such as maternal diabetes diagnosis, her baseline insulin resistance, duration and route of delivery etc. Low dose intravenous insulin and dextrose protocols are necessary to achieve optimal predelivery glycemic control for women with T1DM and T2DM. For most with GDM however, euglycemia can be maintained without intravenous insulin. Women treated with a subcutaneous insulin pump during the antepartum period represent a unique challenge to labor and delivery staff. Strategies for self-managed subcutaneous insulin infusion (CSII) use prior to delivery require intensive education and coordination of care with the labor team in order to maintain patient safety. Hospitalization is recommended for most women with diabetes prior to delivery and in the postpartum period despite appropriate outpatient glycemic control. Women with poorly controlled diabetes in any trimester have an increased baseline maternal and fetal risk for adverse outcomes. Common indications for antepartum hospitalization of these women include failed outpatient therapy and/or diabetic ketoacidosis (DKA). Inpatient management of DKA is a significant cause of maternal and fetal morbidity and remains a common indication for hospitalization of the pregnant woman with diabetes. Changes in maternal physiology increase insulin resistance and the risk for DKA. A systematic approach to its management will be reviewed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Good antenatal care, frequent glucose self-monitoring, and medical-nutritional therapy are associated with improved glycemic control and a reduction in the risk of adverse maternal and neonatal outcomes for women with diabetes in pregnancy [1]. Inpatient management of diabetes during pregnancy can present unique challenges for both the patient and her obstetrician. Despite appropriate outpatient antepartum care, maternal hyperglycemia in labor can increase the risk for neonatal hypoglycemia [2–4, 5•]. For women with significant insulin resistance who are poorly controlled and remote from delivery, antepartum hospitalization may be required for optimization of therapy and patient education. DKA is associated with significant maternal/fetal morbidity and mortality. The increasing insulin resistance of pregnancy places women with T1DM and T2DM at significant risk for DKA. Rare cases of DKA for women with GDM have also been reported. This paper will review inpatient management strategies for women with diabetes who require hospitalization for (1) intrapartum and postpartum care, (2) U-500 regular insulin administration due to poor glycemic control, and (3) DKA.
Intrapartum Diabetes Management
The goals of intrapartum management for women with diabetes in pregnancy are to prevent maternal hyperglycemia, minimize the risk of maternal hypoglycemia, and optimize short term neonatal outcome [1]. Despite good antepartum glycemic control, there is a positive correlation between the risk of neonatal hypoglycemia postdelivery and maternal glycemia in labor [4, 6]. Intravenous insulin and dextrose protocols used to maintain euglycemia for the laboring patient are associated with a significant reduction in the risk of neonatal hypoglycemia for women with pregestational and gestational diabetes [6–8].
Fetal Risk and Maternal Intrapartum Glucose Targets
It has been estimated that up to 50 % of infants born to diabetic mothers will experience hypoglycemia after birth [4, 9]. Clinical consequences for the neonate depend upon the severity and duration of hypoglycemia, the underlying etiology, and the need for transfer to the ICU [9]. Neonatal hypoglycemia is more likely to occur for fetuses that are born to diabetic women with poor glycemic control and/or are macrosomic [2–4, 5•]. Infants of poorly controlled diabetic mothers can develop islet cell hyperplasia and baseline hyperinsulinemia in utero during the antepartum period. They are at risk for clinically significant neonatal hypoglycemia when maternal glucose transfer ceases with delivery [2–4, 5•]. The maintenance of euglycemia for diabetic women in labor has been demonstrated to reduce but cannot eliminate neonatal hypoglycemia particularly for those fetuses with diabetic fetopathy in utero due to poor antepartum glycemic control [10].
Predelivery diabetes management is influenced by maternal diabetes diagnosis, baseline insulin sensitivity, the progress of labor, and its duration. Women with T1DM require administration of glucose and insulin during prolonged labor in order to prevent ketosis. Those with GDM and T2DM have insulin requirements that vary depending upon the duration of maternal disease, stage of labor, antepartum glycemic control, and baseline insulin resistance. Insulin requirements for women with GDM may be influenced by gestational age at diagnosis and her risk for overt T2DM. Historically, initial published reports either described the use of an insulin protocol for type 1 diabetics in labor or included a mixed population of women with both GDM and T1 or T2DM [6, 10–14]. Less is known regarding the comparative efficacy of these protocols for each population separately.
Several intravenous insulin/glucose protocols have been published for the maintenance of euglycemia during labor. There are few, if any, randomized controlled trials available as best evidence to support one management approach over the others. A target glucose range of 70–110 mg/dL (3.6–6.1 mmol/L) in labor for both gestational and pregestational diabetics is supported by the American College of Obstetrics and Gynecology (ACOG) and the American College of Endocrinology (ACE) [1, 15]. Several studies suggest that higher levels of maternal glycemia [glucose ≥126 mg/dL (7 mmol/L)] may be safely permitted during labor without increasing neonatal hypoglycemia risk. In a retrospective evaluation of 107 women with T1DM in labor by Taylor et al 46 % of the neonates had persistent hypoglycemia (glucose <45 mg/dL) [7]. The authors did not identify a significant correlation between neonatal hypoglycemia and maternal glucose when it was maintained within a target range of 4.0–8.0 mmol/L (72–144 mg/dL) during labor. They did identify, however, a significant negative correlation between more severe maternal glycemia (glucose >8 mmol/L (144 mg/dL) and neonatal hypoglycemia. These results were confirmed in other studies and suggest that maternal glycemia 15–30 mg/dL above the consensus threshold of 110 mg/dL may be permissible without significantly increasing neonatal risk [16, 17]. These studies further suggest that neonatal hypoglycemia may occur despite euglycemia in labor. The correlation between neonatal hypoglycemia, intrapartum maternal glycemia, and markers of antepartum maternal glycemic control require further study.
The demands of labor necessitate glucose as an energy source. Oral intake during labor is restricted at many institutions due to maternal aspiration risk. Women with T1DM require glucose supplementation in order to keep capillary glucose values within target range and reduce the risk for ketosis. In the latent phase of labor, women with T2DM and GDM may have sufficient glycogen stores to keep capillary glucose >70 mg/dL without supplemental dextrose solutions. Glucose requirements increase, however, with prolonged labor induction, during the active phase of labor, and with maternal pushing [2].
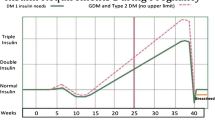
Several excellent glucose/insulin infusion protocols have been published [1, 2, 7, 18, 19•]. Figure 1 depicts elements of the computerized insulin infusion protocol utilized at our institution. This protocol is one of several options available to the practitioner for glycemic control in labor and generates insulin infusion rates that are comparable with those identified in protocols proposed by ACOG and the ADA Technical Reviews and Consensus Recommendations for Care [1, 18].

Screen view of computerized intravenous insulin therapy protocol. If maternal glucose is >110 mg/dL on 2 separate occasions, intravenous insulin is ordered as detailed above. A target glucose range of 80–110 mg/dL is set for all laboring obstetric patients. D5 Normal saline is ordered at 125 cc/h for maintenance fluid if not previously ordered. The computer calculates an insulin drip rate using the following formula: insulin dose (units/hour) = (current glucose (mg/dL) – 60) x multiplier. The multiplier is set at 0.03 but can be d by 0.01 or decreased by 0.01 to 0.02 depending upon subsequent glucose values. An initial glucose value of 115 would trigger an insulin drip rate of 1.7 units/hr. Nurses enter hourly capillary glucose values into a separate “dose titration page” and the computer algorithm will recommend a modification of the drip rate hourly as indicated to keep glucose within target range. The nurse will either accept or speak with the ordering physician to modify the drip rate based upon the patient’s clinical status. The program saves all capillary glucose values and modifications to the insulin drip rate in the electronic medical record
The insulin protocol used for our obstetric population was adopted in 2010 due to its integration with a point of care based electronic order entry system and is a modification of previously published protocols first utilized in critically ill patients at our institution [20–22]. A comparative analysis of maternal and fetal outcomes for pregestational and gestational diabetic women will be necessary in order to determine the benefits and limitations of a computer based intravenous insulin protocol compared with the traditional paper-based intravenous insulin algorithms currently available.
For women with GDM who are diet controlled during the antepartum period, delivery can occur without the need for intravenous insulin. Up to 65 % of women with GDM who have a fasting glucose ≤ 95 mg/dL at diagnosis can achieve optimal antepartum glycemic control with nutrition alone and as such are at low risk for hyperglycemia in labor [19•, 23]. Flores-Le Roux performed a prospective observational study of 129 women with GDM in labor. Eighty-six percent of study participants had capillary glucose values within target range for their institution (3.3 compared with 7.2 mmol/L) or (59.6 compared with 129.6 mg/dL) and did not require insulin [19•]. A maternal glucose target of 7.2 mmol/L (129.6 mg/dL) was selected as the upper limit of normal for this population based upon prior studies that failed to identify neonatal hypoglycemia below this threshold [7, 17, 24, 25]. Maintaining euglycemia in labor for women with GDM may also be possible without insulin by rotating dextrose and nondextrose containing solutions [16, 26]. Additional research is needed for women with GDM in order to identify an evidence based protocol that will facilitate maternal glycemic control, limit insulin use when not indicated, and reduce the risk of neonatal hypoglycemia.
Patients with diabetes in labor who require intravenous insulin are at risk for hypoglycemia if glucose administration is insufficient for maternal demand. Prompt recognition and management of hypoglycemia are important in order to minimize provider error and maternal/fetal risk. Baseline serum glucose levels are 20 % lower in pregnancy compared with the nonpregnant state and as such, women with diabetes are at significant risk for symptomatic and asymptomatic hypoglycemia [27]. The management of hypoglycemia in pregnancy is complicated by lack of consensus regarding its definition. The ADA and The Endocrine Society define hypoglycemia as plasma glucose less than 70 mg/dL [28••]. In pregnancy, ACOG and others report fasting glucose of 60 mg/dL to be the lower end of normal range, with mild hypoglycemia defined as a glucose <60 mg/dL [1, 23, 27, 29, 30]. An example of the hypoglycemia protocol on our obstetrics unit is described in Table 1.
Cesarean Delivery
Women with insulin requiring pregestational diabetes are encouraged to take a reduced dose of intermediate/long acting insulin the evening prior to delivery if the cesarean will start early the next day. For women with GDM, insulin dosing the night prior to delivery will depend upon baseline maternal insulin resistance and her antepartum medication requirements. The day of surgery, the patient should have nothing by mouth and surgery is best scheduled early in the day in order to prevent prolonged fasting related hypoglycemia [29].
For all diabetic women, a capillary glucose is tested at hospital admission and hourly thereafter. They are hydrated with nondextrose containing solution if glucose is 70–110 mg/dL, given dextrose only if glucose <70 mg/dL, and is given insulin/dextrose infusion if glucose >110 mg/dL twice in a row.
With epidural or spinal anesthesia placement, nondextrose containing crystalloid is bolused in order to prevent maternal hypotension and maintain uteroplacental perfusion. Whenever possible, glucose supplementation should be given separately with a smaller volume of IV fluid in order to minimize administration error. At our institution, the bag and tubing for all insulin and dextrose containing solutions are clearly labeled in order to minimize medication and communication errors between anesthesia and nursing staff. Once target capillary glucose is reached, the intravenous insulin is disconnected prior to operating room (OR) transfer in order to minimize fluid administration errors during anesthesia. In the OR, capillary glucose is checked hourly, and dextrose alone or dextrose/insulin may be indicated depending upon maternal glucose and procedure duration. If the intravenous insulin is restarted in the OR due to delay in delivery, the patient is at risk for hypoglycemia and should be followed closely once the placenta is delivered.
Intrapartum Management of Patients Using a Self-Managed Continuous Subcutaneous Insulin Infusion (CSII)
Women with pregestational diabetes who are managed during the antepartum period with CSII, present a unique challenge prior to delivery [29, 32]. Options for diabetes management intrapartum include discontinuation of the CSII and initiation of intravenous insulin, or continued use of the CSII [29, 31, 32]. In the absence of endocrine or inpatient diabetes management team consultation, discontinuation of the device may be preferred. For patient safety, we encourage the development of institution and unit specific protocols for CSII use with labor. At our institution, the CSII is discontinued once glucose values are outside of the target range (70–110 mg/dL) and the patient is given intravenous insulin per protocol. Continued use of the CSII intrapartum would necessitate frequent evaluation of pump basal insulin rates and carbohydrate bolus settings as the patient progresses through delivery and enters the postpartum period. Coordinated care of the patient necessitates communication between obstetrics, nursing staff, and the endocrine inpatient diabetes management service as indicated, in order to minimize the risk of glucose excursions above or below target range prior to delivery. If CSII continuation is planned, the patient’s prelabor basal rate may need to be reduced by 50 % or more during the active phase of labor and in the postpartum period [29]. Situations impairing patient cognition, such as the administration of pain medication, anesthesia, etc should necessitate transition from CSII therapy to alternative management, which is not patient dependent. Several excellent references regarding hospital protocols for CSII use are available for review [33–36].
Postpartum
The insulin resistance of pregnancy ends abruptly with delivery of the placenta. Maternal insulin requirements decrease by one-third to one-half [1, 29]. Postpartum fasting and postmeal glycemic parameters are less stringent compared with those expected of pregnancy. In noncritically ill hospitalized patients, the ADA considers a fasting glucose of <140 mg/dL and a random glucose of <180 mg/dL acceptable. It is acknowledged however, that lower glucose values are permissible for those with a history of tighter glucose control prior to hospital admission [37]. The target glucose values, which would best facilitate cesarean section wound healing, have not been well studied and remain unclear. We recommend a fasting glucose of <110 g/dL and post meal glucose values of ≤ 160 mg/dL particularly for women with delivery by cesarean, these recommendations are consistent with those previously published (fasting <100 mg/dL, postmeal <150 mg/dL) [38].
For women who are in the immediate postoperative state, carbohydrate intake during the first 12–24 hours may be difficult to anticipate. The administration of short acting insulin by sliding scale can provide coverage as necessary with meals until a solid diet can be tolerated [29, 38]. Women with T1DM and T2DM may a resume short/long acting insulin regimen at half the predelivery doses. Continuation of long-acting basal insulin is extremely important in women with T1DM, in order to prevent the risk of DKA. Women using a CSII may restart with reduction of predelivery basal rates by half. Predelivery carbohydrate ratios may be decreased by half to a third.
Depending upon baseline insulin sensitivity, a percentage of women with T2DM may not require medication therapy in the immediate postpartum period. Both metformin and glyburide are safe with breastfeeding [38]. However, these oral medications should be utilized only if necessary in the setting of documented hyperglycemia. Lifestyle modification to promote weight loss and subsequent improvement in insulin sensitivity should be recommended to all that need it and may reduce the requirement for oral hypoglycemic agents postpartum. Upon discharge to home, we recommend women with pregestational diabetes continue capillary glucose testing pre and postmeals until insulin requirements have been established. Prompt follow-up with an endocrinologist or internist, in order to optimize insulin dosing and further simplify glucose testing frequency is encouraged. According to the ADA, the optimal testing frequency for women with T2DM on oral agents is unclear [39••]. We recommend continued daily fasting glucose testing for women on oral agents until there is outpatient follow-up.
Most women with GDM will no longer have glucose intolerance after delivery of the placenta. It is estimated however, that women with GDM have up to a 50 % risk of developing type 2 DM over time [23]. Further, a small percentage of women with GDM in the index pregnancy are at risk of overt T2DM or impaired glucose tolerance undiagnosed prior to pregnancy. Those with GDM who are most at risk for postpartum hyperglycemia and T2DM are women with: morbid obesity, a first or second trimester diagnosis of GDM during the index pregnancy, a significant insulin requirement prior to delivery (100–150 units/day), and prior history of GDM with no formal testing postpartum [38]. Diagnostic testing for T2DM is recommended per ADA guidelines in the outpatient setting by 6 weeks postpartum after the effects of pregnancy have resolved [23, 39••].
U-500
For women with pregestational diabetes, baseline insulin requirements can increase by up to 3-fold in the third trimester [40]. Women taking 75–100 units/day of insulin or more prior to pregnancy may require an escalation of insulin dosing and more frequent insulin administration during the second and third trimesters. A frequent dosing regimen with large volumes of insulin may diminish insulin efficacy due to poor absorption, increase the risk of noncompliance, increase medication costs, and result in poor glycemic control. Subspecialists are often asked to comment upon the benefits and risks of concentrated U-500 regular insulin compared with standard U-100 insulin, for women who fail standard therapy. While several case reports have been published describing successful use of U-500 in pregnancy, we would caution against widespread adoption of this medication in the absence of evidence-based recommendations to support patient selection, efficacy, and safety in pregnancy. A brief review of U-500 and its use in pregnancy are detailed below.
U-500 regular insulin (U-500) has been used in patients with significant insulin resistance. Patient compliance with previously prescribed U-100 should be confirmed and U-500 therapy should be considered only if the patient is unable to maintain euglycemia, despite U-100 treatment. It is associated with fatal medication errors as reported to the FDA and is a “high alert medication” by the Institute for Safe Medication Practice due to patient risk should a dosing error occur [41, 42]. U-500 contains 500 units insulin/ml and is 5-fold more concentrated than the U-100 insulin commonly used in pregnancy. The higher concentration is potentially advantageous in that it can be administered in a volume that is 80 % less than expected with an equivalent dose of U-100 insulin [43•]. The concentration of U-500 is associated with a prolonged absorption time and a pharmacokinetic profile that is more similar to NPH than to Regular insulin. U-500 insulin has a 30 minutes onset of action, time to peak effect of 2–4 hours, and duration of action of 10–24 hours [41]. U-100 regular insulin, in comparison, has a duration of action of 4–6 hours.
U-500 insulin has been well studied in the nonpregnant population, however, little is known, regarding its efficacy and safety in pregnancy [41, 43•, 44, 45]. Despite recent case reports, caution against widespread use of U-500 in pregnancy is recommended due to safety concerns and the risk of hypoglycemia [46–48]. If the decision is made to initiate U-500, appropriate education for the patient, her family, and any hospital staff involved with drug administration is important. We do recommend intravenous infusion with U-100 regular insulin protocols while in labor and immediately prior to cesarean in order to minimize errors. Hospitals are encouraged to develop institution specific protocols in order to ensure appropriate medication labeling, storage, and administration. The reader is referred to several excellent references with protocols designed to address U-500 safety concerns in hospitalized patients [43•, 49–51].
Currently there are no consensus guidelines regarding ideal patient selection for U-500, several authors suggest that it may be considered if the patient requires ≥200–300 units of U-100 insulin per day. For medication initiation, the current total daily dose of insulin is calculated, and divided into 2–3 doses throughout the day [41, 43•, 52]. The actual U-500 dose and volume administered can be calculated by dividing the total U100 dose for each injection by 5.
Keeping this in mind, if the patient receives 100 units of U-100 insulin 3 times daily, this would be equivalent to a U-500 dose of 20 units, which is a volume of 0.2 ml on a tuberculin syringe or equivalent to 20 unit “marking” on a U-100 insulin syringe. Clearly patient education and nursing education regarding the exact volume of U-500 to be administered is needed in order to prevent inadvertent dosing errors. U-500 insulin is not widely available in all pharmacies and is dispensed in insulin vials, which are shaped differently from U100 insulin. Careful patient selection, a discussion with the patient regarding the limited data supporting the use of this insulin in pregnancy, and close follow-up after insulin initiation are recommended if U-500 is determined to be the best alternative to U-100 during the antepartum period.
Diabetic Ketoacidosis
Diabetic ketoacidosis (DKA) has an incidence of 2 %–3 % and remains a leading cause of maternal morbidity and fetal mortality [53–56].
DKA develops as a result of relative insulin deficiency, inadequate glucose utilization at the cellular level, and the exaggerated counter regulatory response that occurs as a result [57–61].
Pregnancy does not alter the basic pathophysiology of DKA. Hormones and hormone levels unique to pregnancy can, however, predispose diabetic women to ketosis, diminish insulin sensitivity, and enhance the counter-regulatory response to relative insulin deficiency. During pregnancy there is increased production of human placental lactogen, cortisol, prolactin, and estrogen. These hormones promote insulin resistance and the production of free fatty acid/amino acid substrates, which can be used as an alternate energy source by the mother, fetus, and placenta. Baseline maternal insulin production is increased in pregnancy compared with the nonpregnant state and is characterized by insulin secretion that is 1.5- to 2-fold higher in early pregnancy, and 3-fold higher in late pregnancy compared with nonpregnant controls [40]. For women with diabetes, the degree of insulin resistance in pregnancy is such that there is decreased utilization of glucose at the cellular level and relative hyperglycemia occurs as a result [62].
DKA classically presents in pregestational diabetics with moderate-to-severe hyperglycemia. In pregnancy however, DKA can present with less hyperglycemia (glucose ≤200 mg/dL) due to greater baseline propensity to ketogenesis and lower serum bicarbonate concentration [54, 63, 64]. Rare cases of normoglycemic DKA in women with pregestational and gestational diabetes have also been reported [59, 63, 65]. Cullen et al identified a cohort of 11 pregnant diabetic women with DKA from 1985–1995 [53]. Thirty–six percent had a blood glucose of 130–200 mg/dL at initial presentation. Chico et al reported their experience in a woman with euglycemic T1DM (glucose 87 mg/dL) with starvation ketoacidosis due to prolonged delay in insulin administration with labor induction [65]. Many of the gestational diabetics with DKA identified in case series are obese, have risk factors for overt T2DM, or have unique stressors related to pregnancy as the precipitating event [59, 63, 64, 66].
Infection, while significant, may not be the most common precipitating factor for DKA in pregnancy. Montoro et al presented a case series, in which noncompliance or cessation of insulin therapy during pregnancy was determined to be either a primary or contributing factor in 40 % of women. Infection and undiagnosed diabetes were identified as the etiology in 20 % and 30 % of women admitted with DKA, respectively [54]. A retrospective review of 64 women with DKA in pregnancy by Rodgers and Rodgers identified refractory emesis and use of beta-sympathomimetics for tocolysis as the most common precipitating factors [56]. Other common precipitating factors reported include use of corticosteroids for fetal lung maturity, poor management of hyperglycemia, and insulin pump failure [1, 62, 67, 68].
Diabetic Ketoacidosis: Presentation, Diagnosis, and Management
The presenting signs, symptoms, laboratory studies, and recommended management principles for DKA are summarized in Table 2. Duration of therapy is individualized to the patient and has the following aims:
-
(1)
Aggressive hydration to correct the volume deficit, improve circulatory volume, and improve uterine perfusion
-
(2)
Insulin therapy
-
(3)
Correction of electrolyte abnormalities
-
(4)
Identification and treatment of precipitating cause
-
(5)
Assess fetus response to therapy.
The reader is referred to several excellent references for detailed inpatient management algorithm options [1, 58, 61, 62].
Fetal response to DKA
Our understanding of the fetal response to maternal metabolic acidosis is limited to that obtained from changes in the fetal heart rate observed during maternal therapy and animal models of acidosis [55, 58, 61, 62]. Maternal insulin does not cross the placenta. Fetal pancreatic beta cells produce insulin in response to hyperglycemia after 20 weeks gestation. Throughout pregnancy, however, maternal glucose, free fatty acids, and ketones cross the placenta freely and increase fetal risk for hyperglycemia and acidemia. The fetal response to maternal DKA is unknown but is likely influenced by fetal maturity, the severity and duration of maternal acidosis, and uteroplacental blood flow.
Delivery due to transient changes in the fetal heart rate during initial management of the mother is not indicated as fetal status is expected to improve with maternal therapy [58, 69]. Fetal monitoring during the acute phase of maternal resuscitation should only be undertaken if the information obtained will be useful with regard to optimizing maternal management. At our institution, we do not perform prolonged fetal heart rate monitoring until maternal stability for an operative delivery is assured. The use of corticosteroids for fetal lung maturity may be considered in women with DKA only if they remain at high risk for preterm delivery after resolution of the maternal metabolic derangement.
Conclusions
Hospitalization of pregnant women with diabetes is indicated in order to reduce maternal and fetal risk for adverse outcomes. Intravenous insulin and dextrose protocols may be employed to keep maternal glucose within target range prior to delivery. Further research is necessary to determine if the maternal glucose threshold can be expanded to include more moderate degrees of hyperglycemia without increasing maternal and/or fetal risk. Use of a subcutaneous insulin pump and U-500 insulin require patient and staff education in order to deliver consistent patient care and maintain patient safety. DKA remains a significant cause of morbidity and mortality. The incidence of DKA is increased in pregnancy due to changes in maternal physiology. The treatment of DKA in pregnancy is similar to that offered for all adults with DKA. Prompt recognition of disease, maternal hydration, and prompt insulin therapy are necessary in order to reduce maternal and fetal risk. Excellent teamwork and education of all team members in the various nuances of management of the pregnant hospitalized patient, translates into the best outcomes for mother and baby.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
ACOG Committee on Practice Bulletins. ACOG Practice Bulletin. Clinical management guidelines for obstetrician-gynecologists. Number 60, March 2005. Pregestational Diabetes Mellitus. Obstet Gynecol. 2005;105:675.
Jovanovic L. Glucose and insulin requirements during labor and delivery: the case for normoglycemia in pregnancies complicated by diabetes. Endocr Pract. 2004;10(Suppl):40–5.
Mimouni F, Miodovnik M, Siddiqi TA, Khoury J, Tsang RC. Perinatal asphyxia in infants of insulin-dependent diabetic mothers. J Pediatr. 1988;113(2):345
Nold JL, Georgieff MK. Infants of diabetic mothers. Pediatr Clin N Am. 2004;51:619–37.
Hawdon JM. Babies born after diabetes in pregnancy: what are the short- and long-term risks and how can we minimize them? Best Prac Res Clin Obstet Gynecol. 2011;25:91–104. This review characterizes the short-term and long-terms risks for infants born to women with diabetes and identifies those that may potentially be avoided with good antenatal or intrapartum care.
Andersen O, Hertel L, Schmolker L, et al. Influence of the maternal plasma glucose concentration at delivery on the risk of hypoglycemia in infants of insulin-dependent diabetic mothers. Acta Paediatr Scand. 1985;74:268–73.
Taylor R, Lee C, Kyne-Grzebalski D, Marshall SM, et al. Clinical outcomes of pregnancy in women with type 1 diabetes. Obstet Gynecol. 2002;99:537–41.
Balsells M, Corcoy R, Adelantado JM, et al. Gestational diabetes mellitus: metabolic control during labor. Diabetes Nutr Metab. 2000;13:257–62.
Cordero L, Treuer SH, Landon MB, et al. Management of infants of diabetic mothers. Arch Pediatr Adolesc Med. 1998;152(3):249–54.
Kline GA, Edwards A. Antepartum and intra-partum insulin management of type 1 and type 2 diabetic women: impact on clinically significant neonatal hypoglycemia. Diabetes Res Clin Pract. 2007;77:223–30.
Miodovnik M, Mimouni F, Tsang R, et al. Management of the insulin dependent diabetic during labor and delivery: influences on neonatal outcome. Am J Perinatol. 1987;4:106–14.
West TE, Lowry C. Control of blood glucose during labor in diabetic women with combined glucose and low dose insulin infusion. Br Med J. 1977;1:1252–4.
Caplan RH, Pagliara AS, Beguin EA, et al. Constant intravenous insulin infusion during labor and delivery in diabetes mellitus. Diabetes Care. 1982;5:6–10.
Feldberg D, Dicker D, Samuel N, et al. Intrapartum management of insulin dependent diabetes mellitus gestatants. A comparative study of constant intravenous insulin infusion and continuous subcutaneous insulin infusion pump. Acta Obstet Gynecol Scand. 1988;67:333–8.
Garber AJ, Moghissi ES, Bransome Jr ED, et al. American College of Endocrinology position statement on inpatient diabetes and metabolic control. Endocr Pract. 2004;10 Suppl 2:4–9.
Barrett HL, Morris J, McElDuff A. Watchful waiting: a management protocol for maternal glycaemia in the peri-partum period. Aust N Z Obstet Gynecol. 2009;49:162–7.
Carron Brown S, Kyne-Grzebalski D, Mwangi B, et al. Effect of management policy upon 120 Type 1 diabetic pregnancies: policy decisions in practice. Diabetes Med. 1999;16:573–8.
Conway DL, Catalano PM, et al. In: Kitzmiller JL, Jovanovic L, Brown F, editors. Management of delivery. In: managing Pre-existing diabetes and pregnancy. Technical reviews and consensus recommendations for care. Alexandria: American Diabetes Association; 2008. p. 584.
Flores-Le roux JA, Chillaron JJ, Goday A, et al. Peripartum control in gestational diabetes. Am J Obstet Gynecol. 2010;202(568):e1–6. The results of this prospective observation study determined that only 31 % of women with GDM required insulin during labor. For women with GDM and intrapartum glucose values within target range, the risk of neonatal hypoglycemia was significantly associated with antepartum A1C and limited prenatal care.
Bode BW, Braithwaite SS, Steed RD, Davidson PC. Intravenous insulin infusion therapy: indications, methods, and transition to subcutaneous insulin therapy. Endocr Prac. 2004;10 Suppl 2:71–80.
White NH, Skor D, Santiago JV. Practical closed-loop insulin delivery. A system for the maintenance of overnight euglycemia and the calculation of basal insulin requirements in insulin-dependent diabetics. Ann Intern Med. 1982;97:210–3.
Boord JB, Sharifi M, Greevy RA, et al. Computer-based insulin infusion protocol improves glycemia control over manual protocol. J Am Med Inform Assoc. 2007;14:278–87.
ACOG Practice Bulletin. Clinical management guidelines for obstetrician-gynecologists. Number 30, September 2001 (replaces Technical Bulletin Number 200, December 1994). Gestational diabetes. Obstet Gynecol. 2001;98:525–38.
Lean ME, Pearson DW, Sutherland HW. Insulin management during labor and delivery in mothers with diabetes. Diabetes Med. 1990;7:162–4.
Njenga E, Lind T, Taylor R. Five year audit of peri-partum blood glucose control in type 1 diabetic patients. Diabetes Med. 1992;9:567–70.
Rosenberg VA, Eglinton GS, Rauch ER, et al. Intrapartum maternal glycemic control in women with insulin requiring diabetes: a randomized clinical trial of rotating fluids versus insulin drip. Am J Obstet Gynecol. 2006;195:1095–9.
Rosenn BM, Miodovnik M. Glycemic control in the diabetic pregnancy: is tighter control always better? J Mat Fetal Med. 2000;9:29–34.
Seaquist ER, Anderson J, Childs B, et al. Hypoglycemia and diabetes: a report of a workgroup of the American Diabetes Association and the Endocrine Society. J Clin Endocrinol Metab. 2013;98:1845–59. This report confirms working definition of hypoglycemia, describes implications of hypoglycemia on treatment outcomes, and presents strategies for prevention.
Gabbe SG, Carpneter LB, Garrison EA. New strategies for glucose control in patients with Type 1 and Type 2 Diabetes Mellitus in pregnancy. Clin Obstet Gynecol. 2007;50:1014–24.
Mazze R, Yogev Y, Langer O. Measuring glucose exposure and variability using continuous glucose monitoring in normal and abnormal glucose metabolism in pregnancy. J Matern Fetal Neonatal Med. 2012;7:1171–5.
Fresa R, Visalli N, Di Bassi V, et al. Experiences of continuous subcutaneous insulin infusion in pregnant women with Type 1 Diabetes during delivery from four Italian Centers: a retrospective observational study. Diabetes Tech Ther. 2013;15:328–34.
Gabbe SG. New concepts and applications in the use of the insulin pump during pregnancy. J Matern Fetal Med. 2000;9:42–5.
McCrea D. Management of the hospitalized diabetes patient with an insulin pump. Crit Care Nur Clin N Am. 2013;25:111–21.
Leonhardi BJ, Boyle ME, Beer KA, et al. Use of continuous subcutaneous insulin infusion (insulin pump) therapy in the hospital: a review of one institution’s experience. J Diabetes Sci Technol. 2008;2:948–62.
Nassar AA, Partlow BJ, Boyle ME, et al. Outpatient-to-inpatient transition of insulin pump therapy: successes and continuing challenges. J Diabetes Sci Tech. 2010;4:863–72.
Cook CB, Boyle ME, Cisar NS, et al. Proposed guidelines and outcome measures use of continuous subcutaneous insulin infusion (insulin pump) therapy in the hospital setting : proposed guidelines and outcomes measures. Diabetes Educ. 2005;31:849–57.
The American College of Endocrinology Task Force on Inpatient Diabetes Metabolic Control. American College of Endocrinology position statement on inpatient metabolic control. Endocr Prac. 2004;10:77–82.
Kjos SL. After pregnancy complicated by diabetes: postpartum care and education. Obstet Gynecol Clin N Am. 2007;34:335–49.
American Diabetes Association. Standards of medical care in diabetes—2013. Diabetes Care. 2013;36 Suppl 1:S11–66. Provides evidence based consensus recommendations for the diagnosis, screening, and management of diabetes in adults and in special populations including GDM.
Catalano PM, Tyzbir ED, Roman NM, et al. Longitudinal changes in insulin release and insulin resistance in non-obese pregnant women. Am J Obstet Gynecol. 2007;50:938–48.
Quinn SL, Lansang MC, Mina D. Safety and effectiveness of U-500 insulin therapy in patients with insulin resistant type 2 diabetes mellitus. Pharmacotherapy. 2011;31:695–702.
U.S. Food and Drug Administration. Potential signals of serious risks/new safety information identified from the adverse event reporting system (AERS) between January– March, 2008. Available from http://www.fda.gov/Drugs/GuidanceCompliance RegulatoryInformation/ Surveillance/ Adverse Drug Effects/ ucm08 5914.htm. Accessed October 6, 2008.
Reutrakal S, Wroblewski K, Brown RL. Clinical use of U-500 regular insulin: review and meta- analysis. J Diabetes Sci Tech. 2012;6(2):412–20. This meta-analysis of characterizes the efficacy and risks reported with U-500 use in 365 adults with Type 1 and Type 2 diabetes complicated by severe insulin resistance.
De la Pena A, Riddle M, Morrow LA, et al. Pharmacokinetics and pharmacodynamics of high dose regular human insulin in healthy obese subjects. Diabetes Care. 2011;34:2496–2501.
Daily AM, Williams S, Tajeha D, Tannock LR. Clinical evidence with U-500 insulin use. Diabetes Res Clin Pract. 2010;88:259–64.
Zuckerwise LC, Werner EF, Pettker CM, et al. Pregestational diabetes with extreme insulin resistance. Use of U-500 in pregnancy. Obstet Gynecol. 2012;12:439–42.
Okeigwe I, Yeaton-Massey A, Kim S, et al. U-500R and aspart insulin for the treatment of severe insulin resistance associated with pregestational diabetes. J Perinatol. 2013;33:235–8.
Reece EA. Use of U-500 Insulin in pregnancy is intriguing, but controlled trials are needed. Obstet Gynecol. 2012;120(Part 2):435–6.
Samaan KH, Dahlke M, Stover J. Addressing safety concerns about u-500 insulin in a hospital setting. Am J Health Syst Pharm. 2011;68:63–8.
Garg R, Johsn V, McNally PG, et al. U-500 Insulin: why, when, how to use in clinical practice. Diabetes Metab Res Rev. 2007;23:265–8.
Segal AR, Brunner JE, Burch FT. Use of concentrated insulin human regular (U-500) for patients with diabetes. Am J Health Syst Pharm. 2010;67:1526–35.
Shubrook JH. Insulin therapy for challening patient cases. J Am Osteopath. 2013;113(4 Suppl 2):217–28.
Cullen MT, Reece EA, Homko CJ, et al. The changing presentations of diabetic ketoacidosis during pregnancy. Am J Perinatol. 1996;13(7):449–52.
Montoro MN, Meyer VP, Mestman JH, et al. Outcome of pregnancy in diabetic ketoacidosis. Am J Perinatol. 1993;10:17–20.
Hagay ZJ. Diabetic ketoacidosis in pregnancy: etiology, pathophysiology, and management. Clin Obstet Gynecol. 1994;37:50–68.
Rogers BD, Rogers DE. Clinical variables associated with diabetic ketoacidosis during pregnancy. J Reprod Med. 1991;36:797–9.
Ramin KD. Diabetic ketoacidosis in pregnancy. Obstet Gynecol Clin N Am. 1999;26:481–8.
Carroll MA, Yeomans ER. Diabetic ketoacidosis in pregnancy. Crit Care Med. 2005;33:S347–53.
Schenider MB, Umiperrez GE, Ramsey RD, et al. Pregnancy complicated by diabetic ketoacidosis. Diabetes Care. 2003;26:958–9.
Kitabachi AE, Umiperrez GE, Murphy MB, et al. Management of hyperglycemic crises in patients with diabetes. Diabetes Care. 2001;24:131–53.
Umiperrez GE, Muphy MB, Kitabchi AE, et al. Diabetic ketoacidosis and hyperglycemic hyperosmolar syndrome. Diabetes Spectr. 2002;15:28–36.
Parker JA, Conwat DL. Diabetic ketoacidosis in pregnancy. Obstet Gynecol Clin N Am. 2007;34:533–43.
Clark JD, McConnell A, Hartog M. Normoglycemic ketoacidosis in a woman with gestational diabetes. Diabetes Med. 1991;8:388–9.
Franke B, Carr D, Hatem MH. A case of euglycemic diabetic ketoacidosis in pregnancy. Diabetes Med. 2001;18:858–9.
Chico M, Levine SN, Lewis DF. Normoglycemic diabetic ketoacidosis in pregnancy. J Perinatol. 2008;28:310–2.
Kilvert JA, Nicholson HO, Wright AD. Ketoacidosis in diabetic pregnancy. Diabetes Med. 1993;10:278–81.
Kamalakannan D, Baskar V, Barton DM, et al. Diabetic ketoacidosis in pregnancy. Postgrad Med J. 2003;79:454–7.
Lindenbaum C, Menzin A, Ludmir J. Diabetic ketoacidosis in pregnancy resulting from insulin pump failure. A case report. L Reprod Med. 1993;38:306–8.
Chauhan SP, Perry KG, McLaughlin BN, et al. Diabetic ketoacidosis complicating pregnancy. J Perinatol. 1996;16:173–5.
Compliance with Ethics Guidelines
ᅟ
Conflict of Interest
Etoi A. Garrison declares that he has no conflict of interest. Shubhada Jagasia declares that he has no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Hospital Management of Diabetes
Rights and permissions
About this article
Cite this article
Garrison, E.A., Jagasia, S. Inpatient Management of Women with Gestational and Pregestational Diabetes in Pregnancy. Curr Diab Rep 14, 457 (2014). https://doi.org/10.1007/s11892-013-0457-x
Published:
DOI: https://doi.org/10.1007/s11892-013-0457-x