
Abstract
Red yeast rice (RYR) is a Chinese herbal supplement produced by fermenting white rice with the yeast, Monascus purpureus. The Chinese have used RYR to flavor, color, and preserve foods and as a traditional medicine for many years. In the USA, RYR has been used as an alternative to statin therapy in treating patients with mild to moderate hypercholesterolemia. RYR contains a variety of monacolins, which inhibit hydroxymethylglutaryl-coenzyme A (HMG CoA) reductase, the rate-limiting step in cholesterol synthesis. Consumption of RYR has increased recently especially among patients who might be intolerant to standardized therapy due to statin-associated myalgia (SAM). Several clinical trials have shown RYR to be safe, effective, and well tolerated; however, the studies are small and of short duration. The US Food and Drug Administration has prohibited the sale of all RYR products containing monacolin K, which is chemically identical to lovastatin, because it is considered an unapproved drug. However, many RYR supplements continue to remain on the market and lack standardization and quality control.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction and Background
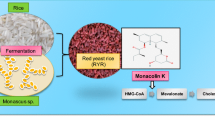
Red yeast rice (RYR), also known as Hong Qu, is a Chinese herbal supplement first described in the Tang Dynasty in 800 AD [1]. It is made by fermenting white rice with the yeast, Monascus purpureus, which turns the rice a red color [2]. The Chinese use RYR as a food preservative, a flavor enhancer, and a food-coloring agent for fish sauce, rice wine, red soybean curd, pickled vegetables, and salted meats. It has also been used in Chinese folk medicine for treating indigestion and diarrhea [2, 3]. In the USA, RYR has been used as an alternative to statin therapy especially among patients opposed to taking statins or who might be intolerant to standardized therapy due to statin-associated myalgia (SAM) [4]. Available as an over-the-counter supplement, several studies have shown RYR to be safe and effective in treating patients with mild to moderate hypercholesterolemia [1]. Consumption of RYR has risen dramatically by almost 80 % in the USA from 2005 to 2008 [1, 4].
Proposed Mechanism of Action
Red yeast rice contains varying amounts of monacolins, a family of naturally occurring substances that inhibit hydroxymethylglutaryl-coenzyme A (HMG CoA) reductase, the rate-limiting step in cholesterol synthesis. One such monacolin, monacolin K, is chemically identical to lovastatin (Fig. 1) [1, 3]. Approximately 90 % of the total monacolin content of RYR consists of monacolin K and its hydroxy acid form, monacolin KA [3, 5, 6]. Other active ingredients with the potential to lower cholesterol in commercially available RYR products include plant sterols (beta-sitosterol, campesterol, stigmasterol), isoflavones, and monounsaturated fatty acids [3].

Chemical structures of monacolin K (lovastatin) and citrinin [1]
In various populations, RYR has been shown to reduce low-density lipoprotein cholesterol (LDL-C) by 22 to 30 % [1]. A greater reduction was observed in one trial when a more potent RYR product with a higher monacolin K content was combined with fish oil and lifestyle changes [7]. Clinical trials have found that a relatively small dose of RYR (equivalent to a daily lovastatin dose of 5 to 7 mg) is as effective as 20 to 40 mg of pure lovastatin in lowering cholesterol [1, 8, 9]. Little is known about the pharmacodynamics of the other monacolins contained in RYR, but it has been suggested that they may also have lipid-lowering effects or potentiate the effects of monacolin K [10]. A recent study demonstrated that the oral bioavailability and dissolution rate of lovastatin is enhanced when given as RYR, which may improve its efficacy [11].
Clinical Trial Evidence
Lipid-lowering Effects
Several clinical trials have proven RYR’s efficacy in treating mild to moderate hypercholesterolemia (Table 1) [1]. The total amount of RYR per day in the various trials ranged from 1200 to 4800 mg, generally divided into two doses [5]. The first prospective, double-blind, placebo-controlled study evaluating RYR in an American population was conducted by Heber et al. in 1999 [8]. Eighty-three healthy adults with untreated hyperlipidemia were randomly assigned to receive 2.4 g per day of RYR (Cholestin, Pharmanex, Inc, Simi Valley, CA) or placebo for 12 weeks. Both groups were counseled on an American Heart Association cardioprotective diet, which contained less than 10 % of calories from saturated fat and less than 300 mg from cholesterol per day. At week 12, LDL-C levels were significantly different (P < 0.001) between the two groups. Compared to baseline, LDL-C levels decreased by 39 ± 19 mg/dL (22 %) in the RYR-treated group and by 5 ± 22 mg/dL (5 %) in the placebo group. There were no reported adverse events in either group [8]. Other studies have shown similar results in different populations [12, 13]. However, all these studies have several limitations, including small sample size, short duration, and single-site design.
Becker et al. compared the efficacy of an “alternative treatment” which included RYR (Res-Q LDL-X, N3 Oceanic, Palm, PA), fish oil, and therapeutic lifestyle changes with simvastatin 40 mg per day in 74 primary prevention patients with known or newly diagnosed hypercholesterolemia [7]. Each 600 mg RYR capsule contained 2.53 mg of monacolin K (lovastatin). Depending on baseline LDL-C, patients were given 1200 mg RYR (10 mg lovastatin) or 1800 mg (15 mg lovastatin) twice daily for a period of 12 weeks. All patients in the alternative treatment group (ATG) received six fish oil capsules.
At the conclusion of the study, both groups had a similar reduction in LDL-C which was statistically significant (P < 0.001 for both), and no significant differences were found between the two groups. LDL-C levels were reduced by 42 ± 15 % in the ATG and 40 ± 20 % in the simvastatin group. Participants in the ATG, however, lost more weight during the study (−4.7 ± 2.4 kg vs −0.3 ± 2.2 kg) and had a significant reduction in triglycerides compared with the simvastatin group. The authors concluded that both the weight loss and addition of fish oils likely contributed to the lower triglyceride levels in the ATG [7].
A recently published multicenter trial [14••] was done testing the efficacy of a partially purified extract of RYR, Xuezhikang (XZK), in lowering non-high-density lipoprotein cholesterol (non-HDL-C) and LDL-C in patients with dyslipidemia. Patients were randomized to a placebo or one of two different doses of XZK, 1200 mg containing 12 mg of lovastatin or double the dose for 4 to 12 weeks. The trial was conducted at 15 sites between the USA and China with a total of 116 participants. Treatment with XZK was well tolerated and resulted in significant reductions in both non-HDL-C (24 %) and LDL-C (27 %) compared with placebo (P < 0.001 for both). Doubling the dose at week eight resulted in an additional 4.6 % reduction in LDL-C. Approximately 50 % of the patients receiving XZK achieved a 30 % reduction in LDL-C from baseline [14••].
The majority of reported adverse events were gastrointestinal in both groups. Four percent of participants experienced muscle spasms or myalgia with XZK; however, no one had myopathy, defined in the study protocol as muscle pain with creatine phosphokinase (CPK) elevations ≥10 times the upper limit of normal (ULN). None of the patients in the placebo group reported muscle symptoms. The findings from this trial were similar in both patient populations and consistent with results from previous trials. Other trials have demonstrated XZK’s efficacy in larger populations [15, 16].
Li et al. recently published a large meta-analysis, which examined the effectiveness and safety of RYR as an alternative approach for treating dyslipidemia. Thirteen randomized, placebo-controlled trials were included dating from 1999 to 2013 with treatment duration of 4 weeks to 6 months. All but two trials were conducted at a single site, and no serious side effects were reported. Overall, RYR significantly lowered total and LDL-C levels [−34 (95 % CI −28 to −40) mg/dL; P < 0.001] compared with placebo, but its effect did not appear to be related to the dose, duration of therapy, or geographic location [17].
Tolerability in Patients with a History of Statin Intolerance
Three randomized and one observational trial looked at the tolerability of RYR in patients who discontinued or refused treatment with statins. Halbert et al. compared the tolerability of RYR (Sylvan Bioproducts, Kittanning, PA) with pravastatin in patients with a history of SAM [18]. Patients were eligible to participate if they discontinued use of at least one statin other than pravastatin due to SAM, although many had been rechallenged with other statins. The two primary outcome measures were the incidence of treatment cessation due to recurrent muscle pain and a validated daily pain severity score. Forty-three dyslipidemic patients were randomized to 2400 mg RYR or 20 mg pravastatin twice daily for 12 weeks. Both treatment groups reported low rates of recurrent myalgia, which were not significantly different (5 % in the RYR group and 9 % in the pravastatin group) and achieved similar LDL-C reduction (30 % in the RYR group and 27 % in the pravastatin group). In addition, the mean pain severity score did not significantly differ between the two groups. This study showed that RYR was as well tolerated as pravastatin in a population with a previous history of statin intolerance [18].
Becker et al. evaluated the efficacy and tolerability of the same RYR product (Sylvan Bioproducts, Kittanning, PA) in lowering LDL-C in 62 patients from a community cardiology practice with dyslipidemia and a history of SAM to at least one statin [19]. All patients were asked to complete a self-administered validated questionnaire (Brief Pain Inventory Short Form) at baseline and at weeks 12 and 24, which assessed pain severity and its effect on the functions of daily living. CPK and liver enzymes were measured in all patients to assess safety. Patients were randomized to receive 1800 mg of RYR or placebo twice daily for 24 weeks and were enrolled in a weekly 3.5-h therapeutic lifestyle change program for 12 weeks. LDL-C levels were measured at baseline, at week 12 after the lifestyle program, and at week 24. The mean reduction in LDL-C from baseline was 27 % at week 12 and 21 % at week 24 for the RYR group and 6 and 9 % at weeks 12 and 24, respectively, for the placebo group. The secondary outcome measures including CPK, liver transaminase levels, and pain severity scores did not significantly differ between groups at week 12 or 24. Persistent intolerable myalgias developed in 7 % of the patients in the RYR group and 3 % in the placebo group, but their CPK levels were within normal limits [19].
The RYR product used in this study contained 1.02 mg monacolin K per 600 mg capsule, equivalent to a daily lovastatin dose of 6 mg. This is far less than a standard therapeutic dose, and the authors hypothesized it was likely below the threshold necessary to cause SAM [19]. RYR significantly decreased mean LDL-C levels at week 12 (P < 0.001) and week 24 (P = 0.011) compared with placebo and did not increase the incidence of myalgias. Thirty percent of the participants achieved an LDL-C less than 100 mg/dL [1]. This same group of investigators looked at the lipid-lowering effects of adding 1800 mg phytosterols in tablet form to RYR and found no additional benefit compared to placebo [20•]. These results are surprising because several studies looking at the use of plant stanols and sterols in combination with a statin medication have shown an additive effect of 10 % on average [21, 5].
A small, retrospective, observational study was performed involving 25 patients from a lipid clinic with a history of intolerance to lipid-lowering medications who were treated with RYR for more than 4 weeks. Patients were included if they experienced myalgia (68 %), gastrointestinal side effects (16 %), or elevated liver transaminase levels (8 %) with previous lipid-lowering therapy. Of the 17 patients with myalgias on statins, 53 % had intolerance to daily ezetimibe. Patients randomly selected a 1200 mg RYR supplement taken at bedtime, and CPK and liver transaminase levels were measured in addition to lipids [22].
Similar to that found in other studies, over-the-counter RYR significantly lowered LDL-C by 21 % (P < 0.001) in this clinical population during 74 ± 39 days of treatment. It was well tolerated by 92 % of the study participants, including 89 % of patients with a history of myalgia [22]. One patient developed myalgia, and another reported abdominal bloating. The highest posttreatment CPK level was 130 mg/dL, and alanine aminotransferase levels were initially elevated at two times the ULN in two patients, which persisted at follow-up [22].
Secondary Prevention Trials
The China Coronary Secondary Prevention Study (CCSPS) was the only randomized, double-blinded, placebo-controlled, multicentered study to demonstrate that RYR reduces cardiovascular (CV) risk [15]. This trial recruited 4870 Chinese patients with a history of myocardial infarction and moderate hypercholesterolemia. Patients were randomized to receive twice-daily treatment with 600 mg Xuezhikang (XZK) or placebo. Each 300 mg capsule of XZK contained 2.5 to 3.2 mg of monacolin K equivalent to a total daily lovastatin dose of 10 to 12.8 mg. The primary endpoint was a major coronary event that included nonfatal myocardial infarction and death from coronary heart disease (CHD). After 4.5 years, XZK was associated with a highly significant reduction in frequency of coronary events (10.4 % in the placebo vs 5.7 % in the XZK group) and a relative risk reduction of 45 % [10, 15]. Treatment with XZK also significantly decreased total mortality by 33 %, cardiovascular deaths by 30 %, and the need for coronary revascularization by 33 %. Total cholesterol and LDL-C levels decreased by 13 and 20 %, respectively, compared to baseline (P < 0.001). Adverse effects were similar in both groups, and the XZK appeared to be well tolerated. A sub-study of elderly hypertensive patients in the same CCSPS cohort found that RYR was effective in lowering rates of coronary events and death from CHD compared with placebo [16].
Long-term treatment with XZK significantly reduced the recurrence of coronary events and total mortality in Chinese patients with average LDL-C levels. The results of the CCSPS showed a greater reduction in coronary events than those reported in statin-based outcome trials in Western populations and therefore should be interpreted with caution [23–25]. Additional trials are warranted to confirm these results in other populations with CHD [26]. Review of ClinicalTrials.gov revealed no ongoing outcomes trials.
Legal and Regulatory Status
In 1998, the US Food and Drug Administration (FDA) ruled that Cholestin, the RYR product used in Heber et al.’s study, was “an unapproved drug under the terms of the Federal, Food, Drug, and Cosmetic Act” because Cholestin contained lovastatin, the active ingredient in the prescription drug, Mevacor [1]. Since 2001, the FDA has required manufacturers to remove the monacolin K content from all RYR products, and it continues to be widely available to the public as an over-the-counter supplement. Some recently tested RYR products have been found to contain monacolin K in substantial amounts, and other products may contain little or none of this active ingredient [5]. To avoid violating FDA policy, many commercial RYR products do not disclose the monacolin content on the package label [1]. Therefore, consumers have no way of knowing how much active ingredient is actually present, leaving them unaware as to whether a particular RYR product is effective [27].
Clinical Implications
Public interest in the use of complementary and alternative medications, and skepticism regarding the benefits of available pharmacotherapy, may explain the increased use of RYR in the USA [1]. Compared to statin therapy, RYR is perceived as a “natural” product providing fewer side effects and fewer drug-drug interactions [4]. RYR may be an alternative for patients with a history of statin-related adverse effects. The incidence of SAM may be as high as 15 % [1]. Although an association with statin use is not always clear, muscle pain can undermine medication compliance [13]. Currently, the FDA does not regulate the manufacture of RYR products and as a result there is a lack of quality control and a wide variability of active ingredients [1, 5]. Gordon et al. [28] evaluated the RYR content in ten commercial preparations and found a 100-fold difference in the monacolin K content (0.10 to 10.09 mg) per capsule, although each capsule was labeled as “600 mg per capsule.” Four of the preparations tested contained citrinin, a potential mycotoxin. Citrinin has been shown to cause kidney failure in animal models with a median lethal dose of 35 mg per kg [4, 5, 28]. Similar effects have not been proven in humans, and more studies are needed to clarify if levels detected are toxic [5, 28].
Summary
A growing number of studies have evaluated the effectiveness of RYR in lowering plasma lipids. RYR may have cholesterol-lowering ability because it contains monacolins with HMG CoA reductase activity and possibly other active compounds. Clinical trials have demonstrated significant total, non-HDL-C, and LDL-C lowering with RYR products as monotherapy and as part of a comprehensive preventive strategy. One randomized, placebo-controlled clinical trial demonstrated a reduction in cardiovascular events, but results must be interpreted with caution [15]. Well-powered, multicenter clinical trials, inclusive of Western populations, are needed to examine the efficacy and safety of RYR in the primary and secondary prevention of CHD.
Marketing RYR supplements, which contain more than trace amounts of monacolins, is prohibited in the USA. Monacolin K is identical to lovastatin, and therefore may present an increased risk of muscular and other side effects especially in patients with a history of SAM. Myopathy, hepatoxicity, and rhabdomyolysis have all been reported in patients taking RYR, as one would expect from any statin therapy [29]. For this reason, RYR should be taken under the guidance of a physician who will closely monitor its efficacy, safety, and tolerability [4]. Physicians should weigh the evidence before recommending RYR as an appropriate nonstatin therapy for their patients (Table 2). Until the FDA regulates all over-the-counter supplements, including RYR, physicians and patients should be wary regarding their use [4].
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
Gordon RY, Becker DJ. The role of red yeast rice for the physician. Curr Atheroscler Rep. 2011;13(1):73–80.
Cunningham E. Is red yeast rice safe and effective for lowering cholesterol? J Am Diet Assoc. 2011;111(2):324.
Musselman ME, Pettit RS, Derenski KL. A review and update of red yeast rice. J Evid Based Complement Alternat Med. 2012;17(1):33–9.
Childress L, Gay A, Zargar A, Ito MK. Review of red yeast rice content and current food and drug administration oversight. J Clin Lipidol. 2013;7:117–22.
ConsumerLab.com. Red yeast rice supplements review. http://www.consumerlab.com/reviews/Red-Yeast-Rice-Supplements-Review/Red_Yeast_Rice. Accessed November 7, 2014.
Ma J, Li Y, Ye Q, Li J, Hua Y, Ju D, et al. Constituents of red yeast rice, a traditional Chinese food and medicine. J Agric Food Chem. 2000;48:5220–5.
Becker DJ, Gordon RY, Morris PB, Yorko J, Gordon YJ, Li M, et al. Simvastatin vs therapeutic lifestyle changes and supplements: randomized primary prevention trial. Mayo Clin Proc. 2008;83(7):758–64.
Heber D, Yip I, Ashley JM, Elashoff DA, Elashoff RM, Go VL. Cholesterol-lowering effects of a proprietary Chinese red-yeast-rice dietary supplement. Am J Clin Nutr. 1999;69:231–6.
Downs JR, Clearfield M, Weis S, Whitney E, Shapiro DR, Beere PA, et al. Primary prevention of acute coronary events with lovastatin in men and women with average cholesterol levels: results of AFCAPS/TexCAPS. Air Force/Texas Coronary Atherosclerosis Prevention Study. JAMA. 1998;279(20):1615–22.
Nijjar P, Burke F, Bloesch A, Rader D. Role of dietary supplements in lowering low-density lipoprotein cholesterol: a review. J Clin Lipidol. 2010;4:248–58.
Chen CH, Jc Y, Uang YS, Lin CJ. Improved dissolution rate and oral bioavailability of lovastatin in red yeast rice products. Int J Pharm. 2013;444(1–2):18–24.
Lin CC, Li TC, Lai MM. Efficacy and safety of Monascus purpureus Went rice in subjects with hyperlipidemia. Eur J Endocrinol. 2005;153(5):679–86.
Verhoeven V, Lopez Hartmann M, Remmen R, Wens J, Apers S, Van Royen P. Red yeast rice lowers cholesterol in physicians—a double blind, placebo controlled randomized trial. BMC Complement Altern Med. 2013;13:178–84.
Moriarty PM, Roth EM, Karns A, Ye P, Zhao SP, Liao Y, et al. Effects of Xuezhikang in patients with dyslipidemia: a multicenter, randomized, placebo-controlled study. J Clin Lipidol. 2014;8(6):568–75. This is the first multicenter trial conducted in both the US and China evaluating the efficacy of Xuezhikang (XZK), a purified extract of red yeast rice, to treat dyslipidemia. It randomized 116 patients (53 % white, 37 % Asian) to 1200 or 2400 mg XZK or placebo and followed for 12 weeks. Treatment with XZK resulted in significant reductions in both non-HDL-C and LDL-C compared with placebo. Doubling the dose after 4 weeks resulted in an additional reduction in LDL-C.
Lu Z, Kou W, Du B, Wu Y, Zhao S, Brusco OA, et al. Effect of Xuezhikang, an extract from red yeast Chinese rice, on coronary events in a Chinese population with previous myocardial infarction. Am J Cardiol. 2008;101(12):1689–93.
Li JJ, Lu ZL, Kou WR, Chen Z, Wu Y, Yu XH, et al. Beneficial impact of Xuezhikang on cardiovascular events and mortality in elderly hypertensive patients with previous myocardial infarction from the China Coronary Secondary Prevention Study (CCSPS). J Clin Pharmacol. 2009;49(8):947–56.
Li Y, Jiang L, Jia Z, Xin W, Yang S, Yang Q, et al. A meta-analysis of red yeast rice: an effective and relatively safe alternative approach for dyslipidemia. PLoS One. 2014;9(6):e98611.
Halbert SC, French B, Gordon RY, Farrar JT, Schmitz K, Morris PB, et al. Tolerability of red yeast rice (2400 mg twice daily) versus pravastatin (20 mg twice daily) in patients with previous statin intolerance. Am J Cardiol. 2010;105:198–204.
Becker DJ, Gordon RY, Halbert SC, French B, Morris PB, Rader DJ. Red yeast rice for dyslipidemia in statin-intolerant patients: a randomized trial. Ann Intern Med. 2009;150(12):830–9.
Becker DJ, French B, Morris PB, Silvent E, Gordon RY. Phytosterols, red yeast rice, and lifestyle changes instead of statins: a randomized, double-blinded, placebo-controlled trial. Am Heart J. 2013;166(1):187–96. This study evaluated the lipid lowering effects of phytosterol tablets and lifestyle modification in addition to red yeast rice in patients with statin intolerance. All 187 patients took red yeast rice and were randomized to phytosterol tablets or placebo for 52 weeks. Phytosterols did not significantly improve LDL-C compared with placebo. Patients were also randomized to lifestyle modification or usual care. The lifestyle modification group lost significantly more weight compared to the usual care group and had greater reductions in LDL-C.
Goldberg AC, Ostlund RE, Bateman JH, Schimmoeller L, McPherson TB, Spilburg CA. Effect of plant stanol tablets on low-density lipoprotein cholesterol lowering in patients on statin drugs. Am J Cardiol. 2006;97(3):376–9.
Venero CV, Venero JV, Wortham DC, Thompson PD. Lipid-lowering efficacy of red yeast rice in a population intolerant to statins. Am J Cardiol. 2010;105:664–6.
Sacks FM, Pfeffer MA, Moye LA, Rouleau JL, Rutherford JD, Cole TG, et al. The effect of pravastatin on coronary events after myocardial infarction in patients with average cholesterol levels. N Engl J Med. 1996;335:1001–9.
Scandinavian Simvastatin Survival Study Group. Randomised trial of cholesterol lowering on 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet. 1994;344:1383–9.
The LIPID Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339:1349–57.
Yang CW, Mousa SA. The effect of red yeast rice (Monasucs purpureus) in dyslipidemia and other disorders. Complement Ther Med. 2012;20(6):466–74.
National Center for Complementary and Alternative Medicine. http://nccam.nih.gov. Accessed December 5, 2014.
Gordon RY, Cooperman T, Obermeyer W, Becker DJ. Marked variability of monacolin levels in commercial red yeast rice products: buyer beware! Arch Intern Med. 2010;170:1722–7.
Klimek M, Wang S, Ogunkanmi A. Safety and efficacy of red yeast rice (Monascus purpureus) as an alternative therapy for hyperlipidemia. P&T A PeerRev J Formul Manag. 2009;34(6):313–27.
Compliance with Ethics Guidelines
Conflict of Interest
Frances Burke declares no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
This article is part of the Topical Collection on Nonstatin Drugs
Rights and permissions
About this article

Cite this article
Burke, F.M. Red Yeast Rice for the Treatment of Dyslipidemia. Curr Atheroscler Rep 17, 22 (2015). https://doi.org/10.1007/s11883-015-0495-8
Published:
DOI: https://doi.org/10.1007/s11883-015-0495-8