
Abstract
Characterizing which types of carbohydrates, including whole grains, reduce the risk for coronary heart disease (CHD) is challenging. Whole grains are characterized as being high in resistant carbohydrates as compared with refined grains, meaning they typically are high in fiber, nutrients, and bound antioxidants. Whole grain intake consistently has been associated with improved cardiovascular disease outcomes, but also with healthy lifestyles, in large observational studies. Intervention studies that assess the effects of whole grains on biomarkers for CHD have mixed results. Due to the varying nutrient compositions of different whole grains, each could potentially affect CHD risk via different mechanisms. Whole grains high in viscous fiber (oats, barley) decrease serum low-density lipoprotein cholesterol and blood pressure and improve glucose and insulin responses. Grains high in insoluble fiber (wheat) moderately lower glucose and blood pressure but also have a prebiotic effect. Obesity is inversely related to whole grain intake, but intervention studies with whole grains have not produced weight loss. Visceral fat, however, may be affected favorably. Grain processing improves palatability and can have varying effects on nutrition (e.g., the process of milling and grinding flour increases glucose availability and decreases phytochemical content whereas thermal processing increases available antioxidants). Understanding how individual grains, in both natural and processed states, affect CHD risk can inform nutrition recommendations and policies and ultimately benefit public health.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The 2005 Dietary Guidelines for Americans recommended intake of whole grains, based on evidence from both population and intervention studies, is at least three ounces per day [1]. The Dietary Guidelines Advisory Committee (DGAC) 2010 Report emphasizes fiber-rich carbohydrate foods such as whole grains and vegetables, fruits, and cooked dry beans and peas. It specifically recommends that half of the grains consumed be whole grains, hence some whole grains should replace refined grains [2]. Recent evidence has shown that the beneficial effects of replacing saturated fat with carbohydrate depend on the type of carbohydrate replaced [3, 4]. This raises important questions: what carbohydrates are most beneficial for cardiovascular health, and where do whole grains fit into a healthy diet? This review examines the evidence and the complexities surrounding the use of whole grains to reduce risk for coronary heart disease (CHD).
Carbohydrate Classification: Where do Whole Grains Fit?
Whole grains are referred to as “complex” or “high-quality” carbohydrates, mainly due to their dietary fiber content; however, a specific definition of “high-quality” is needed. One scheme is to differentiate carbohydrates functionally based on their ability to produce a glycemic response (i.e., a rise in blood glucose) [5•]. “Available” carbohydrates (sugars, starches) have α-1-4 and \( \widetilde{\alpha }1 - 6 \) glucosidic linkages that are digested by salivary and pancreatic enzymes and are absorbed readily in the small intestine, eliciting a marked glycemic response. “Resistant” carbohydrates (fiber or non-starch polysaccharides, certain short chain carbohydrates, sugar alcohols) have different glucosidic linkages that limit digestion and absorption, and consequently produce little or no glycemic response [5•].
Another classification scheme is the glycemic index, which compares the postprandial glucose response of carbohydrate-containing foods to that of a standard (i.e., glucose or white bread) [6]. However, the poor within-person reproducibility of the index brings into question how well the index applies on a population-wide scale [7]. Although the glycemic index has been used to characterize foods that decrease risk for chronic disease, the 2010 report of Dietary Guidelines Advisory Committee (DGAC 2010) reported little to no association between glycemic index and weight loss, type 2 diabetes, and cancer, and an inconclusive association with cardiovascular disease (CVD) [2]. Consequently, the overall healthfulness of a carbohydrate-rich food cannot be based solely on its glycemic response because this ignores the type of fiber and the vitamins, minerals, and bioactive non-nutrient plant compounds (phytochemicals) potentially present in these foods. Thus, a chemical definition of grain and grain products yielding a ratio of available to resistant carbohydrates may be a more consistent metric for classifying foods.
Working Definitions of Whole Grains
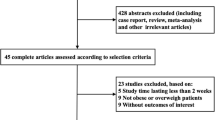
Whole grain products are derived from cereals, which are defined as the fruit of plants belonging to the Poacea (or Gramineae) family of grasses. These include wheat, rice, barley, corn, rye, oats, millets, sorghum, tef, triticale, canary seed, Job’s tears, Fonio, and wild rice (Table 1). The term “pseudo-cereals” includes seeds from non-Gramineae families that function as cereals, such as amaranth, buckwheat, and quinoa [8•]. All grains are comprised of 1) bran—the multi-layered fibrous coat that protects the grain from sun, pests, and diseases; 2) endosperm—the energy supply for the germ and plant; and 3) germ—the embryo of the plant (Fig. 1) [9••].

Structures of whole grains
Because most whole grains are processed, the US Food and Drug Administration (FDA), in concert with the American Association of Cereal Chemists, established a labeling definition. To be considered a “whole grain,” each of the principal components of the grain (endosperm, germ, and bran) must be present in the same relative proportion as they exist naturally in the seed [10]. On the other hand, terms such as “whole wheat” or “multi-grain” are not regulated and can be confusing. Grains can be ground, cooked, parboiled, extruded, pearled, rolled, and even milled (Table 2) as long as the final product has all three parts present in the appropriate proportions.
To ensure that products labeled with a whole grain health claim will provide substantive amounts of whole grains, it must be the first ingredient listed on the ingredient label, meaning it makes up 51% of the product by weight [11]. DGAC 2010 calls for the development of criteria for labeling whole grain foods to decrease confusion both for researchers and consumers [2].
Whole Grain Intake is Associated with Lower CVD Risk and Healthier Lifestyles
Numerous prospective cohort studies of both men and women have reported an inverse relationship between chronic intake of whole grains and CHD, such as heart failure [12], fatal and nonfatal CHD [13, 14], fatal and nonfatal coronary artery disease [15], and fatal ischemic heart disease [16]. The average adjusted hazard ratios from these studies suggest a risk reduction of 7%–30% comparing whole grain consumers versus low or nonconsumers. These studies assessed whole grain intake specifically, rather than fiber, cereal fiber, bran, or low-glycemic carbohydrates, but not all studies used whole grain definitions that met FDA standards [8•]. Jacobs and Gallaher [17] estimated a 20%–40% reduction in CHD risk with frequent whole grain consumption based on 17 prospective cohort studies. In a meta-analysis of 12 prospective cohort studies, Anderson et al. [18] reported a 26% reduction in CHD risk in individuals who consumed whole grains regularly.
DGAC 2010 rated the evidence for the protective relationship between whole grains and CVD as “moderate” [2]. In observational studies, causality cannot be assigned, and it is unknown whether the whole grains are protective or are simply a marker of healthy lifestyles. For example, whole grain intake is positively associated with vitamin use and negatively associated with body mass index (BMI), waist circumference, and smoking status [19]. Another challenge in observational studies is determining the amount of whole grains consumed. Dietary intake data are prone to misreporting and the number of new foods containing whole grains is increasing rapidly. Earlier studies counted whole grain intake from natural grains, dark breads, and cereals with >25% whole grains by weight, whereas current studies count whole grain from any food with as little as 10% whole grain [20]. As whole grains are incorporated into more processed foods, these foods (that may not contain 51% whole grain by weight) must be included in assessing whole grain intake. Indeed, the relationships between whole grain intake and disease status may become less clear as whole grain flour is used in low nutrient density foods such as sugary cereals and pizza. Still, the imprecision in determining whole grain intakes may bias to the null in observational studies, suggesting that whole grain intake may be even more beneficial than hazard ratios indicate [17].
Effects and Mechanisms of Whole Grains on CHD Risk Factors
Dyslipidemia
Numerous cross-sectional studies have reported an inverse association between whole grain intake and dyslipidemia [13, 19, 21]. Intervention trials have produced mixed results, which reflect the type of whole grain studied. Oats and barley improve lipids more than wheat or brown rice, probably because of differences in viscous fiber content. A Cochrane meta-analysis evaluated ten intervention trials (eight of which tested oats) to assess the effect of whole grains on CVD risk factors. Oats consistently lowered total cholesterol (TC) (−0.20 mmol/L; 95% CI, −0.31 to −0.10) and low-density lipoprotein cholesterol (LDL-C) (−0.18 mmol/L; 95% CI, −0.28 to −0.09) compared with the control diets [22]. A recent study with a high-fiber, ready-to-eat oat cereal confirmed this relationship, showing a greater LDL-C–lowering effect than the low-fiber control cereal after 12 weeks in free-living individuals [23]. Furthermore, barley lowered both TC and LDL-C compared with rice [24] and in a dose-dependent manner [25]. Diets containing whole grains low in viscous fiber typically do not affect lipids [26••, 27••].
β-glucan is a type of viscous fiber in barley and oats that increases fecal loss of bile acids, which are derivatives of cholesterol. About 90% of the bile acids entering the small intestine for fat absorption are reabsorbed in the ileum. β-glucan reduces the reabsorption of bile acids, thereby increasing bile acid excretion, lowering the bile acid levels in the liver, and increasing the conversion rate of cholesterol to bile acids. The liver obtains the additional cholesterol by upregulating LDL receptors and increasing LDL particle uptake, thus reducing circulating LDL-C [28]. A viscous fiber intake of 10–25 g/d is recommended by the National Cholesterol Education Program’s Adult Treatment Panel III as an additional diet option to decrease LDL-C. An intake of 5–10 g/d lowers LDL-C by about 5% [29].
Hypertension
Evidence to support benefits of whole grains on hypertension is growing. Two large prospective cohort studies reported that about three servings (16 g per serving) of whole grain per day is associated with a decreased risk of developing hypertension by 19% (95% CI, 75%–87%) in men [30] and by 33% (95% CI, 66%–89%) in women [31]. Multiple types of grains and whole grain foods can lower blood pressure in hypertensive [32, 33] and normotensive (yet hypercholesterolemic) individuals [34]. The hypotensive effects of whole grains are thought to be mediated by improvements in other risk factors such as body weight, dyslipidemia, and insulin resistance. Whole grains are emphasized in the Dietary Approaches to Stop Hypertension (DASH) diet, and increased intake is recommended by the Seventh Panel of the Joint National Committee on the Treatment of Hypertension [35, 36].
Glycemic Control
In large observational studies, whole grains are inversely related to risk of developing type 2 diabetes mellitus [37–39] and are associated with lower serum glucose and insulin [19, 21, 40]. However, randomized controlled trials (RCTs) have reported mixed results on the effects of whole grains on glycemic control. Pereira et al. [41] conducted a controlled-feeding, crossover RCT with 11 hyperinsulinemic adults on either whole or refined grain diets (consisting of 12 30-gram servings per day) for 6 weeks and found an improvement of insulin sensitivity after the whole grain diet. Two large, free-living studies, however, did not find any change in insulin sensitivity in either a cross-over (112 g/d of whole grains for 6 weeks) [42] or a parallel arm (60–120 g/d of whole grains for 8–16 weeks) [27••] study.
Studies examining the glycemic response to different grains (wheat, rye) and whole grain products (breads, pastas) do not provide a consistent explanation for the discrepancy between the observational and intervention studies, but rather raise more questions. First, grains with a higher percentage of amylose starch instead of amylopectin have lower glycemic responses [43]. Amylose (a single strand of glucose molecules) is more resistant to digestion than amylopectin (a highly branched polymer with many sites for hydrolysis) [43]. Second, unprocessed bran (high in fiber) blocks exposure of the rapidly absorbable glucose polymers within the endosperm to digestive enzymes. Interestingly, the presence of finely ground insoluble fiber does not change the glycemic response while intact kernels do [44]. Increased viscosity in the gut may be more effective in lowering glucose responses due to decreased gastric emptying rates and absorption [45]. Third, when grain is ground to produce flour, the surface area for hydrolysis of starch is increased greatly, which would increase glucose absorption [46]. Indeed, whole kernel barley or cracked wheat breads had lower glycemic index values than white bread [46]; however, coarse, ultra-fine, and white wheat flour breads all produced the same glycemic and insulinemic responses in healthy adults [47], perhaps due to the relatively similar particle sizes of flours as compared intact kernels. Fourth, the presence of organic acids (added or from sourdough fermentation) can lower glycemic response, possibly via a lower rate of starch digestion. Despite the lack of fiber, sourdough bread (made with refined wheat flour) produced lower glucose and insulin responses than white, whole wheat and whole-wheat barley breads [48]. The research to date indicates that starch structure, viscosity, particle size, and the presence of organic acids affect glucose availability.
Obesity and Metabolic Syndrome
Increased whole grain intake consistently is associated with lower BMI in the United States [19, 21, 40, 49, 50] and the Netherlands [50]; however, this was not observed in a British population [51]. Longitudinal data from a large cohort of healthy, male health professionals reported that every 40-g/d increment of whole grains was associated with a reduction of 0.49 kg in body weight over 8 years [20]. Whole grains have not, however, facilitated weight loss in the few RCTs that have been conducted [26, 52].
Metabolic syndrome, arising primarily as the result of excess visceral adiposity, is defined by having at least three of following risk factors: increased triglycerides, glucose, blood pressure, and waist circumference and decreased high-density lipoprotein cholesterol (HDL-C) [29]. Whole grain intake of about two servings per day was associated with decreased prevalence of metabolic syndrome in a cross-sectional study [53]. In individuals with metabolic syndrome, the effects of whole grains on glycemic control are mixed, as there are benefits on blood pressure and weight (see previous sections) whereas there are no effects on TG and HDL-C [27••].
Whole grains seem to have the greatest effect on the visceral adipose tissue component of metabolic syndrome. When visceral adipose tissue mass is reduced, there is significant improvement in CVD risk factors, even with only modest weight loss. Whole grain (about three servings per day) and cereal fiber (about 9 g/d) intake were inversely associated with trunk fat mass (as determined by DXA) [54]. For every 10-g/d increment in cereal fiber intake, weight was decreased by 0.77 kg/y (95% CI, −0.127 to −0.026 kg/y) and waist circumference was decreased by 0.10 cm/y (95% CI, −0.18 to 0.02 cm/year) over 6.5 years of follow-up in a European adult cohort [55]. Davis et al. [56••] assessed fiber intake in Latino youth over the course of 2 years and found that decreased fiber intake (average decrease of 3 g of fiber per 1,000 kcal/d) was associated with a 21% increase in visceral fat mass as compared with those who increased fiber intake and decreased visceral fat mass by 4%. Finally, two RCTs reported significantly more visceral fat loss, irrespective of total weight loss, when participants consumed whole grain as compared with refined grain diets for 12 weeks [24, 26••]. The mechanism by which whole grains decrease or prevent visceral fat gain beyond weight loss is unknown; however, it may be due to increased insulin sensitivity in adipose tissue, which decreases adipose lipoprotein lipase activity, thereby reducing fatty acid uptake for storage in visceral fat stores.
Chronic Inflammation
Chronic inflammation is central in the progression of many diseases. Markers of inflammation, such as C-reactive protein (CRP), tumor necrosis factor receptor 2 (TNF-R2) [57], plasminogen activator inhibitor-1 (PAI-1) [58], and interleukin-6 (IL-6) [40], were inversely related to whole grain intake in multiple cross-sectional studies. Some of these relationships were attenuated in a multivariate analysis that included insulin and obesity measures in the model, meaning that the effects of whole grains on insulin resistance and excess adipose tissue could explain the association. In one recent intervention study (n = 50), CRP was lowered on a whole grain diet compared with a refined grain diet [26••]. Conversely, a larger study (n = 316) did not find differences in inflammatory status in participants on a free-living diet who consumed whole or refined grains for 16 weeks [27••].
Components of whole grains, whether in their native and processed states, have a similar antioxidant capacity as do many fruits and vegetables [59]. Most of the phytochemicals are bound in the resistant carbohydrate fraction and are not absorbed unless released by bacteria in the large intestine. Refined grains have only about 20% of the natural antioxidant capacity of whole grains [60]. Some types of processing can actually enhance antioxidant capacity, such as thermal treatment, which releases many of the grain phytochemicals from the bound to the free state, thus maintaining or increasing the antioxidant availability [61].
Resistant Carbohydrates: Fuel for the Gut Microbiota
The interaction between resistant carbohydrates and the microbiota (bacterial population) in the large intestine may contribute to the health benefits of whole grains. Resistant carbohydrates in whole grains fall under the broader definition of prebiotics, meaning they provide fuel for saccharolytic bacteria such as Bifidobacterium [62]. (Probiotics, in contrast, provide bacteria to colonize the colon). It is possible that some of the effects of whole grains on metabolic risk factor are mediated by their abilities to favor the growth of certain types of gut flora.
The majority of the bacteria in the human gut are of the Bacteroidetes (48%) and Firmicutes (51%) divisions, but there is great interpersonal variation in bacterial species, with some people having significant amounts of Bifidobacterium and Lactobacillus [64]. Interestingly, animal [65] and human [66] studies have found differences in bacterial populations between lean and obese individuals [64, 67]. Whether this is a cause, an effect, or unrelated to the obese state is not known. Compared with normal-weight mice, obese mice have 50% less Bacteroidetes and 50% more Firmicutes [65]. During weight loss in humans there was an associated increase in Bacteroidetes, which correlated with weight loss but not caloric intake [65].
These observations suggest that the type of bacteria present in the gut may affect caloric availability, which can affect weight loss (independent of decreased energy intake), and that different types of whole grains may change the character of the biota. The bacterial fermentation of resistant carbohydrates yields different products depending on the type of fuel and bacteria. Fructo-oligosaccharides improve lipid metabolism, immune status, glycemic control and vitamin and mineral absorption, whereas other resistant carbohydrates (resistant starch, inulin) have more varied effects [63]. The products of colonic fermentation are short-chain, volatile fatty acids (SCFA) such as acetate, propionate, and butyrate. The former two enter the portal vein and are metabolized by the liver whereas the latter is an energy source for enterocytes [68]. Acetate, the most abundant product, does not stimulate insulin release, prevents free fatty acid oxidation, and may have a hypercholesterolemic effect by entering cholesterogenic pathways [63]. Propionate may moderate lipid metabolism in humans by competing with acetate for entrance into hepatic cells, thereby preventing excess cholesterol production [63]. An increase in the ratio of propionate to acetate in the portal vein may be responsible for the cholesterol-lowering effect of fermented resistant carbohydrates.
An increase in total SCFA may decrease serum long-chain free fatty acid concentrations, which oppose the action of acetate [69]. Nevertheless, lowering free fatty acid levels can improve the lipid profile and insulin sensitivity by increasing insulin-mediated suppression of gluconeogenesis, decreasing very-low density lipoprotein synthesis and increasing insulin clearance [70]. Hyperinsulinemic individuals supplemented with a high wheat fiber cereal (24 g/d of fiber) for 1 year had an increase in glucagon-like peptide-1 (a hormone related to insulin sensitivity) and SCFA production compared with the low-fiber cereal control group [71]. SCFA levels were increased and free fatty acid levels decreased postprandially in 12 healthy adults after consumption of inulin, a specific fermentable fiber [69]. In summary, whole grains provide fuels that can change the composition of colonic bacteria and also can increase SCFA concentrations and improve postprandial lipid and glycemic processes.
Pros and Cons of Processing
Processing techniques to make grains more palatable and nutritious have been used for centuries. Currently, grains are processed primarily to improve taste but also for nutrition [72] (Table 2). Milling separates the bran and the germ from endosperm that will be used for flour, but all components can be added back into flour at the end of processing. The loss of the bran and germ decreases the nutritional quality of the grain; however, the loss of phytates and fiber increases bioavailability of certain vitamins and minerals. Grinding increases bioavailability of all nutrients in the grain and has both a positive (vitamins, minerals) and negative (glucose) relationship to health. Thermal processing, including industrial and domestic cooking, boiling, parboiling, and baking, can release antioxidants from the bran into the endosperm, increase bioavailability of phytochemicals, and form resistant starch. The fermentation of sourdough bread or the addition of organic acids to grains improves glycemic response in the absence of fiber [48]. Thus, processing improves palatability and digestibility of whole grains, and also may increase antioxidant capacity; some processing techniques, such as milling and decreasing particle size, may offset the health benefits that whole grains provide.
Conclusions
Grains are the primary calorie source for most populations. Increasing consumption of whole grains has the potential to decrease CHD risk in millions of people. An understanding of which grains can most beneficially affect specific risk factors and thereby reduce CHD events can help health professionals make better public health nutrition recommendations. Furthermore, the proper processing techniques of individual grains can confer health benefits. A better understanding of the synergistic effects of whole grain components and their processing on health is needed.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
United States Department of Agriculture, United States Department of Health and Human Services: Dietary Guidelines for Americans, 6th edn. Washington, DC: Government Printing Office; 2005.
United States Department of Agriculture, United States Department of Health and Human Services: Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans. Washington, DC: Government Printing Office; 2010.
Siri-Tarino PW, Sun Q, Hu FB, Krauss RM: Meta-analysis of prospective cohort studies evaluating the association of saturated fat with cardiovascular disease. Am J Clin Nutr 2010, 91:535–546.
Jakobsen MU, Dethlefsen C, Joensen AM, et al.: Intake of carbohydrates compared with intake of saturated fatty acids and risk of myocardial infarction: importance of the glycemic index. Am J Clin Nutr 2010, 91:1764–1768.
• Englyst KN, Liu S, Englyst HN: Nutritional characterization and measurement of dietary carbohydrates. Eur J Clin Nutr 2007, 61(Suppl 1):S19–39. This review thoroughly describes the issues surrounding classifying carbohydrates and provides a framework for a nutritional characterization.
Wolever TM, Jenkins DJ, Jenkins AL, Josse RG: The glycemic index: methodology and clinical implications. Am J Clin Nutr 1991, 54:846–854.
Vega-Lopez S, Ausman LM, Griffith JL, Lichtenstein AH: Interindividual variability and intra-individual reproducibility of glycemic index values for commercial white bread. Diabetes Care 2007, 30:1412–1417.
• De Moura FF: Whole Grain Intake and Cardiovascular Disease and Whole Grain Intake and Diabetes: A review. Bethesda, MD: Life Sciences Research Office; 2008:1–79. This is a thorough review of whole grain observational and intervention studies on cardiovascular disease and diabetes. It assessed evidence of studies testing whole grains that complied with FDA standards versus those that did not.
•• Okarter N, Liu RH: Health benefits of whole grain phytochemicals. Crit Rev Food Sci Nutr 2010, 50:193–208. This is an excellent review on the composition of grains and how they affect CVD risk.
United States Food and Drug Administration: Draft Guidance: Whole Grains Label Statements, Guidance for Industry and FDA Staff. College Park, MD: US Food and Drug Administration; 2006.
United States Food and Drug Administration: Health Claims Notification for Whole Grain Foods. College Park, MD. US Food and Drug Administration; 1999.
Nettleton JA, Steffen LM, Loehr LR, et al.: Incident heart failure is associated with lower whole-grain intake and greater high-fat dairy and egg intake in the Atherosclerosis Risk in Communities (ARIC) study. J Am Diet Assoc 2008, 108:1881–1887.
Jensen MK, Koh-Banerjee P, Hu FB, et al.: Intakes of whole grains, bran, and germ and the risk of coronary heart disease in men. Am J Clin Nutr 2004, 80:1492–1499.
Liu S, Stampfer MJ, Hu FB, et al.: Whole-grain consumption and risk of coronary heart disease: results from the Nurses’ Health Study. Am J Clin Nutr 1999, 70:412–419.
Steffen LM, Jacobs DR Jr, Stevens J, et al.: Associations of whole-grain, refined-grain, and fruit and vegetable consumption with risks of all-cause mortality and incident coronary artery disease and ischemic stroke: the Atherosclerosis Risk in Communities (ARIC) Study. Am J Clin Nutr 2003, 78:383–390.
Jacobs DR Jr, Meyer KA, Kushi LH, Folsom AR: Whole-grain intake may reduce the risk of ischemic heart disease death in postmenopausal women: the Iowa Women’s Health Study. Am J Clin Nutr 1998, 68:248–257.
Jacobs DR Jr, Gallaher DD: Whole grain intake and cardiovascular disease: a review. Curr Atheroscler Rep 2004, 6:415–423.
Anderson JW, Hanna TJ, Peng X, Kryscio RJ: Whole grain foods and heart disease risk. J Am Coll Nutr 2000, 19(Suppl 3):291S–299S.
Newby PK, Maras J, Bakun P, et al.: Intake of whole grains, refined grains, and cereal fiber measured with 7-d diet records and associations with risk factors for chronic disease. Am J Clin Nutr 2007, 86:1745–1753.
Koh-Banerjee P, Franz M, Sampson L, et al.: Changes in whole-grain, bran, and cereal fiber consumption in relation to 8-y weight gain among men. Am J Clin Nutr 2004, 80:1237–1245.
McKeown NM, Meigs JB, Liu S, et al.: Whole-grain intake is favorably associated with metabolic risk factors for type 2 diabetes and cardiovascular disease in the Framingham Offspring Study. Am J Clin Nutr 2002, 76:390–398.
Kelly SA, Summerbell CD, Brynes A, et al.: Wholegrain cereals for coronary heart disease. Cochrane Database Syst Rev 2007, 2:CD005051.
Maki KC, Beiseigel JM, Jonnalagadda SS, et al.: Whole-grain ready-to-eat oat cereal, as part of a dietary program for weight loss, reduces low-density lipoprotein cholesterol in adults with overweight and obesity more than a dietary program including low-fiber control foods. J Am Diet Assoc 2010, 110:205–214.
Shimizu C, Kihara M, Aoe S, et al.: Effect of high beta-glucan barley on serum cholesterol concentrations and visceral fat area in Japanese men—a randomized, double-blinded, placebo-controlled trial. Plant Foods Hum Nutr 2008, 63:21–25.
Behall KM, Scholfield DJ, Hallfrisch J: Lipids significantly reduced by diets containing barley in moderately hypercholesterolemic men. J Am Coll Nutr 2004, 23:55–62.
•• Katcher HI, Legro RS, Kunselman AR, et al.: The effects of a whole grain-enriched hypocaloric diet on cardiovascular disease risk factors in men and women with metabolic syndrome. Am J Clin Nutr 2008, 87:79–90. This randomized controlled trial compared whole and refined grain weight-loss diets and found a significant decrease in abdominal fat mass loss and CRP in the whole grain group despite equal weight loss between groups.
•• Brownlee IA, Moore C, Chatfield M, et al.: Markers of cardiovascular risk are not changed by increased whole-grain intake: the WHOLEheart study, a randomised, controlled dietary intervention. Br J Nutr 2010, 104:125–134. This study is the largest whole grain intervention study to date. It failed to find any improvement in risk factors for cardiovascular disease, but compliance is thought to have been an issue in this free-living study.
Papathanasopoulos A, Camilleri M: Dietary fiber supplements: effects in obesity and metabolic syndrome and relationship to gastrointestinal functions. Gastroenterology 2010, 138:65–72.
National Heart Lung and Blood Institute: Third Report of the Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Edited by National Cholesterol Education Program. Bethesda, MD: National Institutes of Health; 2002.
Flint AJ, Hu FB, Glynn RJ, et al.: Whole grains and incident hypertension in men. Am J Clin Nutr 2009, 90:493–498.
Wang L, Gaziano JM, Liu S, et al.: Whole- and refined-grain intakes and the risk of hypertension in women. Am J Clin Nutr 2007, 86:472–479.
Keenan JM, Pins JJ, Frazel C, et al.: Oat ingestion reduces systolic and diastolic blood pressure in patients with mild or borderline hypertension: a pilot trial. J Fam Pract 2002, 51:369.
Pins JJ, Geleva D, Keenan JM, et al.: Do whole-grain oat cereals reduce the need for antihypertensive medications and improve blood pressure control? J Fam Pract 2002, 51:353–359.
Behall KM, Scholfield DJ, Hallfrisch J: Whole-grain diets reduce blood pressure in mildly hypercholesterolemic men and women. J Am Diet Assoc 2006, 106:1445–1449.
National Heart Lung and Blood Institute: Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC7). Bethesda, MD: National Institutes of Health; 2004.
Appel LJ, Moore TJ, Obarzanek E, et al.: A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N Engl J Med 1997, 336:1117–1124.
Liu S, Manson JE, Stampfer MJ, et al.: A prospective study of whole-grain intake and risk of type 2 diabetes mellitus in US women. Am J Public Health 2000, 90:1409–1415.
de Munter JS, Hu FB, et al.: Whole grain, bran, and germ intake and risk of type 2 diabetes: a prospective cohort study and systematic review. PLoS Med 2007, 4:e261.
Fung TT, Hu FB, Pereira MA, et al.: Whole-grain intake and the risk of type 2 diabetes: a prospective study in men. Am J Clin Nutr 2002, 76:535–540.
Lutsey PL, Jacobs DR Jr, Kori S, et al.: Whole grain intake and its cross-sectional association with obesity, insulin resistance, inflammation, diabetes and subclinical CVD: The MESA Study. Br J Nutr 2007, 98:397–405.
Pereira MA, Jacobs DR Jr, Pins JJ, et al.: Effect of whole grains on insulin sensitivity in overweight hyperinsulinemic adults. Am J Clin Nutr 2002, 75:848–855.
Andersson A, Tengblad S, Karlstrom B, et al.: Whole-Grain Foods Do Not Affect Insulin Sensitivity or Markers of Lipid Peroxidation and Inflammation in Healthy, Moderately Overweight Subjects. J Nutr 2007, 137:1401–1407.
Behall KM, Scholfield DJ, Canary J: Effect of starch structure on glucose and insulin responses in adults. Am J Clin Nutr 1988, 47:428–432.
Juntunen KS, Laaksonen DE, Autio K, et al.: Structural differences between rye and wheat breads but not total fiber content may explain the lower postprandial insulin response to rye bread. Am J Clin Nutr 2003, 78:957–964.
Hallfrisch J, Behall KM: Mechanisms of the effects of grains on insulin and glucose responses. J Am Coll Nutr 2000, 19(Suppl 3):320S–325S.
Jenkins DJ, Wesson V, Wolever TM, et al.: Wholemeal versus wholegrain breads: proportion of whole or cracked grain and the glycaemic response. BMJ 1988, 297:958–960.
Behall KM, Scholfield DJ, Hallfrisch J: The effect of particle size of whole-grain flour on plasma glucose, insulin, glucagon and thyroid-stimulating hormone in humans. J Am Coll Nutr 1999, 18:591–597.
Najjar AM, Parsons PM, Duncan AM, et al.: The acute impact of ingestion of breads of varying composition on blood glucose, insulin and incretins following first and second meals. Br J Nutr 2009, 101:391–398.
Good CK, Holschuh N, Albertson AM, et al.: Whole grain consumption and body mass index in adult women: an analysis of NHANES 1999–2000 and the USDA pyramid servings database. J Am Coll Nutr 2008, 27:80–87.
van de Vijver LP, van den Bosch LM, van den Brandt PA, Goldbohm RA: Whole-grain consumption, dietary fibre intake and body mass index in the Netherlands cohort study. Eur J Clin Nutr 2009, 63:31–38.
Thane CW, Stephen AM, Jebb SA: Whole grains and adiposity: little association among British adults. Eur J Clin Nutr 2009, 63:229–237.
Saltzman E, Moriguti JC, Das SK, et al.: Effects of a cereal rich in soluble fiber on body composition and dietary compliance during consumption of a hypocaloric diet. J Am Coll Nutr 2001, 20:50–57.
Sahyoun NR, Jacques PF, Zhang XL, et al.: Whole-grain intake is inversely associated with the metabolic syndrome and mortality in older adults. Am J Clin Nutr 2006, 83:124–131.
McKeown NM, Yoshida M, Shea MK, et al.: Whole-grain intake and cereal fiber are associated with lower abdominal adiposity in older adults. J Nutr 2009, 139:1950–1955.
Du H, van der AD, Boshuizen HC, et al.: Dietary fiber and subsequent changes in body weight and waist circumference in European men and women. Am J Clin Nutr 2009, 91:329–336.
• Davis JN, Alexander KE, Ventura EE, et al.: Inverse relation between dietary fiber intake and visceral adiposity in overweight Latino youth. Am J Clin Nutr 2009, 90:1160–1166. The reduction of visceral fat without weight loss in diets higher in fiber, which is prevalent in whole grains, is a novel finding. Associating longitudinal dietary and anthropometric data makes the relationship stronger.
Qi L, van Dam RM, Liu S, et al.: Whole-grain, bran, and cereal fiber intakes and markers of systemic inflammation in diabetic women. Diabetes Care 2006, 29:207–211.
Masters RC, Liese AD, Haffner SM, et al.: Whole and refined grain intakes are related to inflammatory protein concentrations in human plasma. J Nutr 2010, 140:587–594.
Adom KK, Liu RH: Antioxidant activity of grains. J Agric Food Chem 2002, 50:6182–6187.
Adom KK, Sorrells ME, Liu RH: Phytochemicals and antioxidant activity of milled fractions of different wheat varieties. J Agric Food Chem 2005, 53:2297–2306.
Dewanto V, Wu X, Liu RH: Processed sweet corn has higher antioxidant activity. J Agric Food Chem 2002, 50:4959–4964.
Gibson GR, Roberfroid MB: Dietary modulation of the human colonic microbiota: introducing the concept of prebiotics. J Nutr 1995, 125:1401–1412.
Delzenne NM, Williams CM: Prebiotics and lipid metabolism. Curr Opin Lipidol 2002, 13:61–67.
Tsai F, Coyle WJ: The microbiome and obesity: is obesity linked to our gut flora? Curr Gastroenterol Rep 2009, 11:307–313.
Turnbaugh PJ, Ley RE, Mahowald MA, et al.: An obesity-associated gut microbiome with increased capacity for energy harvest. Nature 2006, 444:1027–1031.
Ley RE, Turnbaugh PJ, Klein S, Gordon JI: Microbial ecology: human gut microbes associated with obesity. Nature 2006, 444:1022–1023.
Mai V, Draganov PV: Recent advances and remaining gaps in our knowledge of associations between gut microbiota and human health. World J Gastroenterol 2009, 15:81–85.
Elia M, Cummings JH: Physiological aspects of energy metabolism and gastrointestinal effects of carbohydrates. Eur J Clin Nutr 2007, 61(Suppl 1):S40–74.
Tarini J, Wolever TM: The fermentable fibre inulin increases postprandial serum short-chain fatty acids and reduces free-fatty acids and ghrelin in healthy subjects. Appl Physiol Nutr Metab 2010, 35:9–16.
Hennes MM, Dua A, Kissebah AH: Effects of free fatty acids and glucose on splanchnic insulin dynamics. Diabetes 1997, 46:57–62.
Freeland KR, Wilson C, Wolever TM: Adaptation of colonic fermentation and glucagon-like peptide-1 secretion with increased wheat fibre intake for 1 year in hyperinsulinaemic human subjects. Br J Nutr 2010, 103:82–90.
Slavin JL, Jacobs D, Marquart L: Grain processing and nutrition. Crit Rev Biotechnol 2001, 21:49–66.
Alminger M, Eklund-Jonsson C: Whole-grain cereal products based on a high-fibre barley or oat genotype lower post-prandial glucose and insulin responses in healthy humans. Eur J Nutr 2008, 47:294–300.
Berger A, Rein D, Schafer A, et al.: Similar cholesterol-lowering properties of rice bran oil, with varied gamma-oryzanol, in mildly hypercholesterolemic men. Eur J Nutr 2005, 44:163–173.
Disclosure
PM Kris-Etherton’s and KA Harris’ employer has received a grant from General Mills to conduct clinical trials assessing the effect of whole grains on metabolic syndrome.
KA Harris is supported by the Nestle PhD, RD Training Fellowship, which is a competitive award funded by Nestle Research Center for a nutritional science graduate student pursuing both degrees at the Pennsylvania State University.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Harris, K.A., Kris-Etherton, P.M. Effects of Whole Grains on Coronary Heart Disease Risk. Curr Atheroscler Rep 12, 368–376 (2010). https://doi.org/10.1007/s11883-010-0136-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11883-010-0136-1