
Abstract
The daily deposited dose of bioaerosols and particle mass or number in the human respiratory tract using an exposure dose model (ExDoM2) was quantified in the present study. The dose was calculated for the extrathoracic (ET), tracheobronchial (TB), and alveolar-interstitial (AI) regions of the human respiratory tract. The calculations were performed for viable, cultivable airborne heterotrophic bacteria, mesophilic fast-growing fungi, and total coliforms at a municipal wastewater treatment plant (WWTP) located at a suburban area at a Mediterranean site. The human dose was determined using data from two locations at the WWTP which correspond to two different wastewater treatment stages (aerated grit chamber (indoor) and primary settling tanks (outdoor)) and one outdoor location at the urban background site. In addition, the model simulations were performed for two exposure periods (March to April and May to June 2008). Higher daily deposited dose in the total human respiratory tract was observed for heterotrophic bacteria at the aerated grit chamber, whereas lower values of heterotrophic bacteria were observed at the primary settling tanks. These findings were associated with the corresponding stage of wastewater treatment activities and may be valuable information for determining future dose–response relationships. In addition, higher daily deposited dose was determined in the ET region for the three categories of bioaerosols. Regarding PM10 and PN1, the higher daily deposited dose received by a worker at the aerated grit chamber. Finally, the hazard quotients were estimated and the results showed that the non-carcinogenic effects can be ignored for bioaerosols and PM10 except for workers present at aerated grit chamber. Regarding PM2.5, the non-carcinogenic effects are of concern and cannot be ignored for all cases.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Bioaerosols are emitted from natural sources (e.g., soil, water bodies, plant surfaces) and anthropogenic activities (e.g., landfills, composting facilities, wastewater treatment plants (WWTPs)) (Despres et al. 2012; Katsivela et al. 2017; Χie et al. 2021). In particular, WWTPs emit significant amounts of microorganisms in air during the different stages of wastewater treatment such as the aeration and mechanical sewage moving (Han et al. 2020; Benami et al. 2016; Katsivela et al. 2017; Yang et al. 2019; Yan et al. 2021; Xu et al. 2020). Karra and Katsivela (2007) observed a gradual decrease of bioaerosol emissions during the advanced wastewater treatment from the pretreatment to the primary, secondary, and tertiary treatment. Xu et al. (2020) asserted that aerated grit chamber (AGC) and sludge thickening house (STH) were the main indoor emission sources for airborne bacteria while for outdoor air was the aeration tank. Yan et al. (2021) found that the concentration of bioaerosols was below 103 CFU/m3 in a WWTP. In addition, Kowalski et al. (2017) found that air near WWTPs contained elevated concentrations of bioaerosols (5.3 × 101–1.1 × 103 CFU/m3 for bacterial aerosol and 6.3 × 102–1.2 × 103 CFU/m3 for fungal aerosol). These elevated bioaerosol concentrations may cause health risk not only to workers but also to nearby residents (Yan et al. 2021; Xu et al. 2020), but there is no international accepted threshold limit value for their concentrations (Yan et al. 2021). Exposure to bioaerosols was linked with health problems such as infectious diseases (e.g., Legionnaire’s disease), respiratory diseases (e.g., chronic bronchitis), allergic diseases (e.g., asthma) and bioterrorism (Korzeniewska 2011; Secondo et al. 2021; Sturm 2016). It should be noted that part of bioaerosols and airborne particles cannot enter the human respiratory tract or can enter but exhaled. The deposition in the human respiratory tract depends on physicochemical properties of the aerosol (size distribution, density, and shape factor), physiological parameters (inhalation rate, tidal volume, volumetric flow rate of inspired air of breathing, breathing pattern), and anatomical parameters (respiratory tract morphology) (ICRP 1994; Aleksandropoulou and Lazaridis 2013; Brown 2015). The particles deposit in the human respiratory tract mainly by the mechanisms of impaction, sedimentation and diffusion. Each region in the human respiratory tract has different dominant mechanisms and the relative contribution of each depends on the integration of the aerosol physicochemical properties (size, distribution, density) with airway architecture and physiological parameters. Generally, the dominant mechanism for ET region is the impaction, for TB is the sedimentation and impaction while for AI region is the diffusion (Darquenne 2020). In addition, the physicochemical properties of particles (size, density, shape factor) are important parameters for the toxicity of particles (Nel et al. 2009). Therefore, the knowledge of regional deposition and specific dose of bioaerosols at different parts of the respiratory tract is important for the determination of health effects due to inhalation exposure (Secondo et al. 2021).
In addition, WWTPs are also important sources of airborne particles in term of particle mass (PM) and number (PN). Widiana et al. (2017) found in a municipal WWTP in North Taiwan that the annual PM10 concentration was equal to 45 μg/m3, a value that exceeds the annual value recommended by the WHO (20 μg/m3) and EU (40 μg/m3) for the protection of human health. Furthermore, Piqueras et al. (2016) asserted that semi covered aeration tanks emit airborne particles which can affect the health of nearby residents. Specifically, the number concentration in the aeration tank at Orange County Sanitation District (Fountain Valley, CA) ranged from 7000 to 18,000 #/cm3 (Piqueras et al. 2016). In addition, Yang et al. (2021) performed field measurements with a scanning mobility particle sizer (SMPS) and an aerodynamic particle sizer (APS) at moving bed biofilm reactor (MBBR) at a municipal WWTP located in China.
Several studies (Cho et al. 2005; Secondo et al. 2021; Madhwal et al. 2020) determined the deposition of bioaerosols in the human respiratory tract (extrathoracic (ET), tracheobronchial (TB), and alveolar-interstitial (AI) regions) using deposition models (e.g., multiple-path particle dosimetry (MPPD V 3.04) model, lung dose evaluation program (LUDEP)). LUDEP is a user-friendly program which developed from ICRP (1994) for calculation of deposition of radionuclides particles in the human respiratory tract, whereas, the MPPD V 3.04 model was developed by Applied Research Associates (https://www.ara.com/mppd/) with the contribution of several agencies (Chemical Industry Institute of Toxicology (CIIT), Dutch National Institute of Public Health and Environment (RIVM), National Institute for Occupational Safety and Health (NIOSH), Defense Advanced Research Projects Agency (DARPA), Environmental Protection Agency (EPA)) for calculation of deposition of airborne particles.
Secondo et al. (2021) performed field measurements in apartments in the northeastern US and used the MPPD and ICRP dosimetry for the calculation of deposition. The authors found that the majority of fungal spore’s deposit in the ET region while there is a significant deposition for both Aspergillus and Cladosporium spores in the AI region which potentially cause aspergillosis or allergic asthma. Cho et al. (2005) performed measurements under controlled laboratory conditions. The authors used the LUDEP model for the calculation of respiratory deposition for fragments and spores and found that fragments had 230–250-fold higher respiratory deposition than spores of the fungal specie of Stachybotrys chartarum. In addition, Madhwal et al. (2020) conducted bioaerosols measurements in an open landfill site using the MPPD model and observed that the total deposited dose rate of fungal species was greater than the bacterial ones.
Regarding PM, Chalvatzaki et al. (2018, 2021) used the exposure dose model (ExDoM2) for the calculation of personal deposited dose in the human respiratory tract for three European cities and for six major Greek cities respectively. Specifically, Chalvatzaki et al. (2018) found that the daily deposited dose in the human respiratory tract was higher for a resident in Lisbon (378 μg/day) with particles deposited mainly in the ET region (266 μg/day). The study of Chalvatzaki et al. (2021) reported higher deposited dose rate for all urban locations compared with suburban locations. In addition, Chalvatzaki et al. (2020) used the ExDoM2 for the estimation of personal deposited dose of PM10 and PM10-bound metals for 10-year-old school children in Lisbon. Particularly, Chalvatzaki et al. (2020) found that indoor school environment contributed 44% to the weekly deposited dose of PM10.
The current study aims to determine the total and regional daily deposited dose of bioaerosols and particles in terms of mass and number in the human respiratory tract using the exposure dose model (ExDoM2). Input data from a municipal WWTP and an urban background site were obtained from Katsivela et al. (2017). Specifically, the simulations were performed for viable, cultivable airborne microorganisms (heterotrophic bacteria, mesophilic fungi, and total coliforms) emitted from a municipal WWTP in a suburban area of the city of Chania on the island of Crete (Greece). In addition, the impact of different characteristics (age, gender, and exertion level) of the exposed subject to the daily deposited dose was also investigated. Finally, non-cancer toxicity hazard quotients (HQ) was calculated for airborne bioaerosols and particle mass (PM10 and PM2.5).
Materials and methods
Study site and experimental data
Measurements of viable, cultivable potentially pathogenic microorganisms (airborne heterotrophic bacteria, mesophilic fast-growing fungi, and total coliforms) were performed by Katsivela et al. (2017) at a municipal WWTP in a suburban area of the city of Chania (Greece, Crete), and an urban background site, located 5 km from the WWTP which was used as a control site. Specifically, sampling points were established at three locations: (1) aerated grit chamber (AGC), (2) primary settling tanks (PST), and (3) urban background (UB) site (see Fig. 1). The AGC is an indoor pretreatment stage of WWTP, while PST is located outdoors (partially covered) and is a part of the primary treatment of WWTP. The third location (UB) is an outdoor background location (a courtyard with small garden). The field measurements were performed from 12/03/2008 to 19/06/2008 for bioaerosols (heterotrophic bacteria, messophilic fungi, and total coliforms) as well as for inhalable PM (mass concentration of PM10, PM2.5, PM1, and number concentration of PM1 particles). Specifically, measurements performed for 11 days (5 days during March to April and 6 days during May to June) in the time interval 10:30 a.m. to 3:30 p.m. Bioaerosols were collected using a six-stage (0.65–1.1 μm, 1.1–2.1 μm, 2.1–3.3 μm, 3.3–4.7 μm, 4.7–7 μm, and > 7 μm) viable Andersen cascade impactor (Thermo ESM Andersen Instruments GmbH, Germany). Only cultivable and viable airborne microorganisms were determined. The analysis is based on the cultivation of the messophilic fungi, heterotrophic bacteria, and total coliforms in malt extract agar (Lab M, England), tryptone soy broth (Merck, Germany), and membrane lauryl sulfate broth (Lab M, England), respectively. The microbial concentration for each stage was expressed as number of colony-forming units per unit volume of air (CFU/m3).

Location of WWTP (AGC and PST) and UB site (source: Google earth). AGC, aerated grit chamber; PST, primary settling tanks; UB, urban background site
In addition, particle mass (PM) concentrations for three different size categories (PM10, PM2.5, and PM1) were determined using portable aerosol particulate monitor (Dust-Trak instrument, TSI, Germany), while a portable ultrafine particle counter (P-Trak instrument, TSI, Germany) measured the cumulative counts of PN1 (number) particles. The measurements with the Dust-Trak were corrected based on the beta attenuation monitor (FH 62 SEQ) (Thermo). Specifically, the Eq. (1) was used:
The wind speed was measured on a meteorological mast at the WWTP using wind speed sensor 4034 BG (Theodor Friedrichs and Co., Germany). The wind speed values were used as input for the calculation of inhalability. More details for the site and field measurements can be found in the study of Katsivela et al. (2017).
Dosimetry model
Simulations were performed using the ExDoM2 dosimetry model. The respiratory tract deposition model of ExDoM2 (Chalvatzaki and Lazaridis 2015) is based on the human respiratory tract model (HRTM) of ICRP (1994, 2015). The deposited dose rates (CFU/h for bioaerosols, #/h for particle number (PN) and μg/h for particle mass (PM)) were calculated according to Eq. (2):
where \({C}_{i}\) is the exposure concentration (CFU/m3 for bioaerosols, #/m3 for PN and μg/m3 for PM) for particles in the size fraction \(i\), \(B\) is the inhalation rate (m3/h), \({DE}_{i,j}\) is the deposition fraction in region \(j\) of the respiratory tract for particles in the size fraction \(i\). The inhalation rate \(B\) was set equal to 1.5 m3/h for an adult male under light exercise (ICRP 1994). In addition, the deposition fractions \({(DE}_{i,j})\) were calculated with the equations of ICRP (1994, 2015). The daily deposited dose was calculated as the product of deposited dose rate and exposure time. The simulations were implemented assuming a 24-h exposure scenario under the same conditions, therefore, input data (e.g., exposure concentration, inhalation rate) preserved the same values.
The nasal inhalability \(({n}_{I})\) for wind speed ranged from 1 to 9 m/s was calculated from the Eq. (3) while for wind speed less than 1 m/s the Eq. (4) was used (Aleksandropoulou and Lazaridis 2013; ICRP 1994; Ménache et al. 1995):
where \(u\) is the wind speed (m/s) and \({d}_{ae}\) is the aerodynamic diameter (μm).
The \({n}_{I}\) was used in the ExDoM2 dosimetry model for the calculation of the deposition fraction. Specifically, the deposition fraction in each filter (the model treats the human respiratory tract as a series of filters) depends on the fraction of tidal air that reaches the filter, the prefiltration efficiency (n0 = 1-\({n}_{I}\)) and deposition efficiency of each filter (nj).
The human respiratory tract is divided into nine filters: two filters for the anterior nose region (ET1); two filters in the posterior nasal passages, pharynx, and larynx region (ET2); two filters in the bronchial (BB) region; two filters in the bronchiolar (bb) region; and one filter in the alveolar-interstitial (AI) region.
The deposition efficiency of each filter nj was calculated with the following equation (ICRP 1994):
where, nae is the aerodynamic deposition efficiency due to impaction and gravitational settling and nth is the thermodynamic deposition efficiency due to diffusion.
The aerodynamic and thermodynamic deposition efficiency was calculated by (ICRP 1994):
where a and p are dimensionless constants, R has a characteristic functional form that is different in each region and depends on particle size and the relevant respiration parameters.
The respiratory tract deposition module of ExDoM2 incorporates new data from ICRP (2015). Specifically, according to the ICRP (2015), the particles deposited in the ET are partitioned 65% to ET1 and 35% to ET2. In addition, the respiratory tract clearance module of ExDoM2 incorporates a new particle clearance mechanism in the respiratory tract based on the ICRP (2015). The clearance mechanisms for the calculation of retained dose in the respiratory tract and the dose to the blood, oesophaugus and lymph nodes were not taken into consideration in the current study.
ExDoM2 dosimetry model take into account the size distribution data as input for the calculation of the median aerodynamic diameters (MADs) and standard deviation (σg). In addition, the user can enter different particle size distribution measurements for determining realistic exposure scenario at different microenvironments during the day. The particle size distribution from the impactor was used as input in the ExDoM2, whereas the size distribution characteristics (MMD, CMD, MMAD, σg) was used as input in the MPPD.
The most important input data for the implementation of the ExDoM2 dosimetry model are (1) age and gender of exposed subject, (2) breathing pattern of the exposed subject (nose breather or mouth breather), (3) activity level, (4) exposure concentration, (5) size distribution data, (6) particle density, (7) shape factor, and (8) wind speed. In the current study, the exposed subject was considered adult male and nose breather under light exercise. The wind speed ranged from 4.8 to 24.0 m/s with an average value of 9.6 m/s during P1 period, while during P2 period the wind speed ranged from 3.0 to 19.5 m/s with an average value of 8.0 m/s. According to the Löndahl (2014), the shape factor of bioaerosols vary from spherical to elongated structures whereas the density is about 1.0–1.5 g/cm3. The same density and shape factor was used for all cases. Specifically, the density and shape factor were set equal to 1.5 g/m3 and 1 (spherical), respectively. The size distribution data of viable Andersen cascade impactor were used as input for the calculation of the MADs. The MADs of bioaerosols can be considered as CMADs.
Inhalation health risk assessment
The inhalation health risk assessment methodology developed by the United States Environmental Protection Agency (US EPA 2009, 2013) was used in the current study. The non-carcinogenic risk of bioaerosols and particle mass (PM10 and PM2.5) was expressed by the hazard quotient (HQ) and was calculated with the following equation (US EPA 2009, 2013; Han et al. 2019; Yunesian et al. 2019):
where \(\mathrm{ADD}\) is the average daily dose or intake (CFU/kg/day for bioaerosols and μg/kg/day for PM10), \(\mathrm{RFD}\) is the reference dose (CFU/kg/day or μg/kg/day), \({C}_{\mathrm{total}}\) is the pollutant concentration (CFU/m3 for bioaerosols and μg/m3 for PM10), \(\mathrm{IR}\) is the inhalation rate (m3/day), \(\mathrm{EF}\) is the exposure frequency (days/year), \(\mathrm{ED}\) is the exposure duration (years), \(\mathrm{BW}\) is the body weight (kg) of the exposed subject, \(\mathrm{AT}\) is the averaging time (days), and \(\mathrm{RFC}\) corresponds to a reference concentration (CFU/m3 for bioaerosols and μg/m3 for PM10).\(\mathrm{HQ}\le 1\) indicates non-carcinogenic effects are not of concern while \(\mathrm{HQ}>1\) suggests that the non-carcinogenic effects are of concern and cannot be ignored (Lu et al. 2020).
The exposure duration (\(\mathrm{ED}\)) was considered equal to 25 years (occupational value) while the averaging time (\(\mathrm{AT}\)) was considered equal to 9125 days (\(\mathrm{ED}\) ×365 days/year) (US EPA 2013). Furthermore, the exposure frequency (\(\mathrm{EF}\)) were set equal to 250 days/year (occupational value) according to the US EPA (2013). The \(\mathrm{RFD}\) or \(\mathrm{RFC}\) upper limit values for the airborne bacteria or fungi are not available, and therefore, the reference value of 500 CFU/m3 (Han et al. 2019; Lu et al. 2020) was used in the current study. The air quality guidelines levels of WHO (2021) was used as \(\mathrm{RFC}\). Specifically, the value of 45 μg/m3and 15 μg/m3 was used for PM10 and PM2.5, respectively.
Results and discussion
Bioaerosols concentrations and corresponding deposited dose
Bioaerosol concentrations and corresponding deposited dose were classified into two periods (P1 and P2) corresponding to March to April and May to June 2008, respectively. The daily concentrations of viable, cultivable airborne bioaerosols (heterotrophic bacteria, mesophilic fast-growing fungi, and total coliforms) and the corresponding daily deposited dose during the measurement periods at AGC, PST, and UB sites are shown in Figs. 2 and 3, respectively.

Daily concentrations of viable, cultivable airborne heterotrophic bacteria, mesophilic fast-growing fungi, and total coliforms during March to April (P1) and May to June (P2) of 2008 at the aerated grit chambers (AGC), primary settling tanks, (PST), and urban background (UB) site. The whiskers vary between minimum and maximum values (excluding outliers) and the boxes depicts 25th, 50th, and 75th percentile. The red cross indicates outliers

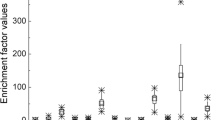
Daily deposited dose (CFU/day) of viable, cultivable airborne heterotrophic bacteria, mesophilic fungi, and total coliforms in the human respiratory tract (extrathoracic (ET), tracheobronhcial (TB), and alveolar-interstitial (AI) regions) during March to April (P1) and May to June (P2) at the a) aerated grit chambers (AGC), b) primary settling tanks (PST), and c) urban background (UB) site
Higher concentration of heterotrophic bacteria as well as deposited dose was observed at AGC. Specifically, the highest concentrations of the heterotrophic bacteria were measured at AGC in a range of 1300–3995 CFU/m3 and 2255–5115 CFU/m3 for P1 and P2 periods, respectively. In addition, higher values of the heterotrophic bacteria were observed during P2 period. Particularly, the highest daily deposited dose of heterotrophic bacteria in the human respiratory tract (sum of all regions) was received by a worker at AGC during the P2 period (71,480–161,663 CFU/day). The workers at AGC received higher dose of heterotrophic bacteria as direct consequence of the flow of raw wastewater through the AGC which have higher microbial community in comparison with the wastewater at PST. The poorly treated wastewater results in high load of airborne hetetrotrophic bacteria and consequently to higher human dose. PST preserved considerably lower levels which confirm previous observations that the concentration of the heterotrophic bacteria depends from the stage of the treatment plant (Karra and Katsivela 2007; Katsivela et al. 2017). Therefore, the first stages of the WWTP are the stages with the highest concentration and corresponding deposited dose of heterotrophic bacteria as also concluded from the work of Katsivela et al. (2017).
Regarding mesophilic fungi, higher values were observed at UB site during the P1 period due to fungi abundance at ambient air. Specifically, the concentration of meshophili fungi ranged from 155–1050 CFU/m3 whereas the corresponding daily deposited dose ranged from 4577–27,642 CFU/day during the P1 period. This finding is linked with the fact that terrestrial organisms which existing in the soil and plants of garden can affect the concentrations levels of mesophilic fungi and hence are more likely to be found in the UB site than at WWTP (Katsivela et al. 2017). In addition, airborne total coliforms were measured only at AGC (pretreatment stage). Specifically, the highest daily deposited dose in the human respiratory tract of coliforms (146–3098 CFU/day) was received by a worker at AGC during the P2 period. Therefore, the wastewater treatment from the pretreatment to the primary treatment resulted to an efficient decrease of total coliforms.
Moreover, the results indicate that higher deposited dose was obtained in the ET region compared to the other regions. Specifically, the deposited dose was higher in the ET region, followed by AI and TB region. This finding is associated with the characteristics (MAD, σg, and % contribution) of size distribution data of bioaerosols (Table 1). In the current study, the contribution of particles with aerodynamic diameter greater than 2.1 μm is above 50% for all cases and hence due to their large size deposit mainly in the ET region. Different size distribution data per day was used in the simulations. However, Fig. 4 and Table 1 show the average size distribution data for each period. Likewise, Secondo et al. (2021) asserted that fungal spores deposited mainly in the ET region for residents in apartments in the northeastern US. Particularly, Fig. 4 indicates that the mesophilic fungi showed a maximum percentage at the aerodynamic diameter size range from 2.1 to 3.3 μm for all cases. Regarding total coliforms, the maximum percentage was observed at the aerodynamic diameter size range from 3.3 to 4.7 μm. However, the maximum percentage for heterotrophic bacteria was observed in different size ranges for each case (e.g., 3.3–4.7 μm for AGC, > 7 μm for UB (P1)). These results show that the size distribution profiles of heterotrophic bacteria have differences between each location. The peaks were observed at 3.3–4.7 μm for AGC for both periods. In addition, two peaks (0.65–1.1 μm and > 7 μm) were observed at PST during the P1 period while one peak (> 7 μm) was observed during the P2 period. Regarding UB site, the peak was observed at particles with aerodynamic diameter greater than 7 μm during the P1 period while two peaks were observed during the P2 period. Specifically, the two peaks were observed at 1.1–2.1 μm and at particles with aerodynamic diameter greater than 7 μm in agreement with other observations for airborne terrestrial and marine bacteria (Li et al. 2011; Raisi et al. 2013).

Size distribution (%) of viable, cultivable airborne heterotrophic bacteria, mesophilic fungi, and total coliforms during March to April (P1) and May to June (P2) of 2008 at the a) AGC, b) PST, and c) UB site
Impact of characteristics of exposed subject to the deposited dose and deposition fraction
The impact of characteristics (age, gender, and exertion level) of the exposed subject to the daily deposited dose and deposition fraction in the human respiratory tract was examined. The simulations were implemented for adults and children (15, 10, and 5 years old) at UB site (Fig. 5). The average concentration of mesophilic fungi during P1 period were selected due to the higher value in comparison with the other bioaerosols at UB site. In the simulations for the impact of gender and age in the daily deposited dose, the same activity level (light exercise) for all exposed subjects was used (Fig. 5a). The highest daily deposited dose in the human respiratory tract was obtained for an adult male while the lower was obtained for children (5 years old). Specifically, the daily deposited dose in the human respiratory tract of an adult male was equal to 14,678 CFU/day, while for a 5-year-old child it was equal to 5912 CFU/day. Regarding gender, higher daily deposited dose was observed for males than females. These findings were associated to the higher inhalation rate\((B)\), tidal volume (\({V}_{T})\), and volumetric flow rate of inspired air \((\dot{V})\) of adult male (\(B\)=1.5 m3/h, \({\mathrm{V}}_{\mathrm{T}}\)=1250 ml, \(\dot{V}\)=833 ml/s) in comparison with the other exposed subjects such as adult female (\(B\)=1.25 m3/h, \({V}_{T}\)=992 ml, \(\dot{V}\)=694 ml/s), and 5–15-year-old children (\(B\):0.57–1.38 m3/h,\({V}_{T}\):244–1000 ml,\(\dot{V}\): 317–767 ml/s). The values were adopted from the ICRP. The parameter \(B\) is the most important physiological parameter due to direct impact to the deposited dose rate (see Eq. 2). However, taking into account the body weight of exposed subject for the estimation of the body weight–adjusted dose of adult male and 5-year-old child was observed that the deposited dose were 1.5 times higher per body weight in a 5-year-old child. Furthermore, the deposition fraction in the total human respiratory tract was 5–8% higher in children (5–10 years old) in comparison with adults (male and female). This occurs due to increase deposition in ET region in children (5–10 years old) than adults. Finally, the respiratory tract of children is more vulnerable than adults because is in the growth phase and has not fully development and as well as their immature immune systems and bodies (Bragoszewska et al. 2016).

Daily deposited dose (CFU/day) and deposition fraction of mesophilic fungi at urban background site for a) different characteristics (age (adults and children) and gender) of exposed subject and b) different exertion level of adult male
In addition, the effect of the different activity level to the daily deposited dose in the human respiratory tract was investigated (Fig. 5b). In order to examine the impact of the different activity level of exposed subject in the daily deposited dose, the same age (adult) and gender (male) was used in the simulations. The daily deposited dose in the human respiratory tract of adult male was equal to 4249 CFU/day, 14,678 CFU/day, and 28,062 CFU/day for sitting, light, and heavy exercise, respectively. The daily deposited dose increased when activity level increased due to the higher inhalation rate. Specifically, the inhalation rates of adult male were equal to 0.54, 1.5, and 3.5 m3/h, for sitting, light exercise, and heavy exercise, respectively (ICRP 1994). Therefore, the difference in inhalation rates between sitting and exercise result in different deposited dose. Finally, the same findings apply for each region of the respiratory tract (ET, TB, and AI regions). Regarding the deposition fraction, the light exercise increases the deposition fraction in ET region in comparison with no activity (sitting). In addition, the deposition fraction was lower in the ET region during heavy exercise while the deposition fraction was lower in both TB and AI regions during light exercise. During heavy exercise conditions, the exposed subject breathes through the nose and mouth. Specifically, 50% of airflow passing through nose and 50% through mouth during heavy exercise while during sitting/light exercise 100% of airflow is passing through nose (ICRP 1994). Consequently, the deposition fraction in the ET region during heavy exercise is low (0.36).
Particle mass (PM) and number (PN) concentration and the corresponding daily deposited dose
The dose of particle mass (PM10) and number (PN1) was calculated at the municipal WWTP and UB sites. Τhe daily mass concentrations of the three particles size categories (PM10, PM2.5, and PM1) for the three sampling locations (AGC, PST, and UB) during March to April (P1) and May to June (P2) were presented in Fig. 6a). The highest mass concentrations for all size categories were observed in AGC during the P2 period. Specifically, the concentrations ranged from 75–250 µg/m3, 42–140 µg/m3, and 38–124 µg/m3 for PM10, PM2.5, and PM1, respectively. The AGC is the stage which removes sand, gravel, and other heavy solids from the raw wastewater and results to the emissions of PM during this process. Specifically, the wastewater flow has a spiral pattern at AGC with particles having a density greater than that of surrounding fluid dropping to the bottom while the particles having a density lower remain suspended and then removed (US EPA 2003). The European Union (EU) has established air quality standards for PM for protection of human health. Specifically, the EU air quality standard sets a daily limit for PM10 equal to 50 µg/m3 while for PM2.5 only annual limit (25 μg/m3) value has been set. In the current study, the PM10 concentrations exceeded several times the legislative daily limit of 50 µg/m3. Specifically, the PM10 levels at the AGC exceeded the daily limit (10 out of 11 days) in which corresponds to 91% exceedances. The corresponding values for PST and UB were equal to 2 out of 7 days; 29% of the corresponding sampling days and 3 out of 11 days; 27% of the corresponding sampling days, respectively. However, the PM10 concentrations in the current study were lower in comparison with the study presented by Viegas et al. (2014). Specifically, Viegas et al. (2014) found that the mean PM10 concentrations in two Portuguese wastewater treatment plants (one totally underground with capacity 285,120 m3/day and the other partially underground with capacity 52,500 m3/day) were very high (350 μg/m3 for totally underground and 630 μg/m3 for partially underground). On the contrary, the PM10 levels in a municipal WWTP (with capacity 240,000 m3/day) in North Taiwan (Widiana et al. 2017) were lower in comparison with the current study. Specifically, the mean concentration of PM10 was equal to 28 μg/m3 and 68 μg/m3 during spring and summer, respectively. Regarding PM2.5, Widiana et al. (2017) found that the mean concentration was equal to 5 μg/m3 and 13 μg/m3 during spring and summer, respectively. The values were lower in comparison with the current study. Specifically, in the current study, the PM2.5 concentration was equal to 56 μg/m3 (P1) and 94 μg/m3 (P2) at AGC while at PST was equal to 17 μg/m3 (P1) and 44 μg/m3 (P2). However, both studies found higher concentrations during summer.

a) Daily concentration of the three particles size categories (PM10, PM2.5, and PM1) and b) daily deposited dose of PM10 in the human respiratory tract (ET, TB, and AI regions) at the AGC, PST, and UB site
In addition, Viegas et al. (2014) found the mean concentration of PM2.5 was equal to 69 μg/m3 and 34 μg/m3 for totally and partially underground WWTP, respectively. In the current study, the inflow of wastewater was 18,843 m3/day, and hence was lower in comparison with the corresponding values in the WWTPs in Portugal and Taiwan.
Regarding daily deposited dose of PM10, it was observed higher values for a worker at AGC during the P2 period with median value equal to 3648 μg/day, 183 μg/day, and 436 μg/day for ET, TB, and AI regions, respectively (see Fig. 6b). Therefore, higher deposited dose was occurred in the ET region followed by AI and TB regions. The higher deposition of PM10 in the ET region was in agreement with results from other studies (Manigrasso et al. 2020; Zwozdziak et al. 2017). In the absence of available dose data for workers at WWTPs in the scientific literature, the comparison was performed for workers at UB site. Specifically, a comparison of the deposited dose at the UB site with the background sites from the study of Aleksandropoulou and Lazaridis (2013) was performed. The daily deposited dose of PM10 in the human respiratory tract at UB site ranged from 528 to 1678 μg/day during the P1 period, whereas during the P2 period the daily deposited dose ranged from 741 to 1278 μg/day. In the study of Aleksandropoulou and Lazaridis (2013), the daily deposited dose in the human respiratory tract ranged from 133 to 212 μg/day in a residential background area in northern Europe (Oslo, Norway), while in a coastal remote site (Finokalia, Greece) ranged from 345 to 761 μg/day. Therefore, the daily deposited dose at UB site presented in this study was higher in comparison with the study of Aleksandropoulou and Lazaridis (2013). The UB site presented in this study was a courtyard with small garden, and hence the soil of garden is a significant source of PM10. The contribution (%) of fine (PM2.5) and coarse (PM2.5–10) particles to the PM10 dose is shown in Table 2. Specifically, 73–80% (for P1 period) and 63–84% (for P2 period) of deposited dose of PM10 in the ET region correspond to coarse particles. The opposite characteristic was observed for AI region. Specifically, 80–84% (for P1 period) and 82–95% (for P2 period) of deposited dose of PM10 in the AI region correspond to the fine particles. This finding is linked with the ability of fine particles to penetrate to the deep lung and deposit mainly to the AI region due to diffusion mechanism while coarse particles deposit mainly to the ET region due to impaction mechanism (Darquenne 2020; Hussain et al. 2011).
In addition, the daily deposited dose of PN1 was also estimated. The median concentration of PN1 was equal to 145,334 #/cm3, 5,319#/cm3, and 4539#/cm3 at AGC, PST, and UB site, respectively (Fig. 7a). Elevated number concentration values at a moving bed biofilm reactor (MBBR) at a municipal WWTP located in China were also reported by Yang et al. (2021). Specifically, the concentration at MBBR tank ranged from 71,992 to 87,088 #/cm3 with average value equal to 79,540 #/cm3. The deposited dose of particle number is shown in Fig. 7b). Higher deposited dose was obtained in the AI region compared to the other regions. The median daily deposited dose in the AI region was equal to 2.3 × 1012 #/day, 8.3 × 1010 #/day, and 3.2 × 1010 #/day at AGC, PST, and UB site, respectively. Specifically, the deposited dose was higher in the AI region, followed by TB and ET region. Ultrafine particles deposit mainly in the AI region due of their ability to penetrate deep into the human respiratory tract (Manigrasso et al. 2020). The workers at AGC received the higher deposited dose for both bioaerosols (sum of the three categories of bioaerosols) and airborne particles (PM10 and PN1), and hence the workers at AGC are exposed to higher airborne particles (PM10 and PN1) and bioaerosols in comparison with the workers at PST and UB.

Daily a) number concentration and b) deposited dose of the PN1 at the AGC, PST, and UB site
Hazard quotients
The non-carcinogenic health risk is represented by the hazard quotient HQ. The hazard quotients of bioaerosols and particle mass (PM10 and PM2.5) for adult workers at the three locations (AGC, PST, and UB) are shown in Table 3. The \(\mathrm{HQ}\) of bioaerosols was lower than the limit of 1 in all examined cases except for workers exposure to bacteria at AGC. Therefore, the present results indicate that the non-carcinogenic effects are not of concern and can be ignored for workers at PST and UB, although the non-carcinogenic effects cannot be ignored for workers at AGC. This finding is linked with the inhalation exposure of workers to high concentration of bioaerosols at AGC (pretreatment stage) due of flow of raw wastewater through the AGC. Likewise, Han et al. (2019) and Yang et al. (2019) calculated the HQ of airborne bacteria and fungi for a WWTP located in Beijing (China). Han et al. (2019) found that \(\mathrm{HQ}\) of bacteria and fungi is less than 1 at PST (were not performed measurements at AGC), whereas Yang et al. (2019) found that the \(\mathrm{HQ}\) of bacteria was less than 1 at both AGC and PST suggesting that the inhalation risk for adults were small. In the above studies, the parameters for the calculation of HQ were obtained from the Chinese exposure handbook, while in the current study we have used the default values of US EPA. In the Chinese exposure handbook, the AT was set equal to 26,419 days (72.38 × 365), while in the US EPA approach the AT was set equal to 9125 days (ED × 365) for the calculation of non-carcinogenic risk (HQ). Regarding PM10, the \(\mathrm{HQ}\) for workers at AGC was greater than 1 (Table 3), indicating a risk for human health. This finding is associated with the removal of inorganic solids from the raw wastewater at pretreatment stage which may cause high PM10 levels during the process. Finally, HQ of PM2.5 was greater than 1 for all cases. Higher value was observed for worker at AGC (3.5).
Conclusions
The current study applied the ExDoM2 dosimetry model to predict the deposited dose of bioaerosols (heterotrophic bacteria, mesophilic fungi, and total coliforms) and particle mass (PM10), and number (PN1) received by workers at two locations at the WWTP and one outdoor background location. The calculations with the ExDoM2 dosimetry model were performed for each sampling day. The ExDoM2 dosimetry model estimates the deposited dose for various reference exposed subjects (a reference adult male, adult woman, and various reference ages of children), and hence the model is not applied to a population. Due to the absence of chemical composition profile of the particulate matter, the hazard quotients were calculated using air quality guidelines levels with an RFC of 45 μg/m3 and 15 μg/m3 for PM10 and PM2.5, respectively.
Heterotrophic bacteria and mesophilic fungi were detected at all sampling sites while total coliforms were detected only at AGC. In addition, higher daily deposited dose was observed at AGC for all cases with the exception of mesophilic fungi during the P1 period. Regarding mesophilic fungi during P1 period, the higher daily deposited dose was observed at the UB site and ranged from 4577–27,642 CFU/day. In addition, the daily deposited dose of heterotrophic bacteria for a worker at AGC was higher in comparison with a worker at PST. Therefore, workers at the AGC received much higher daily dose due of higher microbial community of the raw wastewater. On the other hand, the wastewater treatments activities of WWTP decrease the microbial community of the wastewater, and consequently decrease the daily dose received by the workers. Specifically, the daily deposited dose of heterotrophic bacteria for a worker at AGC ranged from 39,243–132,922 CFU/day for P1 period and from 71,480 to 161,663 CFU/day for P2 period, while at PST ranged from 443–1189 CFU/day and 269–1635 CFU/day for P1 and P2 periods, respectively. Finally, total coliforms were detected only at AGC, and hence the primary treatments of WWTP efficiently decreases the concentration of total coliforms. Regarding PM10, the higher daily deposited dose (1146–4076 μg/day (P1) and 1911–6369 μg/day (P2)) received a worker at the AGC. Likewise, the higher daily deposited dose of PN1 received a worker at the ACG (2.0 × 1012–6.2 × 1012 #/day for the whole measurement period. Furthermore, the results showed that the characteristics (age, gender, and activity level) of the exposed subject play significant role in the calculation of the daily deposited dose in the human respiratory tract with higher values, corresponding to adult males and heavy exercise as a direct consequence of the higher inhalation rates. Specifically, the daily deposited dose in the respiratory tract was 19% higher in adult male (14,678 CFU/day) than in adult female (12,353 CFU/day), while taking into account the age of the exposed subject the daily deposited was 8–148% higher in adult male (14,678 CFU/day) than in children (5912–13,540 CFU/day). Regarding activity level, simulations with heavy exercise increased the daily deposited dose in the human respiratory up to 560% in comparison with simulations with no activity level (sitting). Therefore, the difference in inhalation rates between adults and children and as well as between different activity levels result in different total and regional deposited dose.
In addition, an inhalation health risk assessment methodology was applied in the current study. The results showed that the hazard quotient which represents the non-carcinogenic effects due to the inhalation of bioaerosols and PM10 was less than 1 at PST and UB, and hence the non-carcinogenic effects are not significant for the workers. Regarding AGC, the hazard quotient was equal to 4.3, 0.3, and 1.9 for bacteria, mesophilic fungi, and PM10 respectively. Therefore, the non-carcinogenic effects of bacteria and PM10 were considered to be of concern only for the workers at AGC, while for PM2.5 the con-carcinogenic effects were considered to be of concern for all locations. Finally, measures must be implemented to protect of human health such as hygiene measures and personal protective equipment (e.g., mask).
Data availability
The datasets generated during the current study are available from the corresponding author (lazaridi@mred.tuc.gr) on reasonable request.
References
Aleksandropoulou V, Lazaridis M (2013) Development and application of a model (ExDoM) for calculating the respiratory tract dose and retention of particles under variable exposure conditions. Air Qual Atmos Health 6:13–26. https://doi.org/10.1007/s11869-010-0126-z
Benami M, Busgang A, Gillor O, Gross A (2016) Quantification and risks associated with bacterial aerosols near domestic greywater treatment systems. Sci Total Environ 562:344–352. https://doi.org/10.1016/j.scitotenv.2016.03.200
Brown JS (2015) Chapter 27-Deposition of particles. In: Parent JA (ed) Comparative biology of the normal lung, 2nd ed. Academic Press, Cambridge, pp. 513–536. https://doi.org/10.1016/B978-0-12-404577-4.00027-8
Bragoszewska E, Mainka A, Pastuszk J (2016) Bacterial and fungal aerosols in rural nursery schools in Southern Poland. Atmosphere 7:142. https://doi.org/10.3390/atmos7110142
Chalvatzaki E, Lazaridis M (2015) Development and application of a dosimetry model (ExDoM2) for calculating internal dose of specific particle-bound metals in the human body. Inhal Toxicol 27(6):308–320. https://doi.org/10.3109/08958378.2015.1046201
Chalvatzaki E, Chatoutsidou SE, Mammi-Galani E, Almeida SM, Gini MI, Eleftheriadis K, Diapouli E, Lazaridis M (2018) Estimation of the personal deposited dose of particulate matter and particle-bound metals using data from selected European cities. Atmosphere 9(7):248. https://doi.org/10.3390/atmos9070248
Chalvatzaki E, Chatoutsidou SE, Martins V, Faria T, Diapouli E, Manousakas M, AlmeidaSM EK, Lazaridis M (2020) Assessment of the Personal dose received by school children due to PM10 air pollution in Lisbon. Aerosol Air Qual Res 20:1384–1397. https://doi.org/10.4209/aaqr.2020.01.0022
Chalvatzaki E, Chatoutsidou SE, Kopanakis I et al (2021) Personal deposited dose and its influencing factors at several Greek sites: an analysis in respect to seasonal and diurnal variations. Environ Sci Pollut Res 28:29276–29286. https://doi.org/10.1007/s11356-021-12815-y
Cho SH, Seo SC, Schmechel D, Grinshpun S, Reponen T (2005) Aerodynamic characteristic and respiratory deposition of fungal particles. Atmos Environ 39:5454–5465. https://doi.org/10.1016/j.atmosenv.2005.05.042
Darquenne C (2020) Deposition mechanisms. J Aerosol Med Pulm Drug Deliv 33(4):181–185. https://doi.org/10.1089/jamp.2020.29029.cd
Han Y, Yang K, Yang T, Zhang M, Li L (2019) Bioaerosols emission and exposure risk of a wastewater treatment plant with A2O treatment process. Ecotoxicol Environ Saf 169:161–168. https://doi.org/10.1016/j.ecoenv.2018.11.018
Han Y, Li L, Wang Y, Ma J, Li P, Han C, Liu J (2020) Composition, dispersion, and health risks of bioaerosols in waste water treatment plants: a review. Front Environ Sci Eng 15(3):38. https://doi.org/10.1007/s11783-020-1330-1
Hussain M, Madl P, Khan A (2011) Lung deposition predictions of airborne particles and the emergence of contemporary diseases Part-I. Health 2:51–59
ICRP (1994) Human respiratory tract model for radiological protection. ICRP Publication 66. Ann ICRP 24 (1–3). Pergamon Press, Oxford
ICRP (2015) Occupational intakes of radionuclides: Part 1. ICRP Publication 130. Ann ICRP 44(2). SAGE, California
Karra S, Katsivela E (2007) Microorganisms in bioaerosol emissions from wastewater treatment plants during summer at a Mediterranean site. Water Res 41:1355–1365. https://doi.org/10.1016/j.watres.2006.12.014
Katsivela E, Latos E, Raisi L, Aleksandropoulou V, Lazaridis M (2017) Particle size distribution of cultivable airborne microbes and inhalable particulate matter in a wastewater treatment plant facility. Aerobiologia 33:297–314. https://doi.org/10.1007/s10453-016-9470-2
Korzeniewska E (2011) Emission of bacteria and fungi in the air from wastewater treatment plants - a review. Front Biosci 3:393–407. https://doi.org/10.2741/s159
Kowalski M, Wolany J, Pastuszka J, Płaza G, Wlazło A, Ulfig K, Malina A (2017) Characteristics of airborne bacteria and fungi in some Polish wastewater treatment plants. Int J Environ Sci Technol 14:1–12. https://doi.org/10.1007/s13762-017-1314-2
Li M, Qi J, Zhang H, Huang S, Li L, Gao D (2011) Concentration and size distribution in an outdoor environment in the Qingdao coastal region. Sci Total Environ 409:3812–3819. https://doi.org/10.1016/j.scitotenv.2011.06.001
Löndahl J (2014) Physical and biological properties of bioaerosols. In: Jonsson P, Olofsson G, Tjärnhage T (eds) Bioaerosol detection technologies Integrated analytical systems. Springer, New York. https://doi.org/10.1007/978-1-4419-5582-1_3
Lu R, Frederiksen M, Uhrbrand K, Li Y, Østergaard C, Madsen A (2020) Wastewater treatment plant workers’ exposure and methods for risk evaluation of their exposure. Ecotoxicol Environ Saf 205:111365. https://doi.org/10.1016/j.ecoenv.2020.111365
Madhwal S, Prabhu V, Sundriyal S, Shridhar V (2020) Distribution, characterization and health risk assessment of size fractionated bioaerosols at an open landfill site in Dehradun, India. Atmos Poll Res 11:156–169. https://doi.org/10.1016/j.apr.2019.10.002
Ménache MG, Miller FJ, Raabe OG (1995) Particle inhalability curves for humans and small laboratory animals. Ann Occup Hyg 39:317–328. https://doi.org/10.1016/0003-4878(95)00002-V
Nel A, Mädler L, Velegol D et al (2009) Understanding biophysicochemical interactions at the nano–bio interface. Nature Mater 8:543–557. https://doi.org/10.1038/nmat2442
Piqueras P, Li F, Castelluccio V, Matsumoto M, Asa-Awuku A (2016) Real-time ultrafine aerosol measurements from wastewater treatment facilities. Environ Sci Technol 50(20):11137–11144. https://doi.org/10.1021/acs.est.6b02684
Raisi L, Aleksandropoulou V, Lazaridis M, Katsivela E (2013) Size distribution of viable, cultivable airborne microbes and their relationship to particulate matter concentrations and meteorological conditions in a Mediterranean site. Aerobiologia 29(2):233–248. https://doi.org/10.1007/s10453-012-9276-9
Secondo LE, Sagona JA, Calderón L, Wang Z, Plotnik D, Senick J, Sorensen-Allacci M, Wener R, Andrews CJ, Mainelis G (2021) Estimating lung deposition of fungal spores using actual airborne spore concentrations and physiological data. Environ Sci Technol 55(3):1852–1863. https://doi.org/10.1021/acs.est.0c05540
Sturm R (2016) Bioaerosols in the lungs of subjects with different ages-part 1: deposition modelling. Ann Transl Med. 4(11):211. https://doi.org/10.21037/atm.2016.05.62
US EPA (2003) Wastewater technology fact sheet: screening and grit removal. https://www3.epa.gov/npdes/pubs/final_sgrit_removal.pdf Accessed on 26 July 2021
US EPA (2009) Risk assessment guidance for superfund volume I: human health evaluation manual (part F, supplemental guidance for inhalation risk assessment). EPA/ 540/R/070/002. https://www.epa.gov/sites/production/files/2015-09/documents/partf_200901_final.pdf. Accessed 02 September 2021.
US-EPA (2013) Users’ guide and background technical document for USEPA Region 9 – Preliminary Remediation Goals (PRG) Table. https://semspub.epa.gov/work/02/103453.pdf . Accessed 02 september 202.
Viegas C, Faria T, Gomes A, Sabino R, Seco A, Viegas S (2014) Fungal contamination in two Portuguese wastewater treatment plants. J Toxicol Environ Health A 77:90–102. https://doi.org/10.1080/15287394.2014.866925
Widiana D, You SJ, Yang HH, Tsai JH, Wang YF (2017) Source apportionment of air pollution and characteristic of volatile organic compounds in a municipal wastewater treatment plant, North Taiwan. Aerosol Air Qual Res 17:2878–2890. https://doi.org/10.4209/aaqr.2017.09.0317
World Health Organization. (2021). WHO global air quality guidelines: particulate matter (PM2.5 and PM10), ozone, nitrogen dioxide, sulfur dioxide and carbon monoxide. World Health Organization. https://apps.who.int/iris/handle/10665/345329. Accessed on 19 September 2022.
Xu P, Zhang C, Mou X (2020) Bioaerosol in a typical municipal wastewater treatment plant: concentration, size distribution, and health risk assessment. Water Sci Technol 82:1547–1559. https://doi.org/10.2166/wst.2020.416
Yan C, Wang RN, Zhao XY (2021) Emission characteristics of bioaerosol and quantitative microbiological risk assessment for equipping individuals with various personal protective equipment in a WWTP. Chemosphere 265:129117. https://doi.org/10.1016/j.chemosphere.2020.129117
Yang K, Li L, Wang Y, Xue S, Han Y, Liu J (2019) Airborne bacteria in a wastewater treatment plant: emission characterization, source analysis and health risk assessment. Water Res 149:596–606. https://doi.org/10.1016/j.watres.2018.11.027
Yang T, Jiang L, Cheng L, Zheng X, Bi X, Wang X, Zhou X (2021) Characteristics of size-segregated aerosols emitted from an aerobic moving bed biofilm reactor at a full-scale wastewater treatment plant. J Hazard Mater 416:125833. https://doi.org/10.1016/j.jhazmat.2021.125833
Yunesian M, Rostami R, Zarei A, Fazlzadehdavilb M, Janjani H (2019) Exposure to high levels of PM2.5 and PM10 in the metropolis of Tehran and the associated health risks during 2016–2017. Microchemical J 150:104174. https://doi.org/10.1016/j.microc.2019.104174
Zwozdziak A, Gini MI, Samek L, Rogula-Kozlowska W, Sowka I, Eleftheriadis K (2017) Implications of the aerosol size distribution modal structure of trace and major elements on human exposure, inhaled dose and relevance to the PM2.5 and PM10 metrics in a European pollution hotspot urban area. J Aerosol Sci 103:38–52. https://doi.org/10.1016/j.jaerosci.2016.10.004
Funding
Open access funding provided by HEAL-Link Greece
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Consent for publication
All authors consent for the publication of the manuscript and the materials incorporated.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
PM10: particle mass in which 50% of particles have diameter less than 10 μm, PN1: particle number in which 50% of particles have diameter less than 1 μm, PM2.5: particle mass in which 50% of particles have diameter less than 2.5 μm.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chalvatzaki, E., Katsivela, E., Raisi, L. et al. Assessment of personal deposited dose of bioaerosols and particles in a wastewater treatment plant facility. Air Qual Atmos Health 16, 165–181 (2023). https://doi.org/10.1007/s11869-022-01264-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11869-022-01264-2