
Abstract
Ambient fine particulate (PM2.5) pollution threatens public health. Previous studies have primarily focused on PM2.5 estimation, with the quantitative analysis of public exposure and the reason for increased risk receiving limited attention. Quantitative information is essential for environmental risk estimation. Thus, we collected PM2.5 data and population records to illustrate the spatiotemporal patterns of PM2.5 pollution and to quantify public vulnerability and the cause of increased exposure at global, regional, and country scales from 2000 to 2010, following the air quality standards of the World Health Organization. We found that 11.0 × 106 km2 (8%) of the global terrestrial area was exposed to PM2.5 pollution (> 35 μg/m3) in 2010, an addition of 4.3 × 106 km2 since 2000. Furthermore, by 2010, 1.94 billion (30%) people worldwide were exposed to PM2.5 pollution, including 966 and 778 million in Eastern and Southern Asia, respectively, comprising 962 million in China and 543 million in India. After 2000, the vulnerability of 698 million people to PM2.5 pollution increased, including 356 and 280 million in Southern and Eastern Asia, respectively, accounting for 279 million in China and 253 million in India. Moreover, 25% of the global vulnerability increase was from local population growth, and 75% was due to pollution expansion. Specifically, 26 and 16% of the increase in public vulnerability in Southern and Eastern Asia (22 and 16% in India and China), respectively, were from local population growth. We suggest that countries in which migration has contributed to an increase in public vulnerability should balance pollutant emission reduction and migration control to reduce vulnerability. In addition, cooperation between the government and public could help mitigate global pollution as well as environmental and human health risks.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Ambient fine particulate (PM2.5) matter is small in diameter (≤ 2.5 μm) and can be emitted directly or formed secondarily in the atmosphere, thus carrying considerable risk to public health (Brauer et al. 2012; Huang et al. 2014; Lim et al. 2012). Exposure to ambient PM2.5 pollution is associated with an increase in cardiovascular and circulatory diseases, lower respiratory infection, chronic respiratory diseases, and even cancers (Lim et al. 2012; Du and Li 2016). Many high-income countries have established monitoring networks for PM2.5 detection; however, few low- and mid-income countries have created monitoring networks. Those networks have limited spatial distribution, making it difficult to quantitatively illustrate the spatial pattern of PM2.5 concentration at global or regional scales (Han et al. 2014; Deary et al. 2016). Remote sensing estimations of PM2.5 concentrations provide an efficient way to understand public vulnerability to such pollution, because the ground measurements are majorly available at limited urban areas in recent years (van Donkelaar et al. 2010; Boys et al. 2014; van Donkelaar et al. 2015a). Previous research has focused on PM2.5 concentration estimation using remote sensing technology but paid little attention to public exposure analysis (Boys et al. 2014; van Donkelaar et al. 2015a; Han et al. 2015a; Peng et al. 2016). This lack in quantitative estimation of what drives increased exposure has resulted in the belief that increases (or decreases) in exposure are triggered by changes in PM2.5 rather than changes in the population itself (van Donkelaar et al. 2015a). However, quantitative information is important to global regions and countries when estimating environmental risk. Therefore, we collected remote sensing data (van Donkelaar et al. 2015a, b) on PM2.5 concentrations and gridded population records (CIESIN 2005; CIESIN 2005) to illustrate the spatial pattern changes in PM2.5 pollution levels, quantify public vulnerability to PM2.5 pollution, and quantify the contributions of population increase and pollution expansion to increased public vulnerability at global, regional, and country scales from 2000 to 2010, following the air quality standards of the World Health Organization (WHO).
Materials and methods
Materials
The Global Annual PM2.5 Grids dataset represents a series of 3-year running mean grids (1998–2012) of PM2.5 data derived from a combination of MODIS (Moderate Resolution Imaging Spectroradiometer), MISR (Multi-angle Imaging SpectroRadiometer), and SeaWiFS (Sea-Viewing Wide Field-of-View Sensor) Aerosol Optical Depth (AOD) satellite retrievals (van Donkelaar et al. 2015a, b). The dataset showed strong agreement (r = 0.81; slope = 0.68) with ground-based measurements and was thus adopted for global study of PM2.5 concentration dynamics. It was a 3-year running average record to reduce error for each single year. For instance, PM2.5 in 2000 was an average of the PM2.5 in 1999, 2000, and 2001. The dataset have spatial resolution of 0.1 degree (or ~ 10 km). The dataset is available at the Socioeconomic Data and Applications Center (SEDAC) at Columbia University (http://sedac.ciesin.columbia.edu/). We used the global PM2.5 concentration in 2000 and 2010 for this research.
Population records in 2000 were obtained from the Gridded Population of the World Version 3 (GPWv3) (CIESIN 2005) and in 2010 were obtained from the Gridded Population of the World: Future Estimates (GPWFE) (CIESIN 2005). These data are at 2.5 arc-minutes (or ~ 5 km) resolution and therefore could matched the PM2.5 dataset for population exposure analysis. These data were downloaded from SEDAC at Columbia University (http://sedac.ciesin.columbia.edu/).
The United Nations’ global map was used and included global sub-regions and countries (Fig. S1).
Method of data analysis and collection
PM2.5 pollution levels
The World Health Organization (WHO) sets the air quality guideline (AQG) of annual PM2.5 concentration as 10 μg/m3, which is the lowest levels at which total, cardiopulmonary and lung cancer mortalities have been shown to increase with more than 95% confidence in response to long-term exposure to PM2.5. In WHO’s standard, the highest level of annual PM2.5 concentration is 35 μg/m3 (interim target-1 (IT-1)), which is associated with about a 15% higher long-term mortality risk relative to the AQG level (WHO 2005). Because the global PM2.5 concentration has a range of more than 100 μg/m3, which is beyond the AQG of WHO, thus we used the WHO’s IT-1, twofold IT-1 (2IT-1, 70 μg/m3), and threefold IT-1 (3IT-1, 105 μg/m3) as the standards to quantify PM2.5 pollution levels and public vulnerability.
Exposure analysis
Global PM2.5 concentrations and populations were used to calculate the population exposed to PM2.5 pollution (concentration ≥ 35 μg/m3) at the global, global sub-regional, and national levels in 2000 and 2010. Increased population exposure due to local population change was calculated as the population changes in areas in which the PM2.5 concentration was greater than 35 μg/m3 in both 2000 and 2010. Increased population exposure due to PM2.5 pollution expansion was determined in areas in which the PM2.5 concentration was greater than 35 μg/m3 in 2010, but less than 35 μg/m3 in 2000.
Results and discussion
Global average PM2.5 concentration increased from 11.1 μg/m3 in 2000 to 11.8 μg/m3 in 2010. In 2010, 8% of the global terrestrial area (11.0 × 106 km2) was exposed to PM2.5 pollution (> 35 μg/m3) and was mainly located at Eastern Asia (2.7 × 106 km2), Western Africa (2.4 × 106 km2), Western Asia (2.0 × 106 km2), Northern Africa (1.8 × 106 km2), and Southern Asia (1.7 × 106 km2), as well as particularly in Eastern Asia with 0.4 × 106 and 0.6 × 106 km2 exposed to > 3IT-1 and 2IT-1 to 3IT-1, respectively (Fig. 1a; Fig. S2). Among these regions, seven countries with more than 0.5 × 106 km2 exposed to PM2.5 pollution included China (2.7 × 106 km2), Saudi Arabia (1.1 × 106 km2), India (0.8 × 106 km2), Mauritania (0.6 × 106 km2), Niger (0.6 × 106 km2), Mali (0.5 × 106 km2), and Algeria (0.5 × 106 km2). Moreover, 12 countries had more than half of their terrestrial area exposed to PM2.5 pollution, including Bahrain 100%), Kuwait (100%), United Arab Emirates (99%), Qatar (95%), Iraq (88%), Mauritania (84%), Saudi Arabia (72%), Western Sahara (72%), Pakistan (68%), Niger (63%), Mali (54%), and Senegal (51%). Such large areas with high PM2.5 pollution levels represent a significant increase from 2000 to 2010 (Table S1). In addition, an increase of 3.3% of the global terrestrial area (4.3 × 106 km2) was exposed to PM2.5 pollution from 2000 to 2010 (Fig. 1b; Fig. S1). Four regions showed an increase of more than 0.5 × 106 km2: Eastern Asia (1.5 × 106 km2), Western Asia (1.3 × 106 km2), Southern Asia (0.7 × 106 km2), and Northern Africa (0.6 × 106 km2). Among these regions, China saw an increase of 1.5 × 106 km2 and Saudi Arabia an increase of 0.7 × 106 km2 exposed to PM2.5. Moreover, five countries experienced an increase in exposure of more than half of their terrestrial area, including Bahrain (100%), Kuwait (92.5%), United Arab Emirates (82%), Qatar (73%), and Iraq (50%) (Table S2).

Global PM2.5 pollution in 2010 (a) and changes in its distribution from 2000 to 2010 (b)
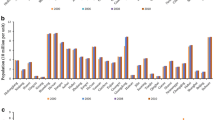
We have found that PM2.5 has potentially influenced the health of global population due to the exposure (Fig. 2; Fig. S3). In 2010, 30% of the global population (1.94 billion) was exposed to PM2.5 pollution, including 62% of people from Eastern Asia (966 million), 47% of people from Southern Asia (778 million), 30% of people from Western Africa (86 million), 28% of people from Western Asia (62 million), and 18% of people from Northern Africa (32 million). We also determined that China (962 million; 72% of its total population), India (543 million; 48% of its total population), Pakistan (153 million; 87% of its total population), Bangladesh (52 million; 31% of its total population), and Nigeria (50 million; 35% of its total population) have 50 million people or more exposed to PM2.5 pollution. The rapid global increase of 698 million people exposed to PM2.5 between 2000 and 2010 has contributed to considerable vulnerability of the public to PM2.5 pollution in 2010 (Fig. S4), including a 356 million increase in Southern Asia, 280 million increase in Eastern Asia, 35 million increase in Western Asia, and 14 million increase in Northern Africa. Moreover, six countries have seen an increase of more than 10 million people between 2000 and 2010, accounting for 93% of the global total increase (650 million), and include China (279 million increase), India (253 million increase), Bangladesh (51 million increase), Pakistan (36 million increase), Iraq (16 million increase), and Saudi Arabia (13 million increase).

Public vulnerability to PM2.5 pollution in 2010
Expansion in PM2.5 pollution is considered the major reason for the substantial increase in public vulnerability. We further analyzed the proportion of increased population exposure due to local population increase and due to PM2.5 pollution expansion. We found that 25% of the increase in global population exposure was due to local population increase, and 75% was due to PM2.5 pollution expansion (Fig. 3a). However, these contributions varied markedly among regions. All increased population exposure in Western Africa was due to local population increase, whereas all increased population exposure in Australia, New Zealand, Central America, Central Asia, Melanesia, Northern America, Northern Europe, South America, Southern Africa, and Southern Europe was due to PM2.5 pollution expansion. Moreover, 88 and 12% of increased population exposure in Middle Africa, 56 and 44% in Western Europe, 52 and 48% in Northern Africa, 26 and 74% in Southern Asia, 26 and 74% in Eastern Africa, 19 and 81% in Western Asia, 16 and 84% in Eastern Asia, 5 and 95% in South-Eastern Asia, 5 and 95% in Eastern Europe, and 4 and 96% in the Caribbean were from local population increase and PM2.5 pollution expansion, respectively. Among these regions (Fig. 3b), the increase in population exposure in seven countries was due to local population increase, including Cameroon, Mali, Mauritania, Nigeria, Senegal, Western Sahara, and Burkina Faso. Furthermore, the increase in public vulnerability in 43 countries was due to local population growth; for example, the 91% (33 million), 22% (55 million), and 16% (43 million) increase in public vulnerability observed in Pakistan, India, and China, respectively. Increased public vulnerability in the remaining countries was due to PM2.5 pollution expansion.

Increased public vulnerability related to local population increase (dark gray bars) and PM2.5 pollution expansion (light gray bars) at global, regional (a), and country (b) scales
Urbanization in developing countries (e.g., China and India) is the major cause of population migrations. Cities, as the major source areas of PM2.5 pollution in many developing counties, are the destination of most domestic migrants (Han et al. 2015a, b; Cohen 2006). Thus, rapid and unplanned urbanization in developing countries can increase population exposure to PM2.5 pollution and contribute considerably to the burden of health expenditure (Gong et al. 2012). Some large developing countries (e.g., China) are now attempting to undertake rapid urbanization with strong attention to environmental protection. However, China still suffers from heavy PM2.5 pollution due to its previous rapid development in which economic growth was the focus (Han et al. 2015c; Bai et al. 2014). Thus, we suggest that countries in which migration contributes to a relatively large proportion of increased public vulnerability should balance pollutant emission reduction and migration control to reduce vulnerability and exposure (e.g., countries listed in Fig. 3).
Both the government and the public in developing countries suffering significant PM2.5 pollution should pay more attention to environmental protection as well as the intensive human activities (e.g., urbanization, industrialization) that will take place over the next decades. Control of and reduction in air pollution emissions in Eastern China and Northern India, where pollution is highly attributed to increasing human activities, and ecological protection in areas such as Northern Africa and the Middle East, where pollution is highly attributed to natural emissions, which must be taken into consideration and action. Mass population migration from no or low pollution areas to heavy pollution areas should be discouraged or controlled until the risk declines to reduce both health hazard and health expenditure. Cooperation between the government and public could go a long way to ensure an environmentally sustainable and ecological civilization.
Conclusions
Ambient fine particulate pollution threatens public health. Previous research has focused on PM2.5 estimation, with limited attention given to the quantitative analysis of public exposure or reasons for the increased risk. Such quantitative information is essential for environmental risk estimation. We collected PM2.5 data and population records to illustrate the spatiotemporal patterns of PM2.5 pollution and to quantify public vulnerability and the causes of increased vulnerability at the global, regional, and country scales from 2000 to 2010.
-
1)
Global small areas exposed to PM2.5 pollution but with large portion of global population. We found that 11.0 × 106 km2 (8%) of global terrestrial area was exposed to PM2.5 pollution (> 35 μg/m3) in 2010, an addition of 4.3 × 106 km2 since 2000. In 2010, 1.94 billion (30%) people worldwide were exposed to PM2.5 pollution, including 966 and 778 million in Eastern and Southern Asia, respectively, accounting for 962 million in China and 543 million in India. After 2000, 698 million more people were vulnerable to exposure, including 356 and 280 million in Southern and Eastern Asia, respectively, consisting of 279 million in China and 253 million in India.
-
2)
Population increase contributing a meaningful amount to the global population exposure to PM2.5 pollution. Twenty-five percent of the increase in global vulnerability was from local population increase, where 75% was due to pollution expansion. In Southern and Eastern Asia, 26 and 16% of the increase in public vulnerability (22 and 16% in India and China) were from local population growth. Thus, countries in which migration has contributed to an increase in public vulnerability should balance pollutant emission reduction and migration control to reduce public vulnerability. Furthermore, strong cooperation between the government and public could help mitigate pollution and its associated environmental and human health risks.
References
Bai X, Shi P, Liu Y (2014) Realizing China’s urban dream. Nature 509:158–160
Boys B, Martin R, van Donkelaar A, MacDonell R, Hsu N, Cooper M, Yantosca R, Lu Z, Streets D, Zhang Q, Wang S (2014) Fifteen-year global time series of satellite-derived fine particulate matter. Environ. Sci. Technol. 48:1109–11118
Brauer M, Amann M, Burnett R, Cohen A, Dentener F, Ezzati M, Henderson S, Krzyzanowski M, Martin R, Dingenen R, van Donkelaar A, Thurston G (2012) Exposure assessment for estimation of the global burden of disease attributable to outdoor air pollution. Environ Sci Technol 46:652–660
Center for International Earth Science Information Network—CIESIN—Columbia University, and Centro Internacional de Agricultura Tropical—CIAT (2005) Gridded Population of the World, Version 3 (GPWv3): population density grid. Palisades, NY: NASA Socioeconomic Data and Applications Center (SEDAC). doi:10.7927/H4XK8CG2. Accessed 28 May 2015a
Center for International Earth Science Information Network—CIESIN—Columbia University, United Nations Food and Agriculture Programme—FAO, and Centro Internacional de Agricultura Tropical—CIAT (2005) Gridded Population of the World, Version 3 (GPWv3): population count grid, future estimates. Palisades, NY: NASA Socioeconomic Data and Applications Center (SEDAC). doi:10.7927/H42B8VZZ. Accessed 28 May 2015b
Cohen B (2006) Urbanization in developing countries: current trends, future projections, and key challenges for sustainability. Technol Soc 28:63–80
Deary M, Bainbridge S, Kerr A, McAllister A, Shrimpton T (2016) Practicalities of mapping PM10 and PM2.5 concentrations on city-wide scales using a portable particulate monitor. Air Quality, Atmosphere & Health 9:923–930
Du Y, Li T (2016) Assessment of health-based economic costs linked to fine particulate (PM2.5) pollution: a case study of haze during January 2013 in Beijing, China. Air Quality, Atmosphere & Health 9:439–445
Gong P, Liang S, Carlton E, Jiang Q, Wu J, Wang L, Remais J (2012) Urbanization and health in China. Lancet 379:843–851
Han L, Zhou W, Li W, Li L (2014) Impact of urbanization level on urban air quality: a case of fine particles (PM2.5) in Chinese cities. Environ Pollut 194:163–170
Han L, Zhou W, Steward P, Li W, Li L (2015a) An optimum city size? The scaling relationship for urban population and fine particulate (PM2.5) concentration. Environ Pollut. doi:10.1016/j.envpol.2015.08.039
Han L, Zhou W, Li W (2015b) City as a major source areas of fine particulate in China. Environ Pollut 206:183–187
Han L, Zhou W, Li W (2015c) Increasing impact of urban fine particles (PM2.5) on areas surrounding Chinese cities. Sci Rep 5:12467
Huang R, Zhang Y, Bozzetti C, Ho K, Cao J, Han Y, Daellenbach K, Slowik J, Platt S, Canonaco F et al (2014) High secondary aerosol contribution to particulate pollution during haze events in China. Nature 514:218–222
Lim S, Vos T, Flaxman A, Danaei G, Shibuya K, Adair-Rohani H, AlMazroa M, Amann M, Anderson H, Andrews K et al (2012) A comparative risk assessment of burden of disease and injury attributable to 67 risk factor s and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the global burden of disease study 2010. Lancet 380:2224–2260
Peng J, Chen S, Lv H, Liu Y, Wu J (2016) Spatiotemporal pattern of remotely sensed PM2.5 concentration in China from 1999 to 2011. Remote Sens Environ 174:109–121
van Donkelaar A, Martin R, Brauer M, Kahn R, Levy R, Verduzco C, Villeneuve P (2010) Global estimates of ambient fine particulate matter concentrations from satellite-based aerosol optical depth: development and application. Environ Health Perspect 118:847–855
van Donkelaar A, Martin R, Brauer M, Boys B (2015a) Use of satellite observations for long-term exposure assessment of global concentrations of fine particulate matter. Environ Health Perspect 123:135–143
van Donkelaar A, Martin RV, Brauer M, Boys BL (2015b) Global annual PM2.5 grids from MODIS, MISR and SeaWiFS Aerosol Optical Depth (AOD), 1998–2012. Palisades, NY: NASA Socioeconomic Data and Applications Center (SEDAC). doi:10.7927/H4028PFS. Accessed 28 May 2015b
World Health Organization (2005) Air quality guidelines for particulate matter, ozone, nitrogen dioxide and sulfur dioxide. Available at: http://www.who.int/phe/health_topics/outdoorair/outdoorair_aqg/en/
Funding information
This research was supported by the National Natural Science Foundation of China (NSFC41590841). In addition, the research received financial support from the National Key Research and Development Program (Grant No. 2016YFC0503004), Ministry of Science and Technology of the People’s Republic of China. Moreover, the research received financial support from the Frontier Science Research Project of Chinese Academy of Sciences (QYZDB-SSW-DQC034-2), the Hundred Talents Program of Chinese Academy of Science, and the Science and Technology Service Network Initiative Project of the Chinese Academy of Sciences (KFJ-EW-ZY-004).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Han, L., Zhou, W., Li, W. et al. Global population exposed to fine particulate pollution by population increase and pollution expansion. Air Qual Atmos Health 10, 1221–1226 (2017). https://doi.org/10.1007/s11869-017-0506-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11869-017-0506-8