
Abstract
Air quality indices (AQI) are commonly used to indicate the level of severity of air pollution to the public. A number of methods were developed in the past by various researchers/environmental agencies for the calculation of AQI, but there is no universally accepted method, appropriate for all situations. An updated review of the major air quality indices developed worldwide is presented in this paper. These methods differentiate mainly in the number of pollutants included, its sampling period and air quality classes and breakpoints. When applying different AQI to a common case study, important differences are found in terms of the classification of the quality of the air. The purposes of this research are to identify weaknesses of the current AQI and to discuss possible changes and updates with Portugal as case study. A survey, with 10 questions about the calculation and use of the AQI and its dissemination to public, was delivered to the five regional environmental agencies in Portugal and, based on results, modifications to the current AQI are proposed. Two main changes—inclusion of PM2.5 and specific urban/industrial AQI—were tested, comparing the current and the proposed AQI along the 2014 year. It is observed that a significant difference exists when specific urban and industrial sites are considered when calculating the AQI. On the other hand, and contrarily to other regional studies, the results show that the inclusion of fine suspended particulate (PM2.5) does not impact the final AQI value.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Air pollution is a global environmental problem that influences mostly the health of urban population, and repeated exposures to ambient air pollutants over a prolonged period of time increases the risk of being susceptible to airborne diseases such as cardiovascular and respiratory diseases and lung cancer (WHO, 2009).
An air quality index (AQI) can be defined as a communication tool and a standardized summary measure of ambient air quality used to express the level of health risk related to particulate and gaseous air pollution (Kowalska et al, 2009), describing the air quality in a simple and understandable way. These indicators give the public an opportunity to track the state of their local, regional and national air quality without the need for an understanding of the details of the data upon which they are based. The primary objective, from a public health point of view, is to provide to the public information that enables people to take appropriate actions to protect themselves from adverse health effects of air pollution. A secondary objective is to increase awareness of the effects attributable to air pollution at current levels of exposure, motivating changes in both individual behaviour and public policy (Doan and East, 1977; Stieb et al. 2005). Although the AQI itself is simply a number that reflects some aspect(s) of air quality, in practice, it is associated with colour schemes, graphics, air quality category labels such as “good”, “moderate” or “poor”, and various messages. These describe the expected effects at various levels of the index, and what people can do to reduce the risk of these effects, in many cases identifying specific population subgroups expected to be at greater risk. These generally include children, the elderly, those who are active outdoors and individuals with heart or lung disease.
An AQI is generally based upon a combination of several sub-indices for individual pollutants. Major pollutants usually considered are O3, NOx, SO2, CO and suspended particulates and oxidants. Such a combined index is suitable for the description of the ambient air conditions in large urban centres, where these specific pollutants are being continuously monitored. Each pollutant sub-index relates the measured levels of the pollutant to the objectives or standards set by the governmental authorities. A number of characteristics seem desirable for an index: consistency, simplicity (readily understandable by the public), versatility (inclusive of major pollutants and their synergies) and flexibility (to allow for pollutants to be added/subtracted as changes to their health impact are revealed and comparable among communities) (Hewings, 2001).
Public health agencies have increasingly called into question the validity of the conventional AQI. The primary criticism is that the status quo AQI does not accurately reflect our current understanding of the adverse health effects of ambient air pollution, particularly the occurrence of effects at low levels of exposure, and the additive contribution of multiple pollutants (Pyta, 2008; Shooter and Brimblecombe, 2009, Robichaud et al., 2016, Fann et al., 2016). It was stated by the World Health Organization (WHO, 2005) that in the case of PM10, PM2.5 and O3, there are no concentrations below which the risk of adverse health effect is zero, which also refers to SO2 and NO2. In fact, much progress is still to be made, mainly through more careful consideration of the combined impact of multiple pollutants, of low level exposure, and more timely transfer of usable information to the public.
Furthermore, the WHO (2006) recommends that governments should consider their own local circumstances carefully, with specificities of places taken into account, when formulating policy targets, namely AQI. Nowadays, there are many air quality indices in use in the world, all different in concept and presentation, which makes difficult the comparison of air quality between cities and regions (Elshout et al., 2008; Kanchan et al., 2015). The need for a uniform air quality index has been discussed at the European Union level, but it has been exceptionally difficult to create a uniformly accepted and publicly accessible index of air quality. Some authors (e.g. Longhurst, 2005; Kanchan et al. 2015) suggest that a universal technique to calculate the air quality index is not very much helpful since the sensitivity of the people to air pollution changes with changing in geographical location, quality of life, etc. They defend that it is infeasible and perhaps impossible to formulate a universal technique for determining one air quality index that considers all pollutants and that is appropriate for all situations. According to the recent review made by Mandal and Gorai (2014) every index should have its own characteristic strengths and weaknesses that affect its suitability to particular applications.
Taking into consideration that the development of an adequate tool to understand pollution levels in an area is of utmost importance (Kyrkilis et al. 2007), the main purpose of this paper is to understand the current AQI used in Portugal and to propose improvements based on other practices in the world. Changes to the current AQI are suggested and tested in this work.
The air quality index over the world
A variety of indices has been, and still is, developed in an attempt to meet the public’s needs for information on air quality. Different breakpoint concentration values and air quality standards are used and reported in the literature (WHO, 2005; Ruggieri and Plaia, 2012). Different areas of the world are characterized by different climatic conditions influencing the effect of atmospheric pollutants on human health and also the response of the population to air pollution could be different. Therefore, it could not be realistic to assume the same AQI as valid all over the world.
In 1976, the USEPA established a Pollutant Standards Index (PSI) that rated air quality from 0 to 500, with 100 equal to the National Ambient Air Quality Standards (NAAQS) (Cheng et al, 2007). The PSI is calculated for every pollutant with a NAAQS (CO, NO2, O3, PM10 and SO2), but the only level reported for a given time and location is for the pollutant most exceeding its standard. The overall range is subdivided into six ranges to which six categories of air quality correspond. For each pollutant, the breakpoint concentrations, corresponding to each category, are not on a linear scale. Breakpoint concentrations have been defined by the USEPA on the basis of NAAQS and on the results of epidemiological studies of the effect of single pollutants on human health. In 1999, the PSI was revised and renamed, by the USEPA (Cheng et al., 2007), as the air quality index (AQI). The new system includes a new sub-index for fine particulate matter (PM2.5). Based on the USEPA’s philosophy for the AQI, similar indices are widely in use worldwide (Kyrkilis et al., 2007). For instance, this AQI is applied in Taiwan, which experiences significant air pollution problems (Fang and Chen, 1996), and where the inclusion of PM2.5 led to three times higher frequency of occurrence of days with AQI higher than 100 (Liu, 2002). In Brunei, Radojevic and Hassan (1999) found that this AQI may not be suitable for haze coming from forest fires, as it does not take into account short-term exposure to extremely high particle concentrations of up to 1 mg m−3. Cheng et al. (2004) proposed a revised USEPA air quality index (RAQI) by introducing an entropy function to include the effect of the concentrations of the rest of pollutants other than the pollutant with maximum AQI, but this was not implemented yet.
In the European member countries, the same approach is used with slight changes among the different member states, with distinct breakpoints even all based on the limit values established by the European Directive 2008/50/EC on ambient air quality. In 2005, the Common Air Quality Index (CAQI) was proposed, in the framework of the CITEAIR project (co-funded by the INTERREG programme in Europe), to facilitate the comparison of air quality in European cities in real-time (Elshout et al., 2008, 2014; www.airqualitynow.eu). An important feature of this index system is that it differentiates between traffic and city background conditions. It has also five levels and the final index is the highest value of the sub-indices for each component (pollutant). The choice of the classes for the CAQI is still inspired by the EC legislation. The CAQI also does not take into account the adverse effects due to the coexistence of all pollutants. CAQI is used by several air quality communication initiatives such as the obsAIRve project (www.obsairve.eu) and some software applications (e.g. obsAIRve, Air Quality in Europe,WorldAQI, and Airparif).
An Air Quality Health Index (AQHI) was developed in Canada to understand the state of local air quality with respect to public health. The scientific basis for the formulation of the AQHI is based on the epidemiological research undertaken at Health Canada (Stieb et al., 2008). A similar approach was used to construct the AQI in Cape Town, using the relative risk factors of daily mortality attributed to the increase in the concentration of main pollutants by 10 μg m−3 (Cairncros et al. 2007). In an attempt to compare and summarize compiled country-based (or administrative-based) AQI, Table 1 identifies the main differences among several indices.
The majority of the countries adopted the AQI defined by the USEPA or are based on it. Only a few number of countries or administrative regions (Canada, Hong Kong and Gibraltar) adopted the “Health AQI”. The main differences are related to the number and type of pollutants included, considering (or not) additive effects, the sampling period (related to level of exposure) and the setting of the threshold values. Besides that, for Australia and India, other factors are included, related to specific pollution sources: the case of the fires in Australia (visibility is included in the AQI estimation) and the chemical industry and agriculture in India (NH3 and Pb are also considered for the calculation of AQI).
Aiming to better understand the different indices in terms of adopted air quality classes and concentration breakpoints, a comparative compilation of AQI classes has been done, for several institutional AQI. Figure 1 shows this analysis for PM10, PM2.5, O3, NO2, and SO2, for a number of countries with available (official) information. A reclassification to five classes was necessary in some cases (countries) to harmonize this comparison.

AQI classes comparison regarding a PM10 daily average, b PM2.5 daily average, c NO2 daily maximum, d CO 8-h running average daily maximum, e O3 8-h running average daily maximum, f O3 daily maximum, g SO2 daily average and h SO2 daily maximum
The less demanding breakpoints (higher concentration values) are defined for the USA, China and India, regarding all the analysed pollutants. In average, these breakpoints are two times higher than in European countries (three times higher for PM10). Over Europe, there are small differences between the standards/breakpoints defined. Nevertheless, Germany adopts more strict (low concentration) values when compared to other European countries.
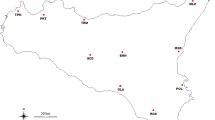
In order to better illustrate these differences, distinct AQI were calculated for the same day (15 December 2015) over Portugal, using observations from all background monitoring stations located in each Portuguese zone/agglomeration (www.qualar.org). The results obtained are shown in Fig. 2, considering the AQI of Portugal, the USA, China and Germany.

AQI for Portugal on 15 December 2015 calculated according to the methodology defined for: Portugal, the USA, China and Germany
According to what was already expected, there are large differences when different AQI are applied over Portugal. When AQI from the USA and China are used, the calculated AQI indicates “very good” (light green) air quality over Portugal. The same dataset corresponds to “medium” (and “bad” for Lisbon area) air quality when the Portuguese AQI is used and “bad” to “very bad” with the German one.
In addition to institutional approaches there are some AQI specifically developed for cities and urban areas. Cannistraro and Ponterio (2009) created the Pollution Index (PI) to report air quality status in the city of Naples, Italy. It is based on the weighted mean value of the sub-indices of the considered pollutants and additive effects of air pollutants have also been considered. Additive effects of air pollutants, taking into account the combined effects of all pollutants to human health, have been studied by Murena (2004) too. Kyrkilis et al. (2007) proposed an aggregate AQI, based on the combined effects of five main pollutants, covered by the European standards, and applied it to assess the air quality at each monitoring station located in the whole area of Athens, Greece. Sicard et al. (2011) designed the Aggregate Risk Index (ARI) for assessing the health impact due to air pollution in the south-east of France, following the methodology proposed by Cairncros et al. (2007). The ARI is based on the exposure response relationship and relative risk of the well-established increased daily mortality, enabling an assessment of additive effects of short-term exposure to the major air pollutants. The index is defined to reflect the contribution of individual pollutants to total risk, based on functions and values published by the WHO (2001, 2004, 2008), Katsouyanni (2006) and InVS (2008). An integrated AQI, called the Air Quality Risk Index, which considers environmental conditions, and economic losses involved, was applied to the city of Tehran as a megacity (Ahmadi et al., 2015). The results indicated that this index can be applied to define the actual conditions of urban air quality and to achieve sustainability and resiliency.
A revised AQI
In Portugal, the AQI is operationally calculated each day by the Portuguese Agency for the Environment, taking into account the measured concentrations of NO2, SO2, O3, CO and PM10 in the background monitoring stations of the country. The concentration classes adopted for each pollutant are summarized in Table 2. The highest individual pollutant index determines the final AQI of the location/zone or agglomeration.
Based on the current practices and on regional stakeholder opinion, an improved AQI is proposed for Portugal.
Questionnaire to the air quality regional administrations
In order to understand and identify the main weaknesses of the current AQI, we surveyed the five regional administrative agencies in Portugal responsible for the air quality monitoring and management with a list of ten questions regarding the use and calculation of the AQI and its public dissemination. The questions delivered in this survey are reported in Table 3 and the answers compiled in Fig. 3.

Results of the survey for each question
In general, there is consensus only regarding the AQI classes based on legislated limit values (and not on WHO recommendations) and the need of developing a software application (“app”) to disseminate this index information. For the remaining questions, a majority agreement (more than 60 %) exists, with the exception of the question about the inclusion of long-term effects, with “no answer” as the larger reply.
Some of the queries reveal that no change is needed: number of classes (5); breakpoints defined according to the legislation; and classification referring to “good-bad” air quality. However, some changes are required too, in agreement with the guidelines for AQI harmonization recently delivered by the DG Environment (EEA, 2015), namely inclusion of PM2.5 and natural events, AQI with information related to each pollutant, developing specific AQI for traffic/industrial areas and inclusion of modelling data in case of absence of monitoring data. Based on this survey results, a revised AQI can be proposed.
AQI proposal
Although a revised AQI can be proposed, the impacts of its implementation are not known yet. Both the inclusion of natural events and air quality modelling values (in case of no monitoring data available) can be particularly easy to implement for Portugal, because there are modelling data, including mineral dust, accessible in forecast mode: http://previsao-qar.web.ua.pt (Monteiro et al., 2005). In this case, the AQI could be (re-)calculated using these prognostic modelling data, which is already planned for the near future.
The other two recommendations derived from the survey results—inclusion of PM2.5 in the calculation of the index and specific AQI for urban/industrial areas—were tested for the metropolitan area of Lisbon (AML, which is divided in two agglomerations: AML North and AML South). The impact of these two changes on the AQI value was studied for a period of 1 year (2014).
The results, in terms of the differences found between the current and revised index, are shown in Fig. 4. For the inclusion of PM2.5 in the AQI calculation, the Spanish breakpoints were adopted (Fig. 1b). The inclusion of traffic and industrial stations was investigated considering all the monitoring stations available in the AML North (four traffic stations; Fig. 4a) and AML South (three industrial stations; Fig. 4b), respectively. The inclusion of PM2.5 in the AQI calculation was assessed using all the monitoring stations measuring this pollutant in AML North (total of three; Fig. 4c) and South (total of two; Fig. 4d).

Top: comparison of the AQI calculated when all monitoring stations are included (a), and only the traffic and industrial stations (b) are considered. Bottom: comparison of the AQI calculated when PM2.5 are included, or not, for AML North (c) and AML South (d)
This analysis demonstrates the sensitivity of the AQI outcome to the type of stations included in its calculation. Regarding the inclusion, or not, of traffic environments, there is a slight deterioration of the AQI when the index is calculated including all stations instead of only the background (<10 % total days) and even higher when only traffic stations are considered. Nevertheless, traffic environments exhibit higher number of days with AQI “very good”, which is explained by the absence of O3 monitoring in these sites (the presence of high O3 concentration in background sites is responsible for lower AQI). About the industrial site inclusion, a decline of AQI is observed for the major part of the days: lower number of days with “good” AQI and higher “medium” and “poor” AQI is verified when considering only the industrial sites. However, for the “very good” range there is a higher number of days exhibiting it for industrial sites, which is explained by the low NO2 concentration values when compared to the background urban sites.
Regarding the inclusion of PM2.5 on the AQI calculation, no changes in the AQI class distribution were found for both agglomerations. The same conclusion was observed when this comparative exercise was extended to other monitoring stations over Portugal. But the same was not experienced by other countries (Cheng et al., 2007; Elshout et al., 2014), which can be explained by the dominance of the coarse fraction of PM10 over Portugal (Monteiro et al., 2015). Nevertheless, the inclusion of PM2.5 will assure that the AQI describes more effectively the exposure of citizens comparing with the original index.
Discussion and conclusions
This work contributes to a proposal of an improved AQI to be used in Portugal. The compilation of the current air quality indices shows a lack of a common strategy, which makes it difficult to compare the state of the air within different regions and cities. The major differences among the indices are found in the aggregation function, type and number of pollutants, number of index classes and associated thresholds. It is also observed that when applying the AQI to a common air quality data set (for Portugal), large differences in the index value and responsible pollutant are calculated. In general there is a deterioration of the air quality (given by the index) from the USA/China to Europe, but even between European countries, differences are found, with Germany showing more demanding standards.
A survey with main ten questions was delivered to the five regional administrative agencies in Portugal responsible for the air quality monitoring, and the main weaknesses of the current AQI were identified regarding its use and calculation and its dissemination for the public. This survey results identified several changes to promote a more complete and correct index information, namely the inclusion of PM2.5, specific standards and index for specific polluted areas (traffic, industrial) and the inclusion of natural events information and modelling data when no monitoring data are available. The two first changes on AQI were evaluated using 1 year of monitoring data over Portugal. According to the results it is important to develop specific AQI representative of traffic and industrial areas, supplying the public with a better indicator of the air quality over these areas. Regarding the inclusion of PM2.5, no impact was found on the AQI value, which indicates that PM10 is enough to assemble the aerosol pollution.
This case study confirms the inherent complexity and, at the same time, need of creating accessible, understandable, and efficient indices for air quality. Future work will involve the study and analysis of other important factors like long-term effects of pollutants, the availability of health descriptors and their purpose or applicability.
References
Ahmadi A, Abbaspour M, Arjmandi R, Abedi Z (2015) Air quality risk index (AQRI) and its application for a megacity. Int J Environ Sci Technol 12(12):3773–3780
Cairncros EK, John J, Zunckel M (2007) A novel air pollution index based on the relative risk of daily mortality associated with short-term exposure to common air pollutants. Atmos Environ 41:8442–8454
Cannistraro G, Ponterio L (2009) Analysis of air quality in the outdoor environment of the city of Messina by an application of the pollution index method. Int J Civ Environ Eng 1:4
Cheng WL, Kuo YC, Lin PL, Chang KH, Chen YS, Lin TM, Huang R (2004) Revised air quality index derived from an entropy function. Atmos Environ 38:383–391
Cheng W-L, Chen Y-S, Zhang J et al (2007) Comparison of the revised air quality index with the PSI and AQI indices. Sci Total Environ 382(2-3):191–198
Doan MH, East C (1977) Proposed air-quality index for urban areas. Water Air Soil Pollut 8(4):441–451
Elshout S, Léger K, Nussio F (2008) Comparing urban air quality in Europe in real time, a review of existing air quality indices and the proposal of a common alternative. Environ Int 34(5):720–726
Elshout S, Léger K, Heich H (2014) CAQI common air quality index—update with PM2.5 and sensitivity analysis. Sci Total Environ 488–489:461–468
EEA (Environmental European Agency) (2015) Minutes of the 20th EIONET Workshop on Air Quality Assessment and Management. Ljubljana, Slovenia, 5–6 October. Available at: http://acm.eionet.europa.eu/docs/meetings/151005_eionet_aq_ws/wrap-up_20eionet_aq_ws_06.10.2015.pdf. Accessed Mar 2016.
Fang S, Chen H (1996) Air quality and pollution control in Taiwan. Atmos Environ 30(5):735–741
Fann N, Wesson K, Hubbell B (2016) Characterizing the confluence of air pollution risks in the United States. Air Qual Atmosphere Health 9(3):293–301
Hewings J (2001) Air quality indices: a review., Pollution A report prepared for Environment Canada by Pollution Probe, Available at: http://www.bvsde.paho.org/bvsacd/cd32/airq.pdf
InVS (2008) Programme de surveillance air et santé (PSAS). Analyse des liens à court terme entre pollution atmosphérique urbaine et mortalité dans neuf villes françaises. InVS, Paris, p 41
Kanchan K, Kumar A, Gorai P (2015) A review on air quality indexing system. Asian J Atmos Environ 9–2:101–113
Katsouyanni K (2006) APHEA project: air pollution and health: a European approach. Epidemiology 17(6):S19, ISEE/ISEA 2006 Conference Abstracts Supplement
Kowalska M, Osrodka L, Klejnowski K, Zejda JE, Krajny E, Wojtylak M (2009) Air quality index and its significance in environmental health risk communication. Arc Environ Prot 35(1):13–21, ISSN: 0324-8461
Kyrkilis G, Chaloulakou A, Kassomenos PA (2007) Development of an aggregate air quality index for an urban Mediterranean agglomeration: relation to potential health effects. Environ Int 33(5):670–676
Liu CM (2002) Effect of PM2.5 on AQI in Taiwan. Environ Model Softw 17:29–37
Longhurst J (2005) 1 to 100: creating an air quality index in Pittsburgh. Environ Monit Assess 106(1-3):27–42
Mandal TK, Gorai AK (2014) Air quality indices: a literature review. J Environ Sci Eng 56(3):357–362
Monteiro A, Vautard R, Lopes M, Miranda AI, Borrego C (2005) Air pollution forecast in Portugal: a demand from the new air quality framework directive. Int J Environ Pollut 25(2):4–15
Monteiro A, Fernandes AP, Gama C, Borrego C, Tchepel O (2015) Assessing the mineral dust from North Africa over Portugal region. Atmos Pollut Res 6:70–81
Murena F (2004) Measuring air quality over large urban areas: development and application of an air pollution index at the urban area of Naples. Atmos Environ 38:6195–6202
Pyta H (2008) Classification of air quality based on factors of relative risk of mortality increase. Environ Prot Eng 34:111–117
Radojevic M, Hassan H (1999) Air quality in Brunei Darussalam during the 1998 haze episode. Atmos Environ 33(22):3651–3658
Robichaud A, Ménard R, Zaïtseva Y, Anselmo D (2016) Multi-pollutant surface objective analyses and mapping of air quality health index over North America. Air Qual Atmosphere Health. doi:10.1007/s11869-015-0385-9, in press
Ruggieri M, Plaia A (2012) An aggregate AQI: comparing different standardizations and introducing a variability index. Sci Total Environ 420:263–272
Shooter D, Brimblecombe P (2009) Air quality indexing. Int J Environ Pollut 36(1-3):305–323
Sicard P, Lesne O, Alexandre N, Mangin A, Collomp R (2011) Air quality trends and potential health effects—development of an aggregate risk index. Atmos Environ 45:1145–1153
Stieb DM, Doiron MS, Blagden P et al (2005) Estimating the public health burden attributable to air pollution: an illustration using the development of an alternative air quality index. J Toxicol Environ Health Part A 68(13-14):1275–1288
Stieb DM, Burnett RT, Smith-Doiron M, Brion O, Shin HH, Economou V (2008) A new multi-pollutant, no-threshold air quality health index based on short-term associations observed in daily time-series analyses. J Air Waste Manage Assoc 58:435–450
WHO (2001) Health impact assessment of air pollution in the WHO European region. WHO/Euro product n 876(03):01(50263446)
WHO (2004) Meta-analysis of time-series studies and panel studies of particulate matter (PM) and ozone (O3). WHO task group. WHO/EURO 04/5042688
WHO (2005) Air quality guidelines for particulate matter, ozone, nitrogen dioxide and sulfur dioxide: global update 2005. Summary of risk assessment. World Health Organization, Geneva
WHO (2006) Preventing disease through healthy environments-towards an estimate of the environmental burden of disease. / Prüss-Üstün A, & Corvalán C. ISBN 92 4 159382 2
WHO (2008) Health risks of ozone from long-range trans boundary air pollution, ISBN 978 92 890 42895 WHO/Euro product
WHO (2009) Global health risks: mortality and burden of diseases attributable to selected major risks. World Health Organization, Geneva, Available online at http://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdf
Acknowledgments
The authors wish to thank the Portuguese Agency for the Environment and the Regional Coordination and Development Commission (CCDRs) for their support. Also, the authors would like to acknowledge the financial support of FEDER through the COMPETE Programme and the national funds from FCT–Science and Technology Portuguese Foundation for the Ph.D. grant of C. Gama (SFRH/BD/87468/2012). Thanks are also due for the financial support to CESAM (UID/AMB/50017), to FCT/MEC through national funds, and the co-funding by the FEDER, within the PT2020 Partnership Agreement and Compete 2020.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Monteiro, A., Vieira, M., Gama, C. et al. Towards an improved air quality index. Air Qual Atmos Health 10, 447–455 (2017). https://doi.org/10.1007/s11869-016-0435-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11869-016-0435-y