
Abstract
Particulate matter less than 2.5 μm in diameter (PM2.5) is associated with asthma morbidity. Recent studies have begun examining the role of various constituents of PM2.5, their potential sources, and their effects on health. We examine their role in asthmatic children. Thirty-six children 6–14 years with moderate/severe asthma from inner city areas in New York City were studied for 2-week periods (summer and winter) using diaries and lung function. Outdoor data, including PM10, PM2.5, elements, elemental/organic carbon, and criteria gases (NO2, SO2, and O3) were collected at two sites. Odds ratios (ORs) relating daily pollutant concentrations to asthma indicators were calculated. During summer significant ORs>1 for symptom severity were obtained (O3, PM10, PM2.5, and S); after adjustment for O3, the ORs were no longer significant. During winter, Cu, Fe, Si, and Zn were significantly but negatively (ORs<1) associated with symptoms. Lag effects in winter suggested delayed effects (ORs>1) on symptoms (As, K, Pb, and V). Albuterol use increased during summer (O3, PM10, PM2.5, Na, and S); after adjustment for O3, only Na and S remained significant. Reduced pulmonary function was significantly associated with O3 and Cl. Components of PM2.5 are associated with asthma exacerbation in asthmatic children. Same-day pollutant associations with symptoms are seen in summer. In winter, our analysis suggests delayed adverse associations of PM2.5 components.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Asthma is the most important chronic disease in children in the US affecting over 5 million children aged 5 to 17 years, accounting for nearly 15 million school absence days, morbidity, and nearly 2 billion dollars in economic impact (Wang et al. 2005). Air pollution in general—and particulate matter (PM) specifically—is recognized as an important contributor to exacerbations of asthma (Gielen et al. 1997; Peters et al. 1997; Vedal et al. 1998; Selgrade et al. 2006; Larsen et al. 2002; Iskandar et al. 2012; Roy et al. 2011). Children are thought to be particularly susceptible due to their smaller lung volumes and unique features of their immune, endocrine, and nervous systems (Selgrade et al. 2006).
Many studies relate time series investigations of PM and other pollutants to asthma endpoints such as unscheduled physician visits (Sinclair et al. 2010), emergency department visits (Peel et al. 2005; Strickland et al. 2014), and hospital admissions (Malig and Ostro 2009). However, there are relatively few panel studies of asthmatic children and the effects of air pollution (Li et al. 2012) and fewer still that specifically examine PM compositional associations (Delfino et al. 2008, 2003; Gent et al. 2003; Zora et al. 2013). Fine particulate matter (PM2.5) is a heterogeneous mixture of compounds originating from many sources (Larsen et al. 2002; Iskandar et al. 2012; Roy et al. 2011; Selgrade et al. 2006; Tzivian 2011), and it is unlikely that all PM components—including both organic and inorganic species—play equal roles in asthma exacerbation. It has been suggested that our understanding of the effects of individual sources on asthma would benefit from additional compositional studies since those might be avoided, modified, or treated prophylactically if exposure were unavoidable (Larsen et al. 2002; Selgrade et al. 2006; Tzivian 2011).
The Children’s Air Pollution Asthma Study investigated the associations of PM2.5 and its elemental and carbonaceous composition on a panel of inner city asthmatic children studied prospectively. We hypothesized that individual PM components, related to different source processes such as primary combustion or secondary photochemistry, would have differential associations with indicators of asthma exacerbation. Furthermore, due to seasonal differences in time–activity patterns and concentrations, examining these PM component associations by season would reveal varying patterns and help to better characterize the role of sources on indices of asthma severity.
Subjects and methods
Overall study design
The study was performed during the summer and winter of 2008 and 2009. Each household was monitored for two 14-day periods, in each season. Thirty-six children with moderate to severe asthma living in East Harlem and the South Bronx were recruited over a 2-year period. These areas were selected because of high asthma prevalence (NYC Department of Health and mental Hygiene 2008). Participants were recruited from the Mount Sinai Hospital Emergency Department (ED) and Outpatient Asthma Clinics (OAC). Recruitment was performed by two bilingual research assistants and a pediatric pulmonary fellow who identified potential subjects in the ED and the OAC, immediately before and during the study periods. Subjects were screened for willingness to participate and entry/exclusion criteria. Of the 43 subjects screened, 39 were eligible and 36 completed at least one season’s measurements. Thirty-two subjects completed both seasons. Our original intent was to study the participants in clearly defined winter and summer seasons, defined in the standard manner: Winter (December 21 to March 21) and Summer (June 21 to September 21); however, the study periods extended into fall and spring in a few subjects.
During each season, outdoor air quality was continuously monitored starting 7 days before the first subject was tested. For each subject beginning on day 1, parents and children recorded pulmonary function twice daily (am and pm), as well as daily symptom scores and other outcome measures. On day 7, homes were revisited, equipment and diaries were checked, and subjects re-instructed. On day 15, the health outcome data were reviewed and collected, and equipment retrieved.
Subjects
Subject demographics are listed in Table 1.
Inclusion criteria
Children aged 6–14 years old with moderate to severe asthma living in the studied areas were recruited. Asthma was diagnosed based on the Guidelines for the Diagnosis and Management of Asthma NAEPP Expert Panel Report (2007). Medical records and patient histories were reviewed at the time of the recruitment in the ED or OAC, and in particular, frequency of bronchodilator use and the use of inhaled corticosteroids were used to assess asthma severity.
Exclusion criteria
We excluded children with active disease other than asthma such as hematologic, endocrine, or cardiac conditions requiring daily medications; families planning to move from their current home within the next 6 months; and families that had members who smoked at home.
Baseline visit
A baseline visit was conducted, during which the objectives and requirements were explained to the child’s primary caretaker and the child. A Mount Sinai Institutional Review Board approved consent (IRB Project 05-0679), and HIPAA form was read and signed by the parent.
A respiratory history and asthma questionnaire, based on an National Health Institutes questionnaire previously used in the Inner City Asthma Study (Kattan et al. 2006), was administered. Trained bilingual (Spanish/English) interviewers performed baseline clinical interviews with the child's primary caretaker that included information about demographics, asthma morbidity, characteristics of the home environment, and the child's exposure to environmental tobacco smoke. A physical examination was performed by the study physicians.
In order to determine the allergic status of our subjects, skin prick testing was conducted with 12 standard antigens and two controls administered with multi-test equipment (Alk-Abello, Horsholm, Denmark) (see Table 1).
Three reproducible spirometric tests meeting ATS criteria (Wanger et al. 2005) were administered using the ML 3500 spirometer (Micro Medical, Lewiston, Me). The spirometer was calibrated daily and before each patient test with a 3-L syringe. Results were expressed as their value in liters or liters per second and as a percent of predicted based on predicted values obtained from NHANES III (children 8–14 years) and Wang et al. (children less than 8 years) (Hankinson et al. 1999; Wang et al. 1993).
Morbidity assessment
A daily symptom diary (cough and wheeze) with each symptom graded on a scale of 0–3 (none = 0, mild = 1, moderate = 2, severe = 3), medication use (albuterol puffs per day), and activity measures were recorded by parent and child. These diaries and the questions were explained to parent and child, and the understanding of the questionnaire was reviewed at the weekly visit. Unscheduled clinic or ER visits and hospitalizations were also recorded. Daily total symptom scores were obtained by adding the severity scores of both cough and wheeze. Average values for daily symptom scores and albuterol usage are shown in Table 1.
Pulmonary function
Baseline measurements in the clinic included forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), and peak expiratory flow (PEF). Two daily lung function measurements, using a Piko 1 handheld spirometer (nSpire Health Inc. Longmont, CO), were conducted at the subject’s home, with PEF and FEV1 measured morning and evening. Parent and child were instructed in the use of the Piko spirometer at baseline, and technique was reevaluated at the weekly visit. Data were downloaded to our database directly from the spirometer. Percent daily lability in PEF and FEV1 were measured by dividing the absolute value of the difference between AM and PM values by the AM value 100 × [(|AM−PM|)/AM]. Severity of obstruction was characterized by FEV1 and PEF (as a percent predicted) as follows—80 %–100 %, mild; 50 %–80 %, moderate; 30 %–50 %, severe; <30 %, very severe). These measurements take into account age and height in that they were expressed as a percent of predicted. Baseline measurements were performed at least 8 h after any bronchodilator treatment had been administered.
Outdoor exposures (Table 2)
Outdoor air pollution measurements were obtained from two monitoring sites: City College of New York (CCNY) in Northern Manhattan as the primary site and Middle School 302 (MS302, previously IS-52), a New York State Department of Environmental Conservation (NYSDEC) site as the secondary site in the South Bronx.
Daily PM2.5 samples were collected at the CCNY site using modified Harvard impactors equipped with ChemComb inlets. Particle samples were collected on Teflon (16.7 LPM) and pre-fired quartz filters (10 LPM). Sequential sampling was performed using an eight-channel programmable controller (Control model XT-W8). This instrument was programmed to start a new 24-h sample every morning at 9:00 AM.
Teflon filters were analyzed gravimetrically for mass. Black carbon was measured by optical reflectance using a smokestain reflectometer (EEL Model 43D). X-ray fluorescence was performed to determine PM2.5 elemental composition. Pre-fired quartz filters were analyzed for total elemental carbon (EC) and organic carbon (OC) using the Thermal Optical Reflectance IMPROVE protocol.
Since gaseous pollutants were not available at the CCNY site (except for O3), additional data were obtained from MS-302 from the Aerometric Information Retrieval System database. Parameters included hourly ozone (O3), sulfur dioxide (SO2), nitrogen dioxide (NO2), and daily PM10 mass. Daily averages were calculated from the hourly data.
On average, residences were located 3.0 (range, 0.8–6 km) and 3.9 (range, 2–5.4 km) away from the primary CCNY and secondary MS-302 monitoring sites, respectively (see Table 1). Ozone measurements at both sites were highly correlated (r[winter] = 0.9698; r[summer] = 0.9675; r[both] = 0.9727).
Weather data and influenza prevalence
Weather data for New York City, including average daily temperature, wind speed, and precipitation, were obtained from the New York Central Park Tower meteorology station of the National Climatic Data Center. Relative humidity (RH) was obtained from the NYSDEC, New York Botanical Gardens site (see Table 2).
Weekly data on influenza prevalence in New York State were obtained from the Weekly Influenza Activity Report. New York State Department of Health, Bureau of Communicable Disease Control Regional Epidemiology Program (2008, 2009).
Data analysis statistical methods
Regression models for longitudinal data with ordinal outcomes using a cumulative logit link function were employed to relate daily outdoor pollutant concentrations to the following daily health outcomes of severity: (1) total asthma symptom scores; (2) number of albuterol puffs; and (3) degree of obstruction (as defined in the sections on morbidity assessments and pulmonary function). These regression models provide estimates of odds ratios (OR), with corresponding 95 % confidence intervals and p values. All models were adjusted for Hispanic ethnicity, gender, daily ambient maximum relative humidity, and average temperature. The statistical analysis using the SAS GLIMMIX procedure allows for missing data. The average percent of missing symptom data in winter was 4.8 % and in summer, 2 %.
Each pollutant was scaled using units of its interquartile range (IQR) for the purposes of these comparisons (Delfino et al. 2003). Relationships between weather parameters and pollutant levels were examined using correlation coefficients. We investigated the pollutant associations for time lags of up to 7 days. All ORs were calculated after adjusting for gender, Hispanic ethnicity, daily ambient maximum relative humidity, and daily average temperature. We also calculated ORs with and without adjustment for ozone. Forest plots were generated summarizing the results of the time-lag analyses. All statistical analyses were performed using SAS version 9.2.
Results
Exposure assessment
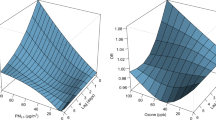
A summary of exposure measurements is shown in Table 2. Mean PM2.5 in summer was 12.4 μg/m3, with major components being OC (2.2 μg/m3), EC (1.2 μg/m3), and sulfate (3.5 μg/m3, calculated from elemental sulfur). Winter PM2.5 mass was slightly lower at 12.2 μg/m3. Organic carbon and sulfate were lower in the winter as expected, due to less photochemical activity, while EC was slightly higher. The highest elemental concentrations in summer were for Na, Fe, Ca, and K; these same elements also predominated in the winter. Na, Cl, Ni, and V were all increased in winter compared with summer, reflecting de-icing activities, marine aerosol, and heating oil combustion. Criteria gases showed expected patterns, with higher ozone in the summer and higher NO2 in the winter. Figure 1 shows a scatter plot of PM2.5 and O3 measurements by season. In summer, O3 and PM2.5 levels correlate positively (r = 0.62; p < 0.0001) while in winter the correlation is negative (r = –0.38; p < 0.0001).

Scatter plot of PM2.5 versus O3 by season
Asthma symptoms (same-day analysis)
We analyzed the ORs for the likelihood of increased asthma symptoms per IQR of outdoor pollutants measured over a 24-h period (Table 3).
In summer, more severe symptoms were significantly associated with O3, PM2.5, PM10, and sulfur (S). However, when these analyses were controlled for ozone (which exhibited the largest OR (1.95) in summer), there was a modest decrease in the ORs, resulting in a loss of significance for these pollutants.
In winter, no significant ORs>1 were observed for any pollutant; however, significant ORs<1 were found for Cu, Fe, Si, and Zn. After adjustment for ozone, significant ORs<1 associations with symptoms persisted for Cu, Fe, Si, and Zn, but also became significant for Ca and Ti (Table 3).
Other environmental risk factors
Because of the ORs<1 associations of PM2.5 components with symptom severity in winter, we examined other known risk factors which might explain this paradoxical association. We evaluated average daily temperature, relative humidity, and wind speed in relation to PM components (Table 4 and Electronic supplementary material (ESM) Table 1). In winter, strong negative correlations were noted between wind speed and PM10, PM2.5, and its various elemental components. NO2 and SO2 were also negatively correlated with wind speed. In contrast, O3 was positively correlated with wind speed. In summer, negative correlations with wind speed were consistently present but generally had lower correlation coefficients than in winter, suggesting less influence of these factors on pollutants during summer.
The ORs for these and other risk factors potentially influencing respiratory symptoms are listed in Table 5. Of note is the strong association of flu prevalence as well as early versus late winter months with asthma symptoms.
Table 6 indicates that, when the model adjusts for Hispanic ethnicity, gender, daily ambient maximum relative humidity, and average temperature, Wind Speed increase, Precipitation, Missed School versus Not Missed, Flu Rate Greater than Zero versus Flu Rate Zero and Early Winter Months versus Late Winter Months, the significant ORs<1 persist only for Fe and Cu; the other components lose significance. This suggests that the additional risk factors co-vary with the pollutants in such a way as to reduce their negative (ORs<1) association.
Lag effects (days −1 to −7).
In each season, a unique pattern of change in the ORs over the lag period was observed for most pollutants. In summer, the ORs for the associations of many of the pollutants were >1 on the day of the measurement decreasing to less than 1 the greater the lag, with most becoming significantly <1. This finding was most pronounced with lag days 3, 4, and 5. In winter, the pattern generally showed ORs<1 on the day of the measurement becoming >1 with increasing lag, usually maximum on days 3, 4, and 5 (Fig. 2; ESM Table 2 and ESM Figure 1a, b). Several PM2.5 components (As, K, Pb, and V) were associated with significant ORs>1 lag effects on symptoms in winter.

Forest plots of pollutants demonstrating significant delayed adverse symptom effects in winter. Seven-day lags are illustrated for Summer and Winter. All ORs were adjusted for gender, Hispanic ethnicity, daily ambient maximum relative humidity, average temperature, and ozone
Albuterol use
The ORs for using more albuterol on the same day by pollutant are shown in Table 7 (lags see ESM Table 3). In summer, significant ORs>1 were observed for same day O3, PM10, PM2.5, Na, and S. After adjusting for O3, ORs remained significant for PM2.5, Na, and S. No significant associations were observed during the winter months for any of the pollutants, with or without ozone adjustment.
Pulmonary function
The odds ratios of experiencing lower lung function (AM FEV1 percent of predicted) by pollutant IQR (lag 0) are shown in Table 8. Only same-day O3 in the summertime showed ORs>1 with lung function. Cl was significantly associated (ORs<1) with FEV1. In addition, we examined FEV1 and PEF; both expressed as a percent of predicted and daily lability of PEF and FEV1. The analysis did not show consistent lag effects of the examined pollutants on lung function variables (see ESM Table 4).
Discussion
Fine particulate matter (PM2.5) is increasingly recognized as a major risk factor for health effects, including cardiovascular and respiratory diseases. Children with asthma are a particularly vulnerable group. PM2.5 is a heterogeneous mixture of organic and inorganic components of many origins. To date, only a few panel studies such as Gent et al. (2009), Delfino et al. (2003, 2008), and Zora et al. (2013) have examined these components in relation to effects in well-defined panels of asthmatic children.
In our prospective study of children with moderate to severe asthma, we found that, in summer, PM2.5 and several of its elemental components were associated with asthma severity, but the effect was modulated by ozone concentrations.
In winter, similar associations (ORs>1) were noted for PM2.5, but these occurred several days after the PM2.5 measurement. In summer, there were also delayed significant associations, but they appeared to be primarily with ORs<1.
Components of PM2.5 and their potential sources
Specific PM2.5 components are related to primary emission sources such as coal- and oil-fired power plants, traffic, as well as industrial operations (Andersen et al. 2007; Dominici et al. 2006; Peltier et al. 2009; Vedal et al. 1994; Zhou et al. 2011) and secondary sources. We did not note significant ORs>1 for same-day associations in summer between symptoms and any pollutant after adjusting for ozone; in the unadjusted models, S was associated with increased symptoms. S and Na were significantly associated with increased albuterol use in both unadjusted and adjusted models. It is important to note that, without transport or meteorological studies—which were beyond the scope of this study—we are only able to point out general sources of PM components and cannot conclusively associate components with specific sources.
However, these overall findings compare favorably with an analysis we reported separately (Rohr et al. 2014) in which we applied source apportionment modeling to the same dataset. In that work, we found that cough and wheeze symptoms were most strongly associated with regional and salt factors; the regional factor was heavily loaded with S, and the salt factor with Na.
Sulfur is present primarily in the form of ammonium sulfate ([NH4]2SO4), a secondary pollutant formed through the oxidation of sulfur dioxide (SO2). Important sources of SO2 are coal-fired power plants and smelting operations (Ramadan et al. 2000).
A small fraction of S in the form of primary metal sulfates is emitted from smelters or from local sources burning residual oil (Ramadan et al. 2000). Sulfur dioxide is also present in mobile source emissions, especially diesel exhaust (Huffman et al. 2000). Sulfur in the Northeastern US is most commonly associated with regional sources, especially during the summer (Herndon et al. 2005), although local sources can play a role in urban or industrialized areas.
Na is generally considered to be a marker of marine aerosols (Penttinen et al. 2006; Thurston et al. 2005), although it has also been associated with waste incineration (Moffet et al. 2008). In winter, road dust contains Na associated with road salt as a de-icing agent. The associations with Na may have been due to its correlation with other PM components. For example, air masses of marine origin could have traveled over sources emitting other pollutants before reaching our study site.
In winter, delayed effects with significant ORs>1 were seen for V, Pb, K, and As. Vanadium has been associated with combustion of heating fuels (Lim et al. 2011; Roemer et al. 2000) and ship traffic (Peltier and Lippmann 2010) Pb is associated with industrial sources and leaded aviation fuels (Miranda et al. 2011; Taylor et al. 2013); K is associated with biomass burning (e.g., wood burning or forest fires) (Delfino et al. 2003), and As is associated with industrial sources and the burning of coal and other fuels (Lim et al. 2011). Marginally significant delayed ORs>1 for Al, Ca, NO2, SO2, S, and Zn were also noted (see ESM Figure 1a and b and Table 2). Most of these elements have been associated with road dust. SO2 and NO2 were also noted to be marginally significant and are associated with combustion sources.
Modulating effects of other environmental factors
Li et al. (2012), in a recent review of the effects of air pollution in panels of asthmatic children, point out that interactions with temperature and the effects of lag are generally lacking in panel investigations.
The fact that adjustment for ozone in summer decreased the magnitude of the ORs and removed their significance in some cases suggests that O3 accounted for some of the effect attributed to PM. This notion is supported by the positive correlation between PM2.5 and O3 in summer (Fig. 1). Similar findings have been reported by Thurston et al. (1997), who note the important role of O3 in summer, as well as by Gent et al. (2003) and Samoli et al. (2011).
In winter, we observed a number of significantly OR<1 for the same-day associations particularly with the elements Ca, Cu, Fe, Si, Ti, and Zn. Only the associations (OR<1) of Cu and Fe persisted when other risk factors including O3, weather, and influenza prevalence were adjusted for. Dales et al. (1996), in particular, note a large increase in asthma hospital admissions beginning in the fall, with much of this increase being due to respiratory infections. Additional explanation may come from the fact that, in winter, asthmatic children spend more time indoors, particularly on days when pollution is greater and adverse weather conditions present.
Our results differ in some cases from other studies that examined respiratory endpoints and, in some cases, are similar. For example, Gent et al. (2003) observed same-day associations for EC, Zn, Cu, Si, Al, Ca, Ti, and K whereas our same day associations were limited to PM2.5, PM10, and S, and the latter lost significance when adjusted for O3.
Symptoms in Patel’s study (2009), an investigation of the effects of PM2.5 components in a general pediatric population, were significantly associated with Ni, V, and EC. They suggested that exposure to particle metals and EC from heating oil and traffic sources were associated with respiratory symptoms in young children. Our study did not find associations with Ni or EC but did find a possible delayed association with V. Interestingly, the Patel study (2009) identified same-day associations between Zn and cough in the cold and flu season which we also observed in the winter. Hirshon et al. (2008), by contrast, found an association of asthma admissions with previous day Zn levels.
The role of a lag effect.
In winter, we found ORs>1 associations between symptoms and lagged PM2.5 components, with the strongest associations observed on lag days 3, 4, and 5 (see Fig. 2 and ESM Figure 1a, b). The S-shaped patterns in the odds ratio suggest a progressive development of these associations with increasing lag times. Similar findings for PM have been described by several authors (Kim et al. 2012; Lipsett et al. 1997; Mar et al. 2010; Rodriguez et al. 2007). This might be explained by a delayed inflammatory effect of outdoor PM2.5 components on airways in this season.
Gent et al. (2009) found delayed effects on symptoms for Si, Ca, K, Pb, Al, and V, consistent with our findings in winter; however, we did not find associations with EC, Cu, or Fe as in that study. Gent’s lag data were limited to the 2 days preceding the exposure day, and the study did not distinguish seasonal associations.
Kim et al. (2012) studied temporal lag patterns of the associations of PM2.5 constituent concentrations by disease category on hospital admissions in Denver. Relative risk for admission was generally larger at longer lags for respiratory disease and asthma, in particular, consistent with our findings in winter.
The lag associations (ORs<1) seen in summer are difficult to explain. As in winter, relationships between PM2.5, its components, and other risk factors varying over time might serve to explain these associations. Alternatively, one might postulate that high concentrations of summer pollutants could induce airway tolerance, rendering the child less susceptible to symptoms. A similar effect is described in Byssinosis (Bakirci et al. 2007).
Albuterol use and lung function
The absence of an association between albuterol use and same-day pollutant levels in winter is supported by the observation of ORs<1 for symptoms.
The overall lack of predictive power of pulmonary function in judging morbidity has previously been noted (Mortimer et al. 2001). In this study, peak flow monitoring in asthmatic children and, in particular, daytime lability did not have additive predictive value for health effects beyond that obtained from symptom reports.
Multiple testing
Multiple tests increase the likelihood that some of the significant associations found in this study have occurred by chance. However, the pattern observed in our forest plot presentation of lag and results of two-pollutant models suggest consistent associations over many pollutants. This should be borne in mind when interpreting our findings.
Conclusions
We found that PM2.5 and its components are associated with severity of asthma symptoms and the use of rescue medications in this panel of moderate to severe asthmatic children residing in areas of high asthma prevalence. In addition to O3, we noted significant associations (ORs>1) with S and Na in summertime. In winter, we observed delayed (ORs>1) associations between symptoms and As, Pb, K, and V. It is difficult to associate components with a single, specific source; nonetheless, previous transport studies and our own source apportionment analyses (Rohr et al. 2014) have associated these components with combustion activities such as coal burning, diesel or residual fuel use, and/or regional transportation of such pollutants in marine air masses. We also documented interesting associations (ORs<1), both for same-day and lagged pollutants which require further investigation, especially given that subjects are exposed to mixtures of correlated multiple pollutants.
References
Andersen ZJ, Wahlin P, Raaschou-Nielsen O, Scheike T, Loft S (2007) Ambient particle source apportionment and daily hospital admissions among children and elderly in Copenhagen. J Expo Sci Environ Epidemiol 17:625–636
Bakirci N, Kalaca S, Francis H, Fletcher AM, Pickering CA, Tumerdem N et al (2007) Natural history and risk factors of early respiratory responses to exposure to cotton dust in newly exposed workers. J Occup Environ Med 49:853–861
Dales RE, Schweitzer I, Toogood JH, Drouin M, Yang JW, Dolovich J et al (1996) Respiratory infections and the autumn increase in asthma morbidity. Eur Respir J 9:72–77
Delfino RJ, Gong H Jr, Linn WS, Pellizzari ED, Hu Y (2003) Asthma symptoms in Hispanic children and daily ambient exposures to toxic and criteria air pollutants. Environ Health Perspect 111:647–656
Delfino RJ, Staimer N, Tjoa T, Gillen D, Kleinman MT, Sioutas C et al (2008) Personal and ambient air pollution exposures and lung function decrements in children with asthma. Environ Health Perspect 116:550–558
Dominici F, Peng RD, Bell ML, Pham L, McDermott A, Zeger SL et al (2006) Fine particulate air pollution and hospital admission for cardiovascular and respiratory disease. JAMA 295:1127–1134
Gent JF, Triche EW, Holford TR, Belanger K, Bracken MB, Leaderer BP (2003) Association of low-level ozone and fine particles with respiratory symptoms in children with asthma. JAMA 290:1859–1867
Gent JF, Koutrakis P, Belanger K, Triche E, Holford TR, Bracken MB et al (2009) Symptoms and medication use in children with asthma and traffic-related sources of fine particle pollution. Environ Health Perspect 117:1168–1174
Gielen MH, Van Der Zee SC, Van Wijnen JH, Van Steen C, Brunekeef B (1997) Acute effects of summer air pollution on respiratory health of asthmatic children. Am J Respir Crit Care Med 155:2105–2108
Hankinson JL, Odencrantz JR, Fedan KB (1999) Spirometric reference values from a sample of the general U.S. population. Am J Respir Crit Care Med 159:179–187
Herndon SC, Shorter JH, Zahniser MS, Wormhoudt J, Nelson DD, Demerjian KL et al (2005) Real-time measurements of SO2, H2CO, and CH4 emissions from in-use curbside passenger buses in New York City using a chase vehicle. Environ Sci Technol 39:7984–7990
Hirshon JM, Shardell M, Alles S, Powell JL, Squibb K, Ondov J et al (2008) Elevated ambient air zinc increases pediatric asthma morbidity. Environ Health Perspect 116:826–831
Huffman GP, Huggins FE, Shah N, Huggins R, Linak WP, Miller CA et al (2000) Characterization of fine particulate matter produced by combustion of residual fuel oil. J Air Waste Manag Assoc 50:1106–1114
Iskandar A, Andersen ZJ, Bønnelykke K, Ellermann T, Andersen KK, Bisgaard H (2012) Coarse and fine particles but not ultrafine particles in urban air trigger hospital admission for asthma in children. Thorax 67:252–257
Kattan M, Crain EF, Steinbach S, Visness CM, Walter M, Stout JW et al (2006) A randomized clinical trial of clinician feedback to improve quality of care for inner-city children with asthma. Pediatrics 117:1095–1103
Kim SY, Peel JL, Hannigan MP, Dutton SJ, Sheppard L, Clark ML et al (2012) The temporal lag structure of short-term associations of fine particulate matter chemical constituents and cardiovascular and respiratory hospitalizations. Environ Health Perspect 120:1094–1099
Larsen GL, Beskid C, Shirnamé-Moré L (2002) Environmental air toxics: role in asthma occurrence? Environ Health Perspect 110(Suppl 4):501–504
Li S, William G, Jalaludin B, Baker P (2012) Panel studies of air pollution on children’s lung function and respiratory symptoms: a literature review. J Asthma 49:895–910
Lim JM, Jeong JH, Lee JH, Moon JH, Chung YS, Kim KH (2011) The analysis of PM2.5 and associated elements and their indoor/outdoor pollution status in an urban area. Indoor Air 21:145–155
Lipsett M, Hurley S, Ostro B (1997) Air pollution and emergency room visits for asthma in Santa Clara County, California. Environ Health Perspect 105:216–222
Malig BJ, Ostro BD (2009) Coarse particles and mortality: evidence from a multi-city study in California. Occup Environ Med 6:832–839
Mar TF, Koenig JQ, Primomo J (2010) Associations between asthma emergency visits and particulate matter sources, including diesel emissions from stationary generators in Tacoma, Washington. Inhal Toxicol 22:445–448
Miranda ML, Anthopolos R, Hastings D (2011) A geospatial analysis of the effects of aviation gasoline on childhood blood lead levels. Environ Health Perspect 119:1513–1516
Moffet RC, Desyaterik Y, Hopkins RJ, Tivanski AV, Gilles MK, Wang Y et al (2008) Characterization of aerosols containing Zn, Pb, and Cl from an industrial region of Mexico City. Environ Sci Technol 42:7091–7097
Mortimer KM, Redline S, Kattan M, Wright EC, Kercsmar CM (2001) Are peak flow and symptom measures good predictors of asthma hospitalizations and unscheduled visits? Pediatr Pulmonol 31:190–197
New York State Department of Health Bureau of Communicable Disease Control. Regional Epidemiology Program (2008) Weekly influenza activity report. (The report with this information was last revised on January, 2015). http://www.health.ny.gov/diseases/communicable/influenza
NIH National Asthma Education and Prevention Program. Expert panel report 3. Guidelines for the diagnosis and management of asthma. NIH Publication Number 08-5846. October 2007 http://www.nhlbi.nih.gov/guidelines/asthma/asthsumm.pdf
Patel MM, Hoepner L, Garfinkel R, Chillrud S, Reyes A, Quinn JW et al (2009) Ambient metals, elemental carbon, and Wheeze and cough in New York City children through 24 months of age. Am J Respir Crit Care Med 180:1107–1113
Peel JL, Tolbert PE, Klein M, Metzger KB, Flanders WD, Todd K, Mulholland JA, Ryan PB, Frumkin H (2005) Ambient air pollution and respiratory emergency department visits. Epidemiology 16:164–174
Peltier RE, Lippmann M (2010) Residual oil combustion: 2. Distributions of airborne nickel and vanadium). J Expo Sci Environ Epidemiol 20:342–350
Peltier RE, Hsu SI, Lall R, Lippmann M (2009) Residual oil combustion: a major source of airborne nickel in New York City. J Expo Sci Environ Epidemiol 19:603–612
Penttinen P, Vallius M, Tiittanen P, Ruuskanen J, Pekkanen J (2006) Source-specific fine particles in urban air and respiratory function among adult asthmatics. Inhal Toxicol 18:191–198
Peters A, Dockery DW, Heinrich J, Wichmann HE (1997) Short-term effects of particulate air pollution on respiratory morbidity in asthmatic children. Eur Respir J 10:872–879
Ramadan Z, Song XH, Hopke PK (2000) Identification of sources of Phoenix aerosol by positive matrix factorization. J Air Waste Manag Assoc 50:1308–1320
Rodriguez C, Tonkin R, Heyworth J, Kusel M, De Klerk N, Sly PD et al (2007) The relationship between outdoor air quality and respiratory symptoms in young children. Int J Environ Health Res 17:351–360
Roemer W, Hoek G, Brunekreef B, Clench-Aas J, Forsberg B, Pekkanen J et al (2000) PM10 elemental composition and acute respiratory health effects in European children (PEACE project). Pollution effects on asthmatic children in Europe. Eur Respir J 15:553–559
Rohr A, Habre R, Godbold J, Moshier E, Schachter N, Kattan N, Grunin A, Nath A, Coull B, Koutrakis P (2014) Asthma exacerbation is associated with particulate matter source factors in New York City. Air Qual Atmos Health 7:239–250
Roy A, Sheffield P, Wong K, Trasande L (2011) The effects of outdoor air pollutants on the costs of pediatric asthma hospitalizations in the United States, 1999 to 2007. Med Care 49:810–817
Samoli E, Nastos PT, Paliatsos AG, Katsouyanni K, Priftis KN (2011) Acute effects of air pollution on pediatric asthma exacerbation: evidence of association and effect modification. Environ Res 111:418–424
Selgrade MK, Lemanske RF Jr, Gilmour MI, Neas LM, Ward MD, Henneberger PK et al (2006) Induction of asthma and the environment: what we know and need to know. Environ Health Perspect 114:615–619
Sinclair AH, Edgerton ES, Wyzga R, Tolsma D (2010) A two-time-period comparison of the effects of ambient air pollution on outpatient visits for acute respiratory illnesses. J Air Waste Manage Assoc 60:163–175
Strickland MJ, Klein M, Flanders WD, Chang HH, Mulholland JA, Tolbert PE, Darrow LA (2014) Epidemiology. E Pub
Taylor MP, Camenzuli D, Kristensen LJ, Forbes M, Zahran S (2013) Environmental lead exposure risks associated with children’s outdoor playgrounds. Environ Pollut 178:447–54
Thurston GD, Lippmann M, Scott M, Jonathan AM, Fine M (1997) Summertime haze air pollution and children with asthma. Am J Respir Crit Care Med 155:654–660
Thurston GD, Ito K, Mar T, Christensen WF, Eatough DJ, Henry RC et al (2005) Workgroup report: workshop on source apportionment of particulate matter health effects—intercomparison of results and implications. Environ Health Perspect 113:1768–1774
Tzivian L (2011) Outdoor air pollution and asthma in children. J Asthma 48:470–481
Vedal S, Petkau J, White R, Blair J (1998) Acute effects of ambient inhalable particulates in asthmatic and nonasthmatic children. Am J Respir Crit Care Med 157:1034–1043
Vedal S, Hannigan MP, Dutton SJ, Miller SL, Milford JB, Rabinovitch N et al (2009) The Denver Aerosol Sources and Health (DASH) study: overview and early findings. Atmos Environ (1994) 43:1666–1673
Wang X, Dockery DW, Wypij D, Fay ME, Ferris BG (1993) Pulmonary function between 6 and 18 years of age. Pediatr Pulmonol 15:75–88
Wang LY, Zhong Y, Wheeler L (2005) Direct and indirect costs of asthma in school age children. Prev Chronic Dis 2:1–10 (www.cdc.gov/pcd/issues/2005/jan/04_0053.htm)
Wanger J, Clausen JL, Coates A, Pedersen OF, Brusasco V, Burgos F et al (2005) Standardisation of the measurement of lung volumes. Eur Respir J 26:511–522
Zhou J, Ito K, Lall R, Lippmann M, Thurston G (2011) Time-series analysis of mortality effects of fine particulate matter components in Detroit and Seattle. Environ Health Perspect 119:461–466
Zora JE, Sarnat SE, Raysoni AU, Johnson BA, Li WW, Greenwald R, Holguin F, Stock TH, Sarnat JA (2013) Association between urban air pollution and pediatric asthma control in El Paso Texas. Sci Total Environ 448:56–65
Acknowledgments
This study was supported by the Electric Power Research Institute (EP-P15909/C7932). The authors would like to thank Tom Gentile, George O’Connor, and Lance Wallace, members of the CAPAS study scientific advisory committee, for their guidance in all phases of the study. Steve Ferguson and Mike Wolfson are also acknowledged for designing the air sampling monitors and conducting laboratory analyses. We thank Dr. Fred Moshary of CCNY for sharing his facilities. The authors would also like to thank all the individuals who participated in this study.
Conflict of interest
Dr. Rohr is employed by the Electric Power research Institute (EPRI) which is primarily supported by the electric industry in the US and abroad. EPRI is an independent 501(c)(3) organization that funds external research at a number of universities and institutes worldwide. Other authors declare no conflict of interest personal, financial or otherwise with the material presented in the manuscript.
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplement Table 1a
Correlation coefficients matrix for pollutants and weather parameters (WINTER). (DOCX 26 kb)
Supplement Table 1b
Correlation coefficients matrix for pollutants and weather parameters (SUMMER). (DOCX 29 kb)
Supplement Table 2
P-values testing for Proportional Odds Ratios (OR) for total symptom score (cough and wheeze) per interquartile range increase in daily outdoor pollutant levels. All ORs were adjusted for gender, Hispanic ethnicity, daily ambient maximum relative humidity, average temperature and same day ozone. (DOC 73 kb)
Supplement Table 3
Proportional Odds Ratios (OR) for more albuterol puffs per interquartile range increase in daily outdoor pollutant levels on all seven lag days. All ORs were adjusted for gender, Hispanic ethnicity, daily ambient maximum relative humidity, average temperature and same day Ozone. (DOCX 53 kb)
Supplement Table 4
Proportional Odds Ratios (OR) for lung function AM and PM (PEF% of predicted and daily lability) per interquartile range increase in daily outdoor pollutant levels on same day and lag day 4. All ORs were adjusted for gender, Hispanic ethnicity, daily ambient maximum relative humidity, average temperature. We show ORs both adjusted and unadjusted for same day Ozone. (DOCX 43 kb)
Supplement Figure 1a
Forest plots for symptoms and ambient pollutants (PM2.5 and PM10 and pollutants with borderline significance [0.1>p>0.05] winter adverse ORs). (DOC 1367 kb)
Supplement Figure 1b
Forest plots of pollutants demonstrating non-significant delayed adverse symptom effects in winter. Seven day lags illustrated for Summer and Winter. All ORs were adjusted for gender, Hispanic ethnicity, daily ambient maximum relative humidity, average temperature and Ozone. (DOC 29 kb)
Rights and permissions
About this article

Cite this article
Schachter, E.N., Moshier, E., Habre, R. et al. Outdoor air pollution and health effects in urban children with moderate to severe asthma. Air Qual Atmos Health 9, 251–263 (2016). https://doi.org/10.1007/s11869-015-0335-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11869-015-0335-6