
Abstract
Background
The dynamic hip screw (DHS) is a common device used in the fixation of hip fractures. Traditionally, this involves the use of a four-hole side plate. Reducing the length of the side plate would theoretically reduce the amount of surgical exposure required, decrease surgery duration, and decrease perioperative morbidity and mortality. Our study aims to review the current evidence regarding the use of two-hole side plates, their use and potential complications.
Methods
Using PRISMA guidelines, two independent reviewers performed a search to collate the available literature from medical databases PubMed, EMBASE, Web of Science, and the Cochrane library. Only clinical and biochemical studies were included. The reference lists of articles included for full text review were searched for any additional primary or review publications.
Results
Four online libraries were searched, with a combined total of 5344 titles reviewed. Following title, abstract, and full text review, 8 articles were considered suitable for inclusion in qualitative analysis. There was a trend towards equal efficiency between two- and four-hole plates when used in stable fractures in terms of blood loss, failure/revision rates, operative and hospital stay durations, collapse loading testing, maximum stress, and fragment migration.
Conclusion
The results of this study show that DHS constructs with two- or four-hole side plates have comparable outcomes when used in patients with stable fracture patterns. However, the majority of the clinical data regarding the use of two-hole DHS plates come from retrospective case series; further prospective, randomised control trials would be of significant benefit.
Level of evidence
Level II; systematic review of all levels of evidence
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The incidence of hip fractures is steadily increasing in the global population, particularly in the osteoporotic patient, with multiple significant co-morbidities [1, 2]. The literature describes numerous anatomical variations of hip fractures, for which various fixation methods are widely practiced [2]. Orthopaedic surgeons routinely use varieties of dynamic hip screws (DHS) in the acute management of intertrochanteric or non-displaced intra-capsular femur fractures; these fracture types are reported to account for approximately 50% of all hip fractures [3]. The routine use of DHS as routine in managing such fractures results in a considerable reduction in 1-year postoperative mortality, with the literature reporting reductions to approximately 12% when DHS is utilised compared with nonoperative management [4, 5]. In 2017, the Irish Hip Fracture Database (IHFD) reported that over 700 patients who underwent internal fixation were treated with DHS as a means of definitive surgical management, including 45% of patients with intertrochanteric hip fractures and 21% of all patients with hip fractures overall [6].
Numerous classification systems are reported in the orthopaedic literature in describing intertrochanteric femur fractures. The Evans classification, subsequently modified by Jensen et al., was used historically to classify intertrochanteric hip fractures as it was believed to demonstrate the most reliable prediction of the reduction instability and risk of secondary fracture dislocation [7]. In recent times, the AO classification is the most commonly utilised fracture classification system as it is believed to be a superior guide for orthopaedic surgeons in terms of preoperative planning in offering orthopaedic surgeons guidance as to which fixation method to deploy [8]. Optimal fracture site classification is of paramount importance to orthopaedic surgeons, as debate centres on the use of intramedullary nailing versus DHS in intertrochanteric fractures; appropriate fracture site classification often tips the balance in terms of the fixation method used [9].
Since Clawson’s introduction of the DHS in 1964, it has become widely used in the management of intertrochanteric hip fractures [10]. With DHS offering orthopaedic surgeons satisfactory reductions with low rates of failure over the past five decades, many varieties of DHS plate have been developed; however, the two-hole and four-hole DHS varieties have become popular as the implant of choice in intertrochanteric hip fracture management in recent years [11]. These two options are based on a common principle that is anatomic reduction of the fracture site with dynamic screw fixation of the head and neck of femur secured by fixation of lateral femoral surface from the greater trochanter inferiorly [12]. Theoretically, two-hole DHS plating is expected to reduce operative time, intraoperative blood loss as well as incision site morbidity whilst maintaining an adequate fixation [13]. However, discrepancies in the literature often generate debate on this topic. Biochemical studies have reported that a minimum of three screws is required for adequate femoral fixation with DHS in such fractures [14]. In spite of this, other studies suggest that similar rigid fixation can be achieved when using a three-hole DHS plate when compared with a four-hole plate [15]. The purpose of this study was to review the current available evidence related to the use of two-hole side plates, their use as well as their potential complications.
Methods
Search strategy
Two independent reviewers performed a systematic review of MEDLINE, the Cochrane Library, and EMBASE databases as outlined by the Preferred Reporting for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The following keywords were utilised for the search: (“hip fractures” OR “hip fracture” [Title/Abstract]) OR (“intertrochanteric fracture” [Title/Abstract]) AND (“bone screws” OR “bone screw”[Title/Abstract]) OR (“2 hole”[Title/Abstract] OR “2-hole”[Title/Abstract] OR “two hole”[Title/Abstract] OR “two-hole”[Title/Abstract] OR “4 hole” [Title/Abstract] OR “4-hole” [Title/Abstract] OR “four hole” [Title/Abstract] OR four-hole [Title/Abstract]) OR (“dynamic hip screw” OR “dhs” [Title/Abstract]).
Both independent reviewers screened all titles and abstracts of each of the returned studies. The findings of both reviewers were compared with any discrepancies then being reviewed and clarified by the senior author. The full texts of all potentially relevant studies were subsequently reviewed with reference lists being reviewed for further study screening.
Inclusion and exclusion criteria
Our inclusion criteria included studies matching the following: (1) any study (including retrospective, biomechanical, and cadaveric studies) comparing outcomes of two-hole and four-hole DHS, (2) studies written in fluent English, (3) papers published in a peer-reviewed journal, and (4) full text must have been available. Our exclusion criteria included studies matching the following: (1) papers not published in English, (2) papers without peer-review, (3) papers not published in the past 20 years.
Outcomes of interest
Outcomes of interest for clinical studies included in this study included the following: (1) blood loss, (2) failure/revision rates, and (3) operative and hospital stay durations. Outcomes of interest for cadaveric and biomechanical studies included in this study included the following: (1) collapse loading testing, (2) maximum stress, and (3) fragment migration.
Statistical analysis
Two independent reviewers extracted the data from each of the included studies. Each study’s level of evidence (LOE) was examined and evaluated based on the criteria established by The Journal of Bone and Joint Surgery. Statistical analysis was performed using the SPSS (IBM Corp. Released 2013. IBM SPSS Statistics for Macintosh, Version 22.0. Armonk, NY: IBM Corp.). These studies were not suitable for meta-analysis. p values of < 0.05 were evaluated as statistically significant.
Results
Literature search
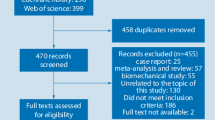
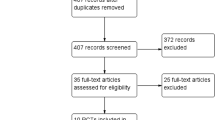
The search yielded in a total of 5297 studies returned. A total of 2191 duplicate studies were removed and the abstracts of 215 remaining articles were assessed using our inclusion and exclusion criteria. This resulted in 8 studies published between 2000 and 2019 with 665 patients included in this review. The PRISMA study selection flow diagram is shown in Fig. 1.

PRISMA
Study characteristics
Eight studies (five clinical and three cadaveric/biomechanical studies) with 631 patients and 34 cadaveric femurs were included. For all studies, the selection and reporting bias were deemed to be low. The study characteristics are illustrated in Table 1 [16,17,18,19,20,21,22,23].
Clinical studies
Four studies including 571 patients compared the use of two-hole versus four-hole DHS. One study including 60 patients compared two-hole DHS with cannulated screws. There was a minimum follow-up of 6 months in all of the included studies.
Blood loss
Two studies reported blood loss differences between those who underwent two-hole versus four-hole DHS. One study reported a statistically significant difference in reductions in postoperative haemoglobin levels (when compared with preoperative samples) in the two-hole versus the four-hole DHS (change of 26 g/L versus 31.3 g/L respectively; p < 0.004) [16]. In the same study, those who underwent two-hole DHS had non-significantly lower rates of perioperative blood transfusions (43% in the two-hole DHS group, versus 60% in the four-hole DHS group, respectively) [16]. The other study reported a mean estimated blood loss of 41.9 mL in 13 patients who underwent two-hole DHS, with no comparison made to four-hole DHS [17].
Failure/revision rates
Three studies reported findings relating to the differences in failure rates between two-hole and four-hole DHS in 470 patients. One of the included studies reported statistically significantly higher failure rates in using two-hole DHS when compared with four-hole DHS when managing unstable intertrochanteric hip fractures in 208 patients (24.4% versus 4.9% respectively; p = 0.048) [16]. However, the same study reported no significant difference in the failure rates between two-hole and four-hole DHS when managing stable fractures in 119 patients (6.3% versus 10.8%: p = 0.68). Similarly, the other two included studies reported failure rates of 3.6% and 3.1% in the management of 143 patients managed with two-hole DHS [18, 19].
Operative and hospital stay durations
One of the included studies reported a non-statistically significant difference in length of hospital stay between those undergoing two-hole versus four-hole DHS. This study reported that in 327 patients, the mean length of hospital stay in two-hole DHS patients was 3 days longer than those who had fixation with the four-hole DHS plate (16 days versus 19 days respectively; p = 0.10) [16].
One of the included studies reported a statistically significant difference in operative duration between those who underwent two-hole versus four-hole DHS. This study reported that in 327 patients, the mean duration in two-hole DHS surgery was statistically significantly lower than the operative duration of the four-hole plate (38.44 min and 51.45 min respectively; p < 0.001) [16].
Cadaveric and biomechanical studies
Three studies including 34 cadaveric femurs compared the use of two-hole DHS versus four-hole DHS.
Collapse loading test
Two of the included studies reported findings relating to the differences in collapse loading testing between two-hole and four-hole DHS in cadaveric femurs. One of the included studies reported a statistically significant difference between the collapse loading testing between two-hole and four-hole DHS (3120 N versus 4160 N respectively) [21]. The other study reported no difference in terms of collapse loading testing between the two groups [22].
Maximum stress
Two of the included studies reported findings relating to the differences in maximum stress tolerated between two-hole and four-hole DHS in cadaveric femurs. One of the included studies reported a statistically significant difference between the collapse loading testing between two-hole and four-hole DHS, reporting that the two-hole DHS has the ability to tolerate up to four times more stress than the four-hole plate (p = 0.02) [21]. The other study reported no difference in terms of collapse loading testing between the two groups [23].
Fragment migration
One of the included studies reported a statistically significant difference in fragment migration during cyclical loading between two-hole and four-hole DHS. This study reported that in cyclic testing of 8 cadaveric femurs, the two-hole DHS exhibited statistically smaller fragment migration in both shear and distraction when compared with the four-hole configuration (p < 0.05) [23].
Discussion
The most important finding in our study was that current clinical and biomechanical studies suggest that two-hole DHS has comparable and even superior outcomes in the management of intertrochanteric hip fractures in terms of duration of surgery, blood loss, and biomechanical testing, when compared with four-hole DHS. This study demonstrates that patient who underwent four-hole DHS as opposed to two-hole DHS had lower failure rates as well as shorter length of hospital stay. Despite these findings, discrepancies in statistical significance between both groups remain and therefore in preoperative planning, each surgeon requires appropriate DHS configuration selection on a fracture-by-fracture basis.
The use of DHS for fixation of intertrochanteric femoral fractures is commonplace in modern orthopaedic surgery as low complication rates have been seen to compliment satisfactory fracture fixation, particularly in fractures that are deemed “stable” [24]. Alongside this, a role has also been described for the use of DHS in fixation of undisplaced intra-capsular neck of femur fractures, particularly Garden I and II type fractures [25]. Despite extensive classification of intertrochanteric femoral fractures, debate continues to be generated between surgeons as to what characteristics of a fracture constitute it being classified as stable or unstable. Many orthopaedic surgeons today commonly regard intertrochanteric femoral fractures with three or more fragments to be considered as unstable (these are classified as “A2”), with instability increasing with the degree of appreciated comminution as described by the AO classification system. In addition to this, transverse or reverse obliquity fractures of the intertrochanteric region are regarded as being the most unstable with high levels of displacement (these are denoted as “A3”) [26]. The use of the AO classification has been adopted by the majority of orthopaedic surgeons in trauma centres; however, a question still arises regarding interobserver reliability on a surgeon-to-surgeon and centre-to-centre basis [26, 27]. Studies demonstrate that interobserver reliability in classification of the stability of intertrochanteric femoral fractures is inconsistent with major discrepancies existing amongst participating surgeons with not only the Evans and Jensen classifications but also the AO classification [28, 29]. For this reason, we must question whether discrepancies in the use of either two-hole or four-hole DHS will continue regardless of modern orthopaedic evidence, as surgeon preference is an element that no guidelines or literature can account for.
For many years now, the orthopaedic literature has concluded that DHS has a clear role in the management of intertrochanteric femoral fractures [9]. However, there are contrasting opinions and reports published in the orthopaedic literature relating to the optimal number of screws when using DHS as operative management of intertrochanteric hip fractures. Some specialist opinions suggest that only with four-hole DHS alone can an orthopaedic surgeon be confident that adequate anatomical reduction is maintained when the patient if fully mobilised postoperatively [23]. Interestingly, a study by Yian et al. in 1997 reported that the use of DHS in the management of intertrochanteric hip fractures is optimal when plates with three bone screws are utilised, as an even distribution of tensile forces results from this [14]. In light of this, evolution of thought in recent years has led to the increasing use of two-hole DHS being deployed for fixation of intertrochanteric femoral fractures. Numerous studies argue that two-hole DHS offers potentially shorter operative times with minimally invasive wound incisions that theoretically minimise patient morbidity postoperatively [30, 31]. On review of the literature, no immediate consensus has been concluded in distinguishing the benefits of two-hole versus four-hole DHS; however, comparable results have been reported in human, cadaveric, and biomechanical studies. However, a poverty of prospective, multi-centre, randomised control trial comparing outcomes of two-hole versus four-hole DHS exists in current literature; such studies are required prior to drawing a definitive conclusion on the matter.
Limitations
There were numerous limitations of this review, primarily related to poverty of high-level evidence on the subject at present. However despite this, a major strength of this study included that the selection of included studies was as per the strict inclusion criteria. Only studies published in the English language were included which immediately introduces a potential selection bias. There were numerous discrepancies between the variables used in each of the studies included such as the following: (1) clinical and cadaveric/biochemical studies were both included, (2) the specific outcomes of interest in the various included studies, and (3) the duration of clinical follow-up. Such variations limit the consistency and comparability of the results obtained in this study and therefore restricts our ultimate conclusions. Such discrepancies deemed quantitative analysis to be inapplicable with no meta-analysis being performed for this review.
Conclusion
The results of this study show that DHS constructs with two- or four-hole side plates have comparable outcomes when used in patients with stable fracture patterns. However, the majority of the clinical data regarding the use of two-hole DHS plates come from retrospective case series; further prospective, randomised control trials would be of significant benefit.
References
Cooper C, Campion G, Melton LJ (1992) Hip fractures in the elderly: a world-wide projection. Osteoporosis Int 2(6):285–289
Bhandari M, Tornetta P, Hanson B et al (2009) Optimal internal fixation for femoral neck fractures: multiple screws or sliding hip screws? J Orthop Trauma 23(6):403–407
Gallagher JC, Melton LJ, Riggs BL et al (1980) Epidemiology of fractures of the proximal femur in Rochester Minnesota. Clin Orthop 150:163–167
Aharonoff GB, Koval KJ, Skovron ML, Zuckerman JD (1997) Hip fractures in the elderly: predictors of one-year mortality. J Orthop Trauma 11:162–165
Richmond J, Aharonoff GB, Zuckerman JD et al (2003) Mortality risk after hip fracture. J Orthop Trauma 17(SUPPLEMENT):S2–S5
National Office of Clinical Audit (2018) Irish Hip Fracture Database National Report 2017. National Office of Clinical Audit, Dublin
Jensen JS (1980) Classification of trochanteric fractures. Acta Orthop Scand 51(1–6):803–810
Van Embden D, Rhemrev SJ, Meylaerts SAG et al (2010) The comparison of two classifications for trochanteric femur fractures: the AO/ASIF classification and the Jensen classification. Injury 41(4):377–381
Parker MJ, Pryor GA (1996) Gamma versus DHS nailing for extracapsular femoral fractures. Int Orthop 20(3):163–168
Clawson DK (1964) Trochanteric fractures treated by the sliding screw plate fixation method. J Trauma 4:737–752
Rao JP, Banzon MT, Weiss AB et al (1983) Treatment of unstable intertrochanteric fractures with anatomic reduction and compression hip screw fixation. Clin Orthop 175:65–71
Doppelt SH (1980) The sliding compression screw - today’s best answer for stabilization of intertrochanteric hip fractures. Orthop C/in North Am; 1
Lee YS, Huang HL, Lo TY et al (2007) Dynamic hip screw in the treatment of intertrochanteric fractures: a comparison of two fixation methods. Int Orthop 31(5):683–688
Yian EH, Banerji I, Matthews LS (1997) Optimal side-plate fixation for unstable intertrochanteric hip fractures. J Orthop Trauma 11(4):254–259
Olsen M, Goshulak P, Crookshank MC et al (2018) Biomechanical testing of a 3-hole versus a 4-hole sliding hip screw in the presence of a retrograde intramedullary nail for ipsilateral intertrochanteric and femur shaft fractures. J Orthop Trauma 32(8):419–424
Baird R, O’Brien P, Cruickshank D (2014) Comparison of stable and unstable pertrochanteric femur fractures managed with 2- and 4-hole side plates. Can J Surg 57(5):327–330
DiPaola M, Razbruch SR, Helfet DL (2004) Minimal incision technique using a two-hole plate for fixation of stable intertrochanteric hip fractures. Orthopaedics 27(3):270–274
Laohapoonrungsee A, Arpornchayanon O, Phornputkul C (2005) Two-hole side-plate DHS in the treatment of intertrochanteric fracture: results and complications. Injury 36(11):1355–1360
Watson A, Zhang Y, Beattie S et al (2012) Prospective randomized controlled trial comparing dynamic hip screw and screw fixation for undisplaced subcapital hip fractures. ANZ J Surg 83(9):679–683
Verhofstad MHJ, Van Der Werken C (2004) DHS osteosynthesis for stable pertrochanteric femur fractures with a two-hole side plate. Injury 35(10):999–1002
Peleg E, Mosheiff R, Liebergall M et al (2006) A short plate compression screw with diagonal bolts—a biomechanical evaluation performed experimentally and by numerical computation. Clin Biomech 21(9):963–968
Rog D, Grigsby P, Hill Z et al (2017) A biomechanical comparison of the two- and four-hole side-plate dynamic hip screw in an osteoporotic composite femur model. J Orthop Surg 25(2):230949901771719
McLoughlin S, Wheeler D, Rider J, Bolhofner B (2000) Biomechanical evaluation of the dynamic hip screw with two- and four-hole side plates. J Orthop Trauma 14(5):318–323
Leung F, Gudushauri P, Yuen G et al (2012) Dynamic hip screw blade fixation for intertrochanteric hip fractures. J Orthop Surg 20(3):302–306
Lee YS, Chen SH, Tsuang YH et al (2008) Internal fixation of undisplaced femoral neck fractures in the elderly: a retrospective comparison of fixation methods. J Trauma 64(1):155–162
Kokoroghiannis C, Aktselis I, Deligeorgis A et al (2012) Evolving concepts of stability and intramedullary fixation of intertrochanteric fractures—a review. Injury 43(6):686–693
Müller ME, Koch P, Nazarian S et al (1990) The comprehensive classification of fractures of long bones. https://doi.org/10.1007/978-3-642-61261-9
Andersen E, Jørgensen LG, Hededam LT (1990) Evans’ classification of trochanteric fractures: an assessment of the interobserver and intraobserver reliability. Injury 21(6):377–378
Pervez H, Parker MJ, Pryor GA, Lutchman L, Chirodian N (2002) Classification of trochanteric fracture of the proximal femur: a study of the reliability of current systems. Injury 33(8):713–715
Alobaid A, Harvey EJ, Elder GM et al (2004) Minimally invasive dynamic hip screw. J Orthop Trauma 18(4):207–212
Říha D, Bartoníček J (2009) Internal fixation of pertrochanteric fractures using DHS with a two-hole side-plate. Int Orthop 34(6):877–882
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Davey, M.S., Flynn, S.O., Hayes, J. et al. Two-hole versus four-hole plate dynamic hip screw: a systematic review of current evidence. Ir J Med Sci 189, 1317–1322 (2020). https://doi.org/10.1007/s11845-020-02184-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-020-02184-9