
Abstract
The upper femur has long held a fascination for both clinicians and bioengineers as it contains two trabecular columns obviously related to its function. In this respect two theories as to the formation of these columns have developed, both associated with Wolff: the Trajectorial Theory, which relates mainly to the passage of forces through the cancellous bone of the upper femur, and Wolff’s Law of bone formation, which describes the bone’s reaction to these forces and relates to bone in general. The two concepts nevertheless are often used synonymously. The Trajectorial Theory propounds that these cancellous structures in the femoral neck are due to both tension and compression forces, while modern day concepts of Wolff’s Law only acknowledge the action of compression forces: and herein lies the paradox. The Trajectorial Theory and Wolff’s Law, when applied to the upper femur, are mutually exclusive. The evidence, anatomical and physiological, indicates that bone forms within the femoral neck solely under the influence of compression forces. This would indicate that the Trajectorial Theory is not appropriate for this region. An alternative conceptual way of looking at this region is presented which eliminates this theory and resolves the paradox.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The human femoral neck contains obvious internal structures, most evident of which are two trabecular columns, one vertical and the other horizontal. These trabecular columns, clinically, are best visualized on antero-posterior radiographs of the hip joint in which it is seen that they pass deeply through the femoral head, terminating close to the subchondral bone. The horizontal trabeculae, as they traverse the femoral head, are seen to cross the vertical trabeculae more or less at right angles (Fig. 1).

Diagram of the ‘compression’ and ‘tension’ trabecular columns in the femoral neck
As the internal structures within the upper femur are obviously related to the mechanical function of the femur they have caught the attention of many investigators, the most well known of which was Wolff [1]. He wrote extensively on the subject and has left us two legacies in this respect: the Trajectorial Theory and Wolff’s ‘Law’.
In his book, Wolff considers these two ideas together and in the literature the terms often seem to be used synonymously; whereas the concepts are completely different. Wolff’s Law, as stated, proposes the effect of physiological forces acting through living bone while the Trajectorial Theory proposes the path which these forces take, notably through the upper femur as shown by the pattern of the trabeculae.
The Trajectorial Theory
Bertrum and Swartz [2] state that the Trajectorial Theory of the organization of the trabeculae in cancellous bone is the fundamental cornerstone in the framework of Wolff’s Law. Enlow [3], in his monograph, considers that the Trabecular Theory has become one of the most useful, albeit controversial, twentieth century concepts and its concept has been widely accepted.
In essence the Trajectorial Theory, when applied to the upper femur, considers that the bone adapts to the applied forces by coalescing at a tangent to the lines of both tension and compression stresses generated within its substance during activity; the vertical column conducting compressive forces and the horizontal column conducting tensile forces. In relation to this theory, Wolff emphasized the fact that where these columns met they crossed at right angles to conform to the concepts of graphic statics [1, 4, 5].
Although an avid proponent for these concepts, Wolff acknowledged that he was not the first to relate the trabecular columns within the femoral neck to the forces of compression and tension passing through the upper femur.
The first, Wolff indicates, were Bourgery and Jacob in 1832 in their textbook of anatomy. He also quotes Ward, perhaps better known, who in 1838 compared the trabecular structure within the upper femur to that of a ‘crane’, i.e. the configuration of the stanchions which held the gas lamps in the streets of Victorian London, and suggested that the compressive and tensile stresses were invoked in the upper femur by similar loading [1, 6] (Fig. 2).

Representation of Ward’s concept relating the structure of a gas-lamp to that of the trabecular columns within the femoral neck
More relevant to the development of Wolff’s Trajectorial Theory was the anatomist Von Meyer who, in 1867, published line drawings of his dissections of the upper femur. Culmann, the originator of graphic statics (a graphic vector representation of the forces which pass through mechanical objects), observed that the cancellous architecture of this region, as depicted by Von Meyer, was similar to the drawings of the stress trajectories which he had computed to be within a curved “Fairbairn” crane [7] (Fig. 3).

Representation of the force diagram by Culmann in relation to the stress trajectories within a curved (Fairbairn) crane
Wolff set out, in association with Culmann, to explore this concept using Fournier sections of the upper femur. His findings, he felt, confirmed this idea and supported the concept that “the proximal end of the femur is stressed not only in compression but also in bending because of the neck shaft angle” and that this “entails an appropriate orientation of bony trabeculae”. His conclusion was that “in the proximal femur, bone is present only along the mathematical stress trajectories and thus is built along the compression and tension lines”. In addition, he emphasized that the two trabecular columns cross at right angles, as this was a requirement of graphic statics, and felt that this was a vital part of the structure [1, 6–8]. Wolff promoted his views and theories fiercely [7], the consequence being that his tenets have been almost universally accepted and are still widely applied.
Koch [6], an ardent supporter of Wolff, investigated the normal femur as a ‘mechanical structure’ on as strict a mathematical basis as possible. In his investigation he “believed in the accuracy of the model of the upper femur defined by Culmann” [9] and considered the femur as an isolated beam structure [10] whose main stressing occurred as a result of the superincumbent load of the body weight. He felt that these stresses are much greater in magnitude than normally may be produced by the muscles alone. Similarly, he felt that “although it is recognized that the action of the muscles exerts an appreciable effect on the stresses in the femur, it is relatively small and very difficult to analyze. For this reason the effect of the action of the muscles will not be investigated”. Following Wolff, he considered the upper femur as an isolated cantilever beam which was loaded in its upper portion and concluded that “The trabeculae of the upper femur, as shown in frontal sections, are arranged in two general systems, compressive and tensile, which correspond in position with the lines of maximum and minimum stresses in the femur determined by the mathematical analysis of the femur as a mechanical structure” [7]. His treatise stood unchallenged as the definitive model of hip biomechanics for the next 70 years. It also served as a foundation for the design, testing and validation of hip replacement prostheses [9].
The second factor in the continuing acceptance of this theory appears to be the increasing dependence of investigators on advanced technology. The structure of these trabecular columns has been extensively investigated using various imaging modalities. These techniques have included two-dimensional finite element analysis (FEA) [11–14] and three-dimensional FEA which are now typically modeled using radiographs [15] and computerized axial tomography [16–19]. Recently, microcomputer tomographic images of the bone specimens are being used on the basis that they show the bone with greater accuracy, assessing individual trabeculae rather than a homogenized continuum [13, 20, 21].
Steihl et al. [22] consider that quantitative computed tomography (QCT) is an excellent tool for the study of the distribution of cortical and trabecular bone in the human body. The cross-sectional presentation of QCT gives a clear, unambiguous picture of the internal anatomic structure. Magnetic resonance imaging techniques also allow the creation of three-dimensional models which enhance the modeling of the anatomy of the bones and muscles, as well as muscle and joint motions [22–25]. The results of these investigations, nevertheless, are dependent upon the specificity, sensitivity and resolution of the imaging. They give a virtual image, the analysis of which is dependent upon the capacity of the computers used and the parameters fed into them. The analysis is limited by the fact that external loading conditions and material properties are not always known with great precision, so simplifying assumptions must be made [26].
Despite using models generated by three-dimensional CAT reconstructions, Keyak and Falkinstein [20] feel that the FEA models still analyze the upper femur as an isolated cantilever structure with little reference to muscular action and no reference to the spiral configuration of the femoral neck.
The use of FEA in functional morphology is described and discussed by Richmond et al. [14]. Perhaps most importantly, they emphasize the importance of validation of these various models used for the analysis as they seem to maintain the potential source of error by continuing to use only one- or two-dimensional determinations.
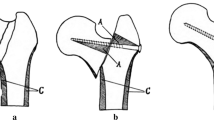
Wolff’s comment regarding the internal architecture of the upper femur was that “it is not very complicated and can be understood particularly easily”. This being so one can describe the situation in a fairly simple manner if one considers the upper femur to be fashioned from a ball atop a single, slightly inclined stick fixed at its base (Fig. 4a). The ball represents the femoral head and the stick the vertical trabecular column. If the ball (femoral head) is loaded in this situation the stick will tend to bend (Fig. 4b). To counter this bending it is then necessary for the body to hold the femoral head in position by connecting the ball (femoral head) to a horizontal trabecular column which will exert a tension force to counteract the bending (Fig. 4c). Thus, when loaded, the vertical column will remain straight. In order that there is no shear effect between the two trabecular columns it is necessary for them to cross at 90°.

Representation of the trabecular theory’s concepts of the action of the roles of the internal trabecular columns within the femoral neck. The small arrow in c donates the required tension strut
The hip joint moves widely in three dimensions. This being so it is of concern that, despite all these present day methods, biomechanical assessments of the hip joint continue to assess its function in two dimensions, mostly with the hip considered to be in the fully extended position as in standing and quiet walking.
Wolff’s Law of bone development
Wolff’s second legacy is his famous “Law” of bone formation:
“Every change in the form and function of bone or of their function alone is followed by certain definite changes in their internal architecture, and equally definite alteration in their external configuration, in accordance with mathematical laws”. [1, 27–30].
This basically states that bone will form in relation to the forces to which it is subjected and this is applicable to bone in general [28].
Wolff’s Law captured the notion of a relationship between form and function in bone [26] but his “Law” was the result of his observations on a series of pathologically healed fractures. Wolff confesses that he only considered the alterations in bone which occur in individuals who “work in circumstances different from normal” and admits in his book that the task of determining the exact growth changes of the internal architecture in each bony area during (normal) growth remained an enormous task for the anatomist [1, 31]. As this “Law” does not predict the specific effects of specific mechanical challenges, mathematically or verbally, Frost considers that it is a statement of relevance and not a law [29]. This being the case, it is recommended that the concept of “functional adaptation to bone forces”, as proposed by Roux, should be adopted. This is considered to be more appropriate than the term “Wolff’s Law”, when this is used in its more general sense of bone developing in response to its mechanical loading, rather than having to consider the specific mathematical rules which Wolff propounded [2, 7, 32, 33].
Investigators have pondered for centuries as to the nature, composition and growth of bone. It was John Hunter, in 1798, who recognized that bone grows in width by outer deposition and inner resorption and is “constantly changing its matter”. Later, in the nineteenth century, other workers (such as Flourens, Brulle and Hugeny, and Loven) recognized that this process of ‘remodeling’ takes place during growth [3].
Remodeling is a fundamental process in the skeleton and is an orderly, progressive mechanism of adjustment which maintains the constant shape, proportions and relationships of a bone during its growth [3]. It is, however, only comparatively recently that the mechanisms which control this process have begun to be understood.
There is now much evidence that architectural adaptations follow a major change in bone loading [34]. Initially, it was felt that the mechanical stimulus on the bone bringing about its adaptation is the stress to which the bone is subjected [8, 11]. Subsequently, it has become accepted that the feedback mechanism for this process is governed by the strain within the bone [30, 34–37].
When designing a tissue, strain is one of the most relevant parameters to control [38]. If the induced strains are too high, the probability of failure of the tissue increases. If the strains are too low, the structures will be unnecessarily robust and energy is wasted in synthesis, maintenance and transport. Generally the bone would attempt to maintain the strain arising from normal activities within a specific range and that there would be no adaptive modeling response below a minimal level, shown to be below 0.0008–0.0015 unit strain [34]. However, should the intermittent, internal strains regularly approach or exceed 0.002 unit strain during normal activities, a response to strengthen the bone will occur by increasing the cross-sectional area, thus reducing these internal strains back to the physiological range (between 0.0050 and 0.0015 unit strain). This theory of ‘minimum effective strain’ (MES) would predict precisely when and where lamellar bone architectural adaptations occur in response to mechanical factors. The tissue’s ability to sustain functional loading, without failure or damage, is achieved because the cells can regulate the orientation, mass and physical properties of their matrix in relation to the requirements of prevailing functional load-bearing [3, 29, 30, 34].
As the mechanical properties of bone do not change significantly when its loading patterns change, adaptation of its architecture remains the only viable option and is the biological basis of these changes. In cortical bone the change is brought about by osteoblastic and osteoclastic bone surface drifts which build up bone surface on one side and erode it on another in coordinated patterns, and this sculpting is termed ‘bone modeling’ [3, 29, 30].
The effect of these changes, initiated by an increase in the internal strain, is to align the bone with the applied stress and to strengthen it by increasing its thickness or diameter to bring the level of strain back to within the normal physiological range [29, 34, 39–41].
Applying Wolff’s Law to the upper femur it can be seen that should there be a bending stress placed upon the femoral head, sufficient to cause an off-centered strain or bending of the femoral neck (Fig. 5a), the bone of the vertical trabecular column will respond to the increased strain by aligning itself with the applied force, as well as hypertrophying to reduce the internal strain back to its physiological levels (Fig. 5b).

Representation of the theory of Wolff’s Law. The arrows in b indicate the realignment and increased diameter of the vertical column as a result of compression stress
The paradox
The paradox between Wolff’s Trajectorial Theory and his Law of Bone Transformation (Wolff’s Law) is that while the Trajectorial Theory demands that complementary tension forces must exist within the bone of the upper femur and be dealt with by an additional strut, Wolff’s Law demonstrates that bone aligns and strengthens itself solely to the applied compression force and an additional tension device is unnecessary.
Discussion
The human femur is not an isolated, cantilevered mechanical beam designed to take static forces but is an important, integrated and functional part of a living, vital and mobile organism. Biological studies and the clinical problems concerned (in orthopedic biomechanics) are complex. Scientific progress in this area requires a sound understanding of engineering mechanics on the one hand and a profound appreciation of the complex reality on the other [42].
It must be appreciated that Wolff’s Law of bone remodeling and the Trajectorial Theory are two separate concepts. Wolff’s Law considers the effect on living bone of applied (physiological) forces. The Trajectorial Theory deals with the apparent nature and direction of forces through the upper femur. From the above it is obvious that these two distinct concepts, when applied to the upper femur, are mutually exclusive. Which then is the correct theory to apply to the upper femur?
While Wolff’s Law is generally, although sometimes begrudgingly, accepted there has always been circumspection, as well as downright antagonism, towards the Trajectorial Theory. According to Wolf’s law, the anatomical form corresponds to mechanical stress patterns realized within the bone. Previous authors have applied engineering concepts to this analysis, suggesting the presence of both compressive and tensile forces within the proximal femur. Nevertheless, simplistic two-dimensional anatomical and force models may not adequately predict the stresses present in such a three-dimensional structure [22, 43].
What are the arguments against the Trajectorial Theory?
Koch, following Wolff, also concluded that “The thickness and spacing of the trabeculae vary with the intensity of the maximum stresses at various points in the upper femur, being thickest and most closely spaced in the regions where the greatest stresses occur” [7]. This contention has been severely criticized by Rybicki et al. [10] who feel that “It is, of course, difficult to prove or disprove whether the trabecular pattern is associated with imposed stresses or due to other physiological reasons such as nourishment requirements”.
Wolff placed great emphasis on the need for the two trabecular columns to cross at right angles (orthogonality) as this is required by static graphics. Jansen [44] emphasizes that the trabeculae in the upper femur generally do not cross at right angles.
Garden [45] states that the mechanics of the joint, depicted diagrammatically in the form of a simple lever, “fails utterly to indicate the complexity of hip joint function”. He continues that the theories of Ward, Culmann and Meyer have contributed to the belief that the structure of the femoral neck embodies mechanical principles which are foreign to bony formations elsewhere. “This isolated departure from the normal pattern of bone behavior is considered to be most unlikely”.
Cowin [7] makes the point that the ‘rigid form’ of Wolff’s Law of Trabecular Architecture is nonsense and has been identified as such almost from its publication. He maintains that Wolff’s Law of Trabecular Architecture is a false premise for a number of reasons. First, there cannot be a one-to-one correspondence between the stress trajectories in a linearly elastic, homogenous isotropic object in the shape of real bone on the one hand and the trabeculae in a real bone on the other. Second, in the model there are an infinite number of stress trajectories between two points whereas there are only a finite number of trabeculae between them. Third, bones are subjected to variable, not static loads which are unknown. Fourth, many writers have disputed that the trabeculae cross at right angles. Cowin nevertheless, in another paper, goes on to state that a ‘resolution length restriction’ on the trabecular bone, in which the length scale on which trabecular bone can be considered as a continuous material for the purpose of stress analysis, can preserve the basic idea of the Trajectorial Theory [28].
Criticism regarding the mathematical and mechanical principles
Roesler [46] makes reference to Zschokke, Mohr and Tripel who, he says, criticize Wolff’s ideas on mechanical and mathematical grounds.
Scientific historians have argued that Wolff’s Law is seriously flawed, if not in its conclusions then at least in its derivation. Wolff placed great emphasis on the similarities between the pattern of trabecular bone in the proximal femur and that of the stress trajectories in Culmann’s crane. It follows therefore that if these stresses are incorrect or misinterpreted then Wolff’s deductions, based on this model, are put in question [33].
Rybicki et al. [10] found that the choice of mathematical model to represent the behavior of a bone is important. They pointed out that the stresses in the shaft of the femur may appropriately be analyzed using slender beam theory as was done by Koch. However, in the regions of the femoral head, the greater trochanter, and areas of muscle attachments, the assumptions inherent in beam theory become questionable. They concluded that beam theory can give acceptable results for stresses in the shaft of the femur, whereas a continuum model should be used in regions where loads are applied or where the shape of the femur is unlike that of a slender beam.
Lee and Taylor [33], quoting Roesler [47], state that the Culmann crane was inaccurate and that Roesler cited two main engineering errors in the crane model:
-
1.
Culmann’s crane was probably based on a straight cantilever having a parabolic shearing stress distribution at its free end and that, to make the geometry more consistent with the proximal femur, some curvature was added to this free end. However, no change was made to the stress distribution to allow for this curvature.
-
2.
To describe the state of stress in a curved bar with a parabolic or near-parabolic distribution of shearing stresses along its free end three different stress components are required. Culmann’s model involved only two components: a two-dimensional solution.
Roesler concluded that the Culmann crane was no more than a good first estimate of the stresses in the proximal femur and that Wolff’s mistake was to read more into Culmann’s analysis than was technically justified.
Questions regarding the effect of tension in the formation of bone
In relation to Wolff’s Law of bone remodeling it has been shown that bone forms in relation to a compressive force, particularly if it is relatively large, and this has been supported by experimental evidence stretching over centuries [3, 37–39, 48, 49]. There is dispute, however, as to whether bone is formed in response to tensile forces.
Although the literature is voluminous, and it is recognized that tension on some soft tissues can promote the formation of bone within its substance [50], there are few, if any, studies which have shown that tension in bone itself brings about bone formation. Chamay and Tschantz [39] in fact have shown that, in long bones, traction causes bone to atrophy by ‘periosteal resorption and intracortical osteolysis’. Similarly, “Where net tension is unlikely to exist, bone does, and where net tension probably does exist, bone does not”. Oxnard [43].
From the time of Wolff, until comparatively recently, the upper femur was studied as an isolated, cantilevered structure. Carter et al. [11] quote several authors, stating that “The modeling and remodeling activity of bone is influenced by the complete loading history to which the tissue is exposed over some period of time” and went on, like many other biomechanical studies of that time, to assess the upper femur in this manner on the basis that this corresponds to the principle stress directions.
An isolated femur, investigated as a cantilever structure, undoubtedly cannot but confirm a tension response in relation to compression loading; but is this physiological? The largest voluntary bone loads and bone strains come from muscles, not body weight as formerly thought by Koch [30].
The photoelastic work of Pauwels [40] demonstrated that tension in a muscle from the greater trochanter to the lateral femoral condyle could reduce the bending stress in the femur. Soft tissues around the hip play an important role in the biomechanics of the hip joint and femur, partly by moving the joint and partly by acting as a tension band which has the effect of converting tension to compression [40, 51]. Frankel [52] states that muscle contraction also plays a vital role in the supportive functions of the hip joint and goes on to state that “the contraction of the gluteus medius generates a compressive stress and strain that acts as a counterbalance to neutralize the tensile strain on the superior cortex of the femoral neck. As a result the lateral trabecular system probably resists the compressive force produced by the contraction of the abductor muscles”.
While the importance of muscle loadings as a source of stress in the skeletal system has now long been recognized, efforts to define these and relate them to stresses in bone have been quite limited [10]. On the other hand, Dude et al. [53] state that if the appropriate muscle groups are considered strain magnitudes and orientations similar to those reported from in vivo measurements may be obtained.
These factors have been progressively introduced into the biomechanical studies of the hip. Initially, it was only the abductor muscles which were incorporated but further soft tissue structures have gradually been added with increasing complexity. Rybicki [10] incorporated the effects of the abductor muscles and the fascia lata and, in a recent paper, Fraldi et al. [54] have incorporated the effects of the hip abductors, the fascia lata and the ileopsoas muscle. It might be asked that if the effect of muscle tension is to reduce the tension passing through the upper femur, would this reduced tension force, if it exists, remain sufficient to generate the horizontal trabecular column?
Carey [55] considered that the trabecular columns are formed as a result of internal ‘pressure’ and not tension. Similarly Tobin [4] reviews and supports the ideas of Jansen and Carey, questioning Wolff’s concepts and maintaining the idea that the trabeculae form only under the influence of a compression force.
Ling et al. [51], quoting Jansen [44], Garden [45], Carey [54] and St Clair Strange [56], state that “contrary to the generally held opinion, both the superior (horizontal) and inferior (medial vertical) trabecular systems are loaded in compression”. In their paper they reproduce a diagram by St Clair Strange showing how the tension of the iliotibial tract can result in a compressive rather than a tensile force through the superior (horizontal) trabecular system, even when the individual is in a single-legged stance position.
Heller et al. [57] bemoan that while there is strong evidence that muscles are major contributors to femoral loading the actual forces occurring in vivo are hardly accessible and non-invasive measurement of in vivo muscle forces is still impossible. Therefore, the only opportunity to estimate the complex distribution of muscle forces is offered by computer analysis. The results of such a study by Rudman et al. [58] serve to support the hypothesis that both trabecular columns conduct a compressive force.
The curvature of the horizontal trabeculae
Biomechanically it is necessary for the two trabecular columns to be in the same plane, if the Trajectorial Theory is to be valid. This is the crux of the Trajectorial Theory.
It is argued that a major source of error in the Trajectorial Theory is the assumption that the two trabecular systems in the upper femur, as shown on a plain X-ray of the hip joint, are in the same coronal plane. The upper femur is a three-dimensional structure whereas plain X-ray films are two dimensional. It must be asked whether, in light of the nature of X-rays, is it not possible that the courses of the trabeculae through the upper femur, as shown in these plain X-ray films, are apparent and may not lie in the same coronal plain rather than being coincident within the upper femur?
Validation is demanded but, in many studies, although the trabecular columns are imaged their actual positions within the femoral neck are not validated and it is assumed that they are in a mechanically valid position. Rarely, does the description of a study record that the underlying concepts for its investigation are based on the Trajectorial Theory, although this may be implicit in its methodology. The fact that the Trajectorial Theory is contentious is unrecognized or studiously ignored and in biomechanical studies the Trajectorial Theory is rarely, if ever, discussed. Certainly, none consider that there may be another way of interpreting the results.
Garden [45] states “The Trajectorial Theory interpretation of the internal weight-bearing system derives largely from Ward (1838) and from the radiographic appearance of the femoral neck and head which Ward’s diagram so well foresaw. However, both diagram and radiograph fail to demonstrate the three-dimensional features of the proximal end of the femur, and for this reason the descriptions of the calcar femorale and internal weight-bearing system are inadequate”. Using stereo-radiography, it was possible for Garden to see that the vertical (medial) trabecular column lies postero-medially and the horizontal (lateral) trabecular column lies antero-superiorly in the femoral neck.
Similarly, the curved and separate trajectory of the horizontal trabeculae has also been described by several authors over the years [45, 51, 59, 60]. This arrangement was also confirmed in the physical dissections of the upper femur by the author [61] in which the two trabecular columns within the femoral neck were well defined and it was evident that they do not lie in the same coronal plane. Thus, the radiological resemblance of the internal structure of the upper femur to a beam is only apparent, being due to the two three-dimensional columns being superimposed onto a two-dimensional X-ray plate. Nevertheless, this has been used as the basis for investigation of hip biomechanics for the last 140 years. Have these investigations been performed on the basis of an illusion?
There is an obvious discrepancy between what can be physically seen and felt of the trabecular columns within the femoral neck and what is obtained by imaging; and this needs to be resolved. Perhaps one factor in the difference is the bone itself. It was observed during the physical dissections [61] that the upper femur in the younger individual is an almost solid piece of bone and the delineation of the columns is subtle. With the overlap of these columns almost any longitudinal section will show a superior and inferior column, although the actual centers and bulk of the columns are offset. It is only as the bone becomes osteoporotic that the two columns separate fully and their relative positions become very much clearer and easier to identify. Alternatively, the problem may lie in the way the computer is programmed to assess the bone, or it may just be that the imaging process is not sensitive enough. It is notable in the study by Steihl et al. [22] that, although they make allusion to an anterior twist of the metaphysis (helix) of the femoral neck, they do not demonstrate the horizontal (superior tensile) trabecular column, despite using quantitative computer tomography.
Is there an alternative to the Trajectorial Theory?
There has been criticism of the Trajectorial Theory ever since it was first postulated by Wolff and many arguments have been put forward to counter it. This being so, it is difficult to understand how it continues to function as the basis of many biomechanical studies without even so much as a comment in this respect. It frequently appears to be so universally accepted as being correct that the fact that it is the basis for a study is not mentioned but is simply found to be implicit in the methodology of the experiment.
Tension and compression are part and parcel of the ‘beam theory’. If the femur is studied as an isolated beam, then it is not surprising that the results confirm that there is tension and compression in the upper femur during the stance position. The recognition that such a situation is not physiological and that the effect of the surrounding muscles is to reduce, or even reverse, the tension forces in the femoral neck requires a modification of this theory.
Most biomechanical studies consider the fully extended hip joint or, at the most, a few degrees of flexion. Heller et al. [57] and Shelly et al. [62], studying total joint force measurements of the hip in stair climbing, showed that activities involving large flexion angles, especially those requiring large flexion moments, generate large hip loads. Nevertheless, the actual courses of the forces generated through the hip were not demonstrated.
Squatting, to undertake a miscellany of tasks, is a physiological activity for many millions of people. The question which then begs an answer is what is the nature of the force and how does it traverse the upper femur while these individuals move to and from the full squatting position?
No biomechanical study describes, let alone mentions, the curved course of the horizontal trabecular column. Bertrum and Scwartz [2] contend that the understanding of functional adaptation in bone has, in many ways, been hindered by the wholesale acceptance of Wolff’s paradigm and that his view of the link between load and bone form has become unexpectedly restrictive, limiting both the design of experiments and the interpretations of equivocal results. Nevertheless, if it were accepted that the main function of this curved (horizontal) trabecular column is to conduct the compressive force through the upper femur during the activities of squatting and climbing, it may begin to explain, in biomechanical terms, how this region of the skeleton functions during the full three-dimensional range of normal hip movement.
A recent study by the author, in which the bone of the upper femur was physically dissected, showed that the arrangement of cancellous bone within the upper femur is complex [61]. It confirmed several of the features previously described to be within the femoral neck and showed the presence of some new features.
It confirmed the helical configuration of the horizontal trabecular column which runs antero-superiorly around the vertical trabecular column. Importantly, it showed that these columns within the femoral neck do not lie in the same coronal plane, as would be expected if the Trajectorial Theory prevailed, but are offset. Thus, the upper femur cannot be regarded as a simple beam, cantilever or otherwise. It also showed that the horizontal trabecular column arises from a large buttress on the inner surface of the anterior femoral wall which is connected to the calcar which, in turn, is connected to the vertical trabecular column.
Importantly, it showed that the cephalic end of the vertical (medial) trabecular column lies within the dome of the acetabulum when the hip is extended, as in the standing position, and that the medial end of the horizontal (superior) trabecular column lies within the dome of the acetabulum when the hip is in the fully flexed (squatting) position. The configuration of all the internal cancellous structures in the femoral neck between the ends of each trabecular column is found to be one of a continuous, sigmoid shape. The curved nature of the horizontal trabecular column fits in well with Wolff’s contention that bone is formed at a tangent to the applied force when the hip femur moves in the hip joint from the fully flexed to the fully extended position. The cortex overlying the trabecular columns is thickened and intimately blends with them. This needs to be considered as, undoubtedly, this cortex participates in carrying the load.
It is hypothesized that the cancellous structures within the femoral neck demonstrate the three-dimensional pathway of the compression force which passes through the upper femur as it moves fully during the individual’s normal everyday physiological activities [61]. Accepting this concept eliminates the Trajectorial Theory and resolves the paradox.
References
Wolff J (1986) The law of bone remodelling (trans: Maquet P, Furlong R). Springer, Berlin
Bertrum JEA, Swartz SM (1991) The ‘law of bone transformation’: a case of crying Wolff? Biol Rev 66:245–273
Enlow DH (1963) Principles of bone modeling. In: Evans FG (ed) American lectures in anatomy. Charles Thomas, Springfield, pp 1–30
Tobin WJ (1955) The internal architecture of the femur and its clinical significance. J Bone Joint Surg Am 37A:57–71
Scott JH (1957) The mechanical basis of bone formation. J Bone Joint Surg Br 39B:134–144
Koch JC (1917) The laws of bone architecture. Am J Anat 21:177–298
Cowin SC (1997) The false premise of Wolff’s Law. Forma 12(3,4):247–262
Turner CH (1992) On Wolff’s Law of trabecular architecture. J Biomech 25:1–9
Fetto J, Leali A, Moroz A (2002) Evolution of the Koch model of the biomechanics of the hip: clinical perspective. J Orthop Sci 7:724–730
Rybicki EF, Simone FA, Weis EB (1972) On the mathematical analysis of stress in the human femur. J Biomech 5:203–215
Carter DR, Orr TE, Fyhrie DP (1989) Relationship between loading history and femoral cancellous bone architecture. J Biomech 22:231–244
Goldstein S, Matthews L, Kuhn J et al (1991) Trabecular bone modelling. An experimental model. J Biomech 24:135–150
Van Rietbergen B, Huiskes R, Eckstein F et al (2003) Trabecular bone tissue strains in the healthy and osteoporotic human femur. J Bone Min Res 18:1781–1788
Richmond BG, Wight BW, Grosse I et al (2005) Finite element analysis in functional morphology. Anat Rec 283A:259–274
Rohlmann A, Mosner U, Bergann G et al (1982) Finite element analysis and experimental investigation of stress in a femur. J Biomed Eng 4:241–246
Zannoni C, Mantovani R, Viceconti M (1988) Material properties assignment to finite element models of bone structures: a new method. Med Eng Phys 20:735–740
Keyak JH, Rossi SA, Jones KA et al (1998) Prediction of femoral fracture load using automated finite element modeling. J Biomech 31:125–133
Gomez-Benito MJ, Garcia-Aznar JM, Doblare M (2005) Finite element prediction of proximal femoral fracture pattern under different load. J Biomech Eng 127:9–14
Roger K, Resnick D, Sartoris DJ et al (2005) Computerized tomography of proximal femoral trabecular patterns. J Orthop Res 4:45–56
Kayak JH, Falkinstein Y (2003) Comparison of in situ and in vitro CT scan based finite element model predictions of proximal femoral fracture load. Med Eng Phys 25:781–787
Verhulp E, Van Rietbergen B, Huiskes R (2006) Comparison of micro-level and continuum-level voxel model of the proximal femur. J Biomech 39:2951–2957
Steihl JB, Jacobson D, Carrera G (2007) Morphological analysis of the proximal femur using quantitative computed tomography. Int Orthop 31:287–292. doi:10.1007/s00264-006-0182-z
Wirtz DC, Pandorf T, Portheine F et al (2003) Concept and development of an orthotropic FE model of the proximal femur. J Biomech 36(2):289–293
Blemker SS, Delp SL (2004) Three-dimensional representation of complex muscle architectures and geometries. Ann Biomed Eng 33:661–673
Blemker SS, Asakawa DS, Gold GE et al (2007) Image based musculo-skeletal modeling: applications, advances and future opportunities. J Magn Reson Imaging 25(2):441–451
Huiskes R (2000) If bone is the answer, then what is the question? J Anat 197:145–156
Frieburg AH (1902) Wolff’s Law and the functional pathogenesis of deformity. Anatomy 124:956–972
Cowin S (1989) A resolution restriction for Wolff’s Law of trabecular architecture. Bull Hosp Joint Dis Orthop Inst 49:205–212
Frost HM (1994) Wolff’s Law and bone’s structural adaptations to mechanical usage: an overview for clinicians. Angle Orthod 64:175–188
Frost H (2001) From Wolff’s Law to the Utah paradigm: insights about bone physiology and its clinical applications. Anat Rec 262:398–419
Prendergast PJ, Huiskes R (1995) The biomechanics of Wolff’s Law: recent advances. Ir J Med Sci 164(2):152–154
Ruff C, Holt B, Trinkhaus E (2006) Who’s afraid of the big bad Wolf? “Wolff’s Law” and bone functional adaptation. Am J Physiol Anthropol 129:484–498
Lee TC, Taylor D (1999) Bone remodeling: should we cry Wolff? Ir J Med Sci 168:102–105
Frost HM (1983) A determinant of bone architecture: the minimum effective strain. Clin Orthop Relat Res 175:286–292
Huiskes R (1997) Validation of adaptive bone remodeling simulation models. In: Lowet G et al (eds) Bone research in biomechanics. IOS Press, Amsterdam, pp 33–48
Goodship AE, Lanyon LE, McFie H (1979) Functional adaptation of bone to increased stress. J Bone Joint Surg Am 61A:539–546
Lanyon LE, Baggott DG (1976) Mechanical function as an influence on the structure and form of bone. J Bone Joint Surg Br 58B:436–443
Rubin CT, Lanyon LE (1985) Regulation of bone mass by mechanical strain magnitude. Calcif Tissue Int 37:411–417
Chamay A, Tschantz P (1972) Mechanical influences in bone remodeling; experimental research of Wolff’s Law. J Biomech 5(2):173–180
Pauwels F (1980) Short survey of the mechanical stressing of bone. In: Maquet P, Furlong R (eds) Biomechanics of the locomotor apparatus. Springer, Berlin, pp 478–503
Hart R (2001) Bone modeling and remodeling: theories and computation. In: Cowin SC (ed) Bone mechanics handbook, 2nd edn. CRC Press, Boca Raton, pp 31–41
Huiskes R, Chao EYS (1983) A survey of finite element analysis in orthopedic biomechanics: the first decade. J Biomech 16:385–409
Oxnard CE (2004) Thoughts on bone biomechanics. Folia Primatol 75:189–201
Jansen M (1920) On bone formation. The University Press, Manchester
Garden RS (1961) The structure and function of the proximal end of the femur. J Bone Joint Surg Br 43B(3):576–589
Roesler H (1987) The history of some fundamental concepts in bone biomechanics. J Biomech 20:1025–1034
Roesler H (1981) Some historical remarks on the theory of cancellous bone structure (Wolff’s Law). In: Cowin SC (ed) Mechanical properties of bone. American Society of Mechanical Engineers, New York, pp 27–42
Meade JB, Cowin SC, Klawitte JJ et al (1984) Bone remodeling due to continuously applied loads. Calcif Tissue Int 36(Suppl):S25–S30
Rubin CT, Lanyon LE (1987) Osteoregulatory nature of mechanical stimuli: function as a determinant for adaptive remodeling in bone. J Orthop Res 5:300–310
Kenwright J, White SH (1993) A historical review of limb lengthening and bone transport. Injury 24(Suppl):S9–S19
Ling RSM, O’Connor JJ, Lu T-W et al (1996) Muscular activity and the biomechanics of the hip. Hip Int 6:91–105
Frankel VH (1986) Biomechanics of the hip joint. Instr Course Lect 35:3–9
Dude GN, Heller M, Albingere J et al (1998) Influence of muscle forces on femoral strain distribution. J Biomech 31:841–846
Fraldi M, Esposito L, Perrella G et al (2009) Topological optimization in hip prosthesis design. Biomech Model Mechanobiol. doi:10.1007/s10237-009-0183-0
Carey EJ (1929) Studies in dynamics of histogenesis. J Radiol 13:127–168
St. Clair Strange FG (1965) The hip. Heinemann, London, pp 28–51 (quoted by Ling et al)
Heller MO, Bergman G, Deuretzbacher G et al (2001) Musculo-skeletal loading conditions at the hip during walking and stair climbing. J Biomech 34:883–893
Rudman KE, Aspden RM, Meakin JR (2006) Compression or tension? The stress distribution in the proximal femur. Biomed Eng 5:12. doi:10.1186/1475-925X-5-12
Dixon AF (1910) The architecture of the cancellous tissue forming the upper end of the femur. J Anat Physiol 45:223–230
Backman S (1957) The proximal end of the femur. Acta Radiol Suppl 146:1–166
Hammer A (2010) The structure of the femoral neck: a physical dissection with emphasis on the internal trabecular system. Ann Anat 192:168–177
Shelley FJ, Anderson DD, Kolar MJ et al (1996) Physical modeling of hip joint forces in stair climbing. Proc Inst Mech Eng 210:65–68
Conflict of interest
Dr. Hammer has nothing to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Hammer, A. The paradox of Wolff’s theories. Ir J Med Sci 184, 13–22 (2015). https://doi.org/10.1007/s11845-014-1070-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-014-1070-y