
Abstract
Background
Despite a steady increase in the rate of breastfeeding in Ireland over the period 2004–2010 (from 46.8 % in 2004 to 55.7 % in 2010), Irish rates of breastfeeding are still low by international standards. Over this period, the characteristics of mothers and babies changed, with mothers increasingly older, having fewer children and increasingly born outside the Republic of Ireland.
Aims
The purpose of this paper is to understand the extent to which changing maternal and birth characteristics explained the increase in the breastfeeding rate in Ireland over the period 2004–2010.
Methods
We apply non-linear decomposition techniques to micro-data from the 2004–2010 Irish National Perinatal Reporting System to examine this issue. The technique allows us to quantify the extent to which the increase in the breastfeeding rate over the period 2004–2010 is due to changing maternal and birth characteristics.
Results
We find that between 55 and 74 % of the increase over the period can be explained by changing characteristics, with the increasing share of mothers from Eastern Europe, and increasing maternal age the most important contributors.
Conclusions
These findings suggest that the existing policy initiatives have been relatively ineffective in increasing breastfeeding rates in Ireland, i.e. most of the observed increase occurred simply because the characteristics of mothers were changing in ways that made them increasingly likely to breastfeed.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The benefits of breastfeeding for babies, mothers and society have been demonstrated in a large scientific literature [1]. Reflecting the proven benefits, the WHO recommends that babies should be exclusively breastfed for the first 6 months and that some breastfeeding should continue up to 2 years old and beyond [2]. Despite this recommendation, breastfeeding initiation and duration rates remain varied across developed countries.
Cross-country comparisons of breastfeeding rates are complicated by a lack of comparable data. Despite the variety of definitions, data sources and collection methods employed, the available data show rates of breastfeeding in Ireland that are considerably lower than other in other European countries. In 2010, Ireland had the lowest ‘any’ breastfeeding rate of 14 European countries, measured both at birth and 48 h postpartum (‘any’ breastfeeding refers to both exclusive breastfeeding and breastfeeding combined with artificial feeding methods) [3]. While the rate in Ireland has been increasing, it remains below national targets [4, 5].
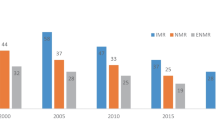
As well as the breastfeeding rate being much lower in Ireland than in other countries there are distinct patterns within Ireland by maternal country of birth. As illustrated in Fig. 1, 46.1 % of Irish-born mothers were breastfeeding at hospital discharge in 2010, in contrast to 84.2 % of non-Irish-born mothers. In addition, the overall breastfeeding at hospital discharge rate was increasing over the period 2004–2010. However, the share of non-Irish-born mothers also increased considerably (from 16.4 % in 2004 to 25.1 % in 2010), and given the much higher rates of breastfeeding among non-Irish-born mothers, it is important to understand the extent to which this compositional change contributed to the overall increase over the period.

Percentage of mothers breastfeeding at discharge from Hospital by Maternal Country of Birth, 2004–2010. *Any breastfeeding includes exclusive breastfeeding and breastfeeding combined with artificial feeding. Sample derived from the National Perinatal Reporting System—see “Methods” for description
Differences in breastfeeding rates by maternal country of birth/race/ethnicity are not unique to Ireland, although the scale of the differential between Irish-born and non-Irish-born mothers is particularly distinctive [6, 7]. The existence of racial/ethnic differences in breastfeeding rates is highlighted by a large body of literature from the US and the UK [8–13]. Much of the previous research in Ireland has focussed on the determinants of breastfeeding initiation and duration, using information collected from small samples [7, 14, 15]. With the exception of the few studies that have noted the discrepancy in breastfeeding behaviour between Irish- and non-Irish-born/nationals/ethnic groups [6, 7, 16], more detailed analysis of the differences, and the change in breastfeeding behaviour over time, is absent. This is partly due to a lack of data [the National Perinatal Reporting System (NPRS), the only source of micro-data on all births in Ireland, first collected information on maternal country of birth in 2004]. Using data from the NPRS, the purpose of this paper is to examine the extent to which the increase in the breastfeeding at hospital discharge rate between 2004 and 2010 is due to changes in maternal characteristics over the period.
Methods
Data source
In this paper, we use the NPRS which reports data on all births over 500 g in the Republic of Ireland (ROI). Over the period 2004–2010, 489,170 live and stillborn births were recorded. Non-hospital births (2,967), births in private hospitals (15,171), and births from one hospital where breastfeeding was underreported (34,905) are excluded. In common with other studies, stillbirths and early neonatal deaths (3,481) and multiple births (15,674) are excluded. In the absence of detailed clinical data we include only healthy babies by excluding babies of <37 weeks gestation (29,258), <2.5 kg (26,433) and where the discharge date of mother and baby are different (21,381). After excluding a further 4,164 observations with missing values on key variables, the final data-set contains 385,549 births, which represents 78.8 % of all births in the ROI between 1 January 2004 and 31 December 2010.
The dependent variable indicates whether the mother was engaged in ‘any’ breastfeeding upon hospital discharge. No data are available on breastfeeding duration. The main independent variable of interest is maternal country of birth, disaggregated into seven mutually exclusive categories: ROI, UK, EU-15 (excluding ROI and UK), EU-27 Accession States (excluding ROI, UK, and EU-15—referred to as EU-27 for the remainder of the paper), Africa, Asia, and other. Information on race/ethnicity or length of time since migration is not available. The data reveal a steady decrease in the proportion of births in this sample to Irish-born mothers, from 83.6 % in 2004 to 74.9 % in 2010.
Other independent variables include those familiar from previous research on breastfeeding determinants [17], such as maternal age, marital status, social class and parity. Variables describing the child’s sex, birthweight, gestation length, type of delivery, postpartum length of stay (LOS) and hospital designation as ‘baby friendly’ under the WHO/UNICEF Baby Friendly Hospital Initiative (BFHI) are also included.
Summary statistics
Table 1 presents the proportion of mothers in the sample who were engaged in ‘any’ breastfeeding at hospital discharge in 2010 by various characteristics (data for 2004–2009 are available from the authors). Mothers that were non-Irish-born, older, married, in higher social classes, with fewer previous children and with a longer postpartum LOS had higher rates of breastfeeding. Mothers of low birthweight babies, those of shorter gestational age and those born via Caesarean section had lower rates. In a multivariate analysis (results of which are available on request from the authors), all of these factors were statistically significant, with the effects for maternal country of birth particularly large and significant.
The main objective of this research is to examine the extent to which the increase in the breastfeeding at hospital discharge rate between 2004 and 2010 can be explained by changing maternal characteristics over the period. In general, over the period, the change in characteristics of mothers is predictive of higher breastfeeding rates over time (e.g. increasing age, social class, non-Irish, falling parity), although there are some exceptions (e.g. declining postpartum LOS, increasing rate of Caesarean section) (Table 2).
Decomposition of the Increase in breastfeeding at hospital discharge rate 2004–2010
To determine the extent to which the increase in the breastfeeding at hospital discharge rate between 2004 and 2010 can be explained by changing maternal characteristics, we use a non-linear decomposition technique [18]. The average difference in the breastfeeding at hospital discharge rate between 2004 and 2010 may be expressed as:
where \( \overline{Y}^{\rm J} \) is the average probability of breastfeeding at hospital discharge for group J (J = A, B), X J i is the vector of independent variables of observation i in group J, \( \hat{\beta }^{\rm J} \) is the vector of coefficients. In this case, group A is the sample of 2010 mothers, group B is the sample of 2004 mothers, and the reference group is group A. We also undertake the decomposition using the estimated group B and pooled coefficients as the reference, to provide a range of estimates [19]. We use the ‘Fairlie’ decomposition command in STATA 12.1 [20].
The first term on the right hand side of Eq. (1) measures the amount of the breastfeeding gap that is due to differences in the characteristics of the two groups. The second term captures the degree to which mothers giving birth in the 2 years, but with similar observable characteristics, breastfeed at different rates. The first part may be further decomposed into the relative contributions of each of the independent variables (e.g. we can quantify the extent to which the breastfeeding differential between 2004 and 2010 is due to differences in maternal age, social class, country of birth, etc.).
Robustness checks
A unique health identifier is not available in NPRS; while it is unlikely that the same woman could give birth twice in one year, it is possible that the same woman could give birth more than once over the period 2004–2010. To test whether our results are dependent on this assumption, we also estimate the models on the sample of primiparous women. There is a larger, albeit still small (3.2 %), proportion of missing observations on maternal country of birth for 2004. We also run the model using 2005 as the start year (results from all robustness checks are available from the authors).
Results
Table 3 presents the results of the decomposition of the change in the breastfeeding at hospital discharge rate between 2004 and 2010, using the 2010 coefficients as the reference. The raw difference in breastfeeding between 2004 and 2010 was 8.8 percentage points. Of that, 4.9 percentage points (or 55.5 %) may be explained by changing maternal characteristics over the period, i.e. on average, characteristics in 2010 were predictive of higher breastfeeding rates. Using the 2004 and pooled coefficients as the reference results in explained components of 61.4 and 73.8 %, respectively.
Decomposing the contributions of each of the independent variables in Table 3 reveals that increasing maternal age explains 13.5 % of the increase in the rate between 2004 and 2010, while the increasing share of EU-27 mothers explains 36.8 %. Other variables make much smaller contributions, although it is important to note that the breastfeeding at hospital discharge rate would have actually fallen between 2004 and 2010 if mothers in 2004 had the same postpartum LOS as mothers in 2010, holding all else constant.
Discussion
The benefits of breastfeeding for mothers, babies and society have been demonstrated in a large scientific literature. Irish rates of breastfeeding are very low by international standards, despite a steadily increasing rate in recent years. There has been no attempt to analyse the reasons for the recent increase in the breastfeeding rate in Ireland, and in particular, to examine the possibility that an increasing proportion of non-Irish-born mothers may have driven much of the observed increase. The availability of detailed micro-data on the full census of births over the period 2004–2010 allowed us to examine this issue in greater detail than before.
Despite the size of the data-set, there are inevitably some limitations. First, our indicator of breastfeeding refers to ‘any’ breastfeeding at hospital discharge. Information on breastfeeding initiation at birth or on the duration of breastfeeding is not available. Second, detailed clinical information is not available, although we have attempted to control for this by excluding low birthweight babies, those born early, and those where the discharge data of mother and baby are different. Third, information on race/ethnicity and/or ‘length of time since migration’ is not available. Finally, there are a number of potentially important variables for which information is not available from NPRS (e.g. smoking status, antenatal intention to breastfeed, etc.).
The results show that between 55 and 74 % of the increase in the breastfeeding rate over the period 2004–2010 was due to changing maternal characteristics. Further decomposition confirms that the majority of the increase over the period is accounted for by the increasing share of EU-27 mothers, and by increasing maternal age. This suggests that existing policy initiatives have been relatively ineffective in increasing breastfeeding rates in Ireland. Much of the increase in the breastfeeding rate in Ireland occurred simply because, over the period 2004–2010, the characteristics of mothers were changing in ways that made them increasingly likely to breastfeed.
References
American Academy of Pediatrics (2005) Section on breastfeeding: breastfeeding and the use of human milk. Pediatrics 115(2):496–506
WHO (2003) Global strategy for infant and young child feeding. WHO, Geneva
EURO-PERISTAT Project, SCPE EUROCAT, EURONEOSTAT (2013) European perinatal health report
Department of Health and Children (1994) A national breastfeeding policy for Ireland. Department of Health and Children, Dublin
Department of Health and Children (2005) Breastfeeding in Ireland: a five-year strategic action plan. Department of Health and Children, Dublin
Begley C, Gallagher L, Clarke M, Carroll M, Millar S (2009) National infant feeding survey 2008. School of Nursing and Midwifery, Trinity College, Dublin
Tarrant RC, Younger KM, Sheridan-Pereira M, White MJ, Kearney JM (2009) The prevalence and determinants of breast-feeding initiation and duration in a sample of women in Ireland. Public Health Nutr 13(6):760–770
Griffiths LJ, Tate AR, Dezateux C, The Millennium Cohort Study Child Health Group (2005) The contribution of parental and community ethnicity to breastfeeding practices: evidence from the Millennium Cohort Study. Int J Epidemiol 34(6):1378–1386
Kelly YJ, Watt RG, Nazroo JY (2006) Racial/ethnic differences in breastfeeding initiation and continuation in the United Kingdom and comparison with findings in the United States. Pediatrics 118(5):e1428–e1435
Celi AC, Rich-Edwards JW, Richardson MK, Kleinman KP, Gillman MW (2005) Immigration, race/ethnicity, and social and economic factors as predictors of breastfeeding initiation. Arch Pediatr Adolesc Med 159(3):255–260
Merewood A, Brooks D, Bauchner H, MacAuley L, Mehta SD (2006) Maternal birthplace and breastfeeding initiation among term and preterm infants: a statewide assessment for Massachusetts. Pediatrics 118(4):e1048–e1054
Singh GK, Kogan MD, Dee DL (2007) Nativity/immigrant status, race/ethnicity, and socioeconomic determinants of breastfeeding initiation and duration in the United States, 2003. Pediatrics 119(Supplement):S38–S46
Li R, Grummer-Strawn L (2002) Racial and ethnic disparities in breastfeeding among United States infants: Third National Health and Nutrition Examination Survey, 1988–1994. Birth 29(4):251–257
Fitzpatrick C, Fitzpatrick P, Darling M (1994) Factors associated with the decision to breastfeed among Irish women. Ir Med J 87(5):145–146
Ward M, Sheridan A, Howell F, Hegarty I, O’Farrell A (2004) Infant feeding: factors affecting initiation, exclusivity and duration. Ir Med J 97(7):197–199
McCrory C, Layte R (2011) The effect of breastfeeding on children’s educational test scores at nine years of age: results of an Irish cohort study. Soc Sci Med 2(9):1515–1521
Dennis C-L (2002) Breastfeeding initiation and duration: a 1990–2000 literature review. J Obstet Gynecol Neonatal Nurs 31(1):12–32
Fairlie R (2005) An extension of the Blinder-Oaxaca decomposition technique to logit and probit models. J Econ Soc Meas 30(4):305–316
Bhalotra S, Valente C, van Soest A (2010) The puzzle of Muslim advantage in child survival in India. J Health Econ 29(2):191–204
Jann B (2006) Fairlie: Stata module to generate nonlinear decomposition of binary outcome differentials
Acknowledgments
The authors would like to thank the National Perinatal Reporting System (NPRS) team in the Health Research and Information Division at the Economic and Social Research Institute (ESRI) for access to the NPRS data, as well as Dr Genevieve Becker [National Co-ordinator for WHO/UNICEF Baby Friendly Hospital Initiative (BFHI) in Ireland] for access to data on the BFHI. The authors would also like to thank seminar participants at the ESRI and ECHE 2012 for helpful comments.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Brick, A., Nolan, A. Explaining the increase in breastfeeding at hospital discharge in Ireland, 2004–2010. Ir J Med Sci 183, 333–339 (2014). https://doi.org/10.1007/s11845-013-1012-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-013-1012-0