
Abstract
Background
This study establishes baseline prevalence of smoking and cigarette consumption among Cork bar workers prior to the Republic of Ireland’s (ROI) smokefree workplace legislation and compares gender- and age-specific smoking rates and estimates the adjusted odds of being a smoker for Cork bar workers relative to the general population.
Methods
Cross-sectional random sample of bar workers in Cork city and cross-sectional random telephone survey of the general population were conducted prior to the smokefree legislation.
Results
Self reported smoking prevalence among Cork bar workers (n = 129) was 54% (58% using cotinine-validated measures), with particularly high rates in women (70%) and 18–28 years old (72%). Within the ROI (n = 1,240) sub-sample rates were substantially lower at 28%. Bar workers were twice as likely to be smokers as the general population sub-sample (OR = 2.15).
Conclusions
Cork bar workers constitute an occupational group with an extremely high smoking prevalence.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
For many years legislation in Ireland has prohibited smoking in most public places, providing protection for many workers. However much of the service industries, including pubs, were exempt. On 29 March 2004, Republic of Ireland (ROI) became the first European country to introduce nationwide smokefree workplace legislation for all workplaces including pubs and restaurants. Smoking is now prohibited in enclosed work places with few exceptions.
The Irish service industries, as in other countries, are low paid and largely non-unionised, a situation conducive to poor health behaviours. Bar workers can be considered as a highly vulnerable group whose health would be expected to benefit greatly from a smokefree work environment for two reasons. First, without smoking bans in place, bar workers are exposed to high levels of secondhand smoke at work [1, 2]. After the introduction of the smokefree workplace legislation in Ireland, cotinine levels dropped in non-smoking bar workers indicating significant reductions in secondhand smoke exposure [3, 4].
Second, research suggests that bar workers constitute an occupational group with a high proportion of active smokers. Jones et al. [5] found a 40% prevalence in hospitality workers in New Zealand, and Bang and Kim [6] reported a smoking rate of 44.5% among waiters and waitresses and 39% in those working in eating and drinking venues including pubs. Although the smokefree workplace legislation in Ireland was introduced as a measure to protect workers from secondhand smoke, the policy might also result in decreased smoking in the working population. Corroborating evidence for beneficial effects of workplace smoking restrictions on smoking prevalence and consumption rates has been reported by several authors [7–11]. However, non-representative samples and lack of comparison with occupation-specific general population smoking rates of the respective countries limit the interpretation and generalisability of these findings.
Little is known about smoking rates in hospitality workers in Ireland although anecdotal evidence suggested that the rate of smoking among Irish bar workers was high. In order to establish smoking prevalence estimates for this group we enrolled a random sample of Cork city bar workers comprising floor staff, bar managers and owners. The objectives were (1) to establish a baseline prevalence of smoking and cigarette consumption among Cork bar workers prior to the introduction of the smokefree workplace legislation; (2) to compare gender- and age-specific smoking rates in Cork bar workers with the equivalent occupational classes within the general population; and (3) to estimate the adjusted odds of being a smoker for Cork bar workers relative to the general population (sub-sample).
This study provides the first estimates of smoking prevalence and cigarette consumption in bar workers adjusted to enable comparisons with the general population.
Methods
We used two datasets for this study: (1) bar workers from Cork City, part of a larger study, the ‘All-Ireland bar study’ reported elsewhere [3]; (2) a subset from a general population (ROI) telephone survey conducted by TNS mrbi, a commercial research company.
Sample selection
Bar workers
A three step cluster sampling strategy was used (Fig. 1). First, 300 streets were randomly selected from a list of all Cork city streets (obtained from Cork City Corporation), using the random number generator in SPSS 12.0.1 (SPSS, Chicago, IL). Second, all pubs located on these 300 streets were selected resulting in 171 pubs representing 44% of the approximately 385 pubs in Cork city. Third, we randomly selected up to two bar workers at the time of the visit. If only one/two worker(s) was/were present at the time of the visit, only one/two worker(s) was/were selected. If a randomly selected bar worker was unable or unwilling to participate, a replacement bar worker was then randomly selected (if possible) from the same pub.

Sampling and participation of Cork city bars and bar workers. *Best estimate of number of pubs in Cork city in early 2004
Participants were interviewed in the pub where they worked between January and March 2004 (before implementation of the smokefree workplace legislation). Only those actively involved in everyday tasks within the pub and who were over 18 years were eligible. We enrolled both smoking and non-smoking bar workers and all occupational positions i.e. owners, managers, full- and part-time bar staff. Follow-up post-ban surveys were completed 1 and 2 years later, but will not be detailed here.
General population sub-sample
General population data were obtained from an ongoing national monthly telephone survey of 1,000 randomly selected individuals (>15 years) during the same time period as the bar workers survey (January–March 2004). Participants were selected based on randomly generated phone numbers; targets were met in relation to gender, age, occupational class and region. For comparison purposes the general population sample was restricted to participants of similar age (≥18 years) and with occupations equivalent to bar workers. This sample is referred to as the general population sub-sample. We used un-weighted data as we compared estimates within age, gender and occupational class strata.
Measures
Bar workers
Survey administration and salivary cotinine sampling procedures were described in more detail elsewhere [3].
Sociodemographics
Participants were asked about their gender, age, and occupational position as an indicator of occupational class. Occupational class was determined by involvement in the pub: owners and managers were categorised as ‘manager’ (occupational class C2), temporary and permanent staff as ‘staff’ (occupational class DE). The term ‘bar worker’ refers to the entire sample. The occupational class classification was taken from the ROI Central Statistics Office (CSO) [12] classification which is based on the UK Standard Occupational Classification [13].
Smoking status
Participants were asked about their current smoking status, average cigarette consumption per day and smoking history. Two different measures of smoking status were used for bar workers: ‘self reported’ smoking status and ‘combined self report and cotinine’ smoking status. Self reported smoking status (self reported current smoker versus current non-smoker) was used when comparing bar workers with the general population sub-sample.
Combined self report and cotinine smoking status was obtained by validating self reports by cotinine (where possible). Non-smokers were defined as those who self reported as current non-smokers and had cotinine concentration levels <20 ng/ml (113.6 nmol/l) [3]. Smokers were defined as those who self reported as current smokers plus those who self reported to be non-smokers but with cotinine concentration levels of ≥20 ng/ml (113.6 nmol/l). In cases where cotinine was not available due to insufficient samples or refusals, the self reported smoking status was used (28 cases). The self reported and cotinine combined measure was used to provide a more accurate estimate of the smoking prevalence in bar workers as it takes potential under-reporting of smoking into account.
General population sub-sample
Sociodemographics and smoking status
Participants were asked about their gender, age group, self reported smoking status (‘do you smoke >1 cigarette per week’), self reported cigarette smoking consumption and occupation. Occupation classes equivalent to the bar managers and owners (occupational class C2) and bar staff (occupational class DE) were selected.
Statistical analysis
Data analysis was conducted using SPSS 12.0.1 (SPSS, Chicago, IL). Pearson’s chi square or Fisher’s exact test was used to examine gender, age and occupational class patterns in prevalence. The Mann–Whitney U test and the Kruskall Wallis H test were used to test for differences in consumption by sociodemographic characteristics. Logistic regression models were built for both samples with smoking status as outcome, adjusting for gender, age and occupational class.
Results
Study participation
Study participation is shown in Fig. 1. A final pub participation rate of 69.5% (98/141) with 129 bar workers enrolled in the study. A replacement bar worker was required in 9% of cases.
Of the 2,460 individuals enrolled in the national telephone survey over the 3 months, there were 1,240 participants ≥18 years with occupational class equivalent to the bar workers.
Table 1 shows the demographic characteristics of the participating bar workers and the general population sub-sample. Among participating bar workers 69% were male, mean age 33 years; 56% were temporary or permanent staff (equivalent to occupational class DE) and the remaining 44% were either owners or managers (equivalent to occupational class C2). In comparison to the general population sub-sample, bar workers were more likely to be male and younger (88% under 49 years of age compared to 52%).
Bar worker smoking prevalence: combined self report and cotinine
Table 2 shows the prevalence of smoking among Cork bar workers by gender, age and occupational class. The overall prevalence of smoking (combined self report and cotinine) in bar workers was 58.1% (95% CI 49.5–66.6); 70% of female bar workers were smokers compared to 53% of male bar workers (P = 0.067). Smoking prevalence was 72.3% in 18–28 years old but decreased significantly with age. Staff had a significantly higher smoking prevalence (68%) than managers (46%) (P = 0.01).
Bar worker prevalence (self reported) in comparison to the general population sub-sample
We compared the prevalence for bar workers with the corresponding rates in the general population sub-sample (Table 2). As cotinine-validated data were not available for the general population, we used the self reported smoking status for the bar workers which vary slightly from the partially cotinine-validated estimates. The overall prevalence of smoking in the general population sub-sample was 28.3% compared to 54.3% in bar workers. As the age and gender distributions differ, we compared gender- and age-specific rates. Higher prevalence rates in bar workers were observed for both genders and both occupational classes. Among bar workers, women (65%) were more likely to be smokers than men (49%) (P = 0.07), whereas almost equal proportions of men and women (29.1 vs. 27.5%) in the general population sub-sample were smokers. The gender difference was particularly striking in bar workers classified as managers: 37.5% of male managers smoked compared to 66.7% of female managers. This pattern in managers was not observed in the general population sub-sample. Bar workers also had substantially higher rates within the younger age groups, especially the 18–28 year olds. Comparison of the older age groups was limited due to the small numbers of bar workers.
Bar worker cigarette consumption in comparison with the general population sub-sample
The mean number of cigarettes consumed (self reported) by bar workers was 16.7 (SD = 11.5) per day, similar to the 16.9 (SD = 9.8) per day consumed by the general population sub-sample (Table 3). In the general population sub-sample, men consumed more cigarettes than women (19 vs. 15 cigarettes per day, P = 0.018); this gender difference was not observed in bar workers (P = 0.8). Consumption varied by age among bar workers (P = 0.099) with the highest consumption rates in the 29–48 years category. Average consumption for 29–48 years old bar workers was much higher than in the corresponding age groups of the general population but the confidence intervals of the estimates in bar workers were very wide. Among bar workers, comparison of average consumption between male and female staff and managers was constrained by the small numbers within these sub-categories.
Adjusted smoking prevalence
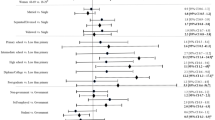
In order to control for the differences in age, gender and occupation distribution between the bar worker sample and the general population sub-sample, three logistic regression models were built, one for bar workers, one for the general population sub-sample and a final model comparing bar workers with the general population sub-sample taking age, gender and occupational class into account (Table 4). Due to small numbers in the older age groups, the age categories ‘49–58 years’ and ‘59–78 years’ were combined.
Bar workers were more than twice as likely to be smokers as the general population sub-sample (adjusted OR = 2.15, 95% confidence limits 1.45–3.17, P < 0.01). In all three models age was an independent predictor of smoking with generally decreasing prevalence by age. Neither gender nor occupational class was found to be independent predictors of smoking status in any of the models.
Discussion
Main findings
Smoking prevalence among Cork bar workers is extremely high at 58%, higher than in other similar studies [5, 6]. Due to the random sampling methods employed, the high response rate and the use of validated smoking status, this study provides to our knowledge the best estimate available of smoking prevalence in this occupational group. A higher prevalence rate (83.3%) was found in male Asian American restaurant workers in Boston [14]. However, Averbach’s estimates were based on a convenience sample and are not generalisable to a larger population.
The social and cultural environment in Ireland may influence bar workers’ smoking behaviour. A strong tradition of alcohol consumption and its association with smoking within the pub culture in Ireland meant that bar workers were continuously surrounded by smoke and alcohol with possible ‘normalisation’ of smoking. This may partially explain the magnitude of this group’s smoking prevalence. Another explanation may be that smokers, especially young smokers, are attracted to the pub trade. In our sample, the mean age bar workers started smoking was 17.7 years of age with female bar workers starting at a slightly younger age (17.3 years) than males (18.0 years). Evidence on whether individuals were already smokers before they started working in the hospitality industry or whether they became smokers after they started working is best obtained by longitudinal studies.
Furthermore bar workers cannot be considered a homogeneous group; they comprised bar owners, managers, and temporary and permanent staff with different socio-economic positions. As higher smoking rates are commonly observed within lower occupational and social classes, we conducted class-specific analyses. As expected, bar staff had a significantly higher prevalence of smoking than bar managers.
Bar workers had more than double the odds of being a smoker than individuals in the general population sub-sample. This result highlights the magnitude of smoking as an issue in this unique population. Interestingly, age remained an independent significant predictor of smoking in both samples.
The present study has established a baseline prevalence among bar workers which can be contrasted with post-ban prevalence thereby clarifying the differential effects of workplace health protection measures on smoking behaviour.
Limitations of this study
Because of the random sampling strategy and the low refusal rate our results can be seen as representative of bar workers in a city area. Cork city is a small urban area comprising 123,000 citizens. It is possible that smoking behaviour among bar workers is different in rural areas; however, we are confident that our sample also included people from rural backgrounds [private addresses were available for 75 participants (58%); 60 (80%) identified that they were currently living in Cork city and 15 (20%) identified that they were currently living outside the city]. We have no reason to expect significant differences in smoking patterns for bar workers within the ROI generally.
With regard to the telephone survey assessment of population smoking rates, there is likely to be under-sampling of some population groups such as foreign workers and students, who are less likely to have land lines. Smoking rates in such groups may differ from the general population. Other ROI general population surveys such as SLÁN [15, 16] do exist but were either unavailable for our analysis or may be seen as out of date; we therefore consider our dataset to be the best estimate of smoking available for the general population.
Differences in methodology between the general population and bar worker samples limited comparisons. Bar workers were interviewed in a face to face interview while the general population were interviewed over the telephone, this may have introduced a bias into the general population data as some evidence suggests that interviewee are more likely to give socially desirable answers during a telephone interview [17]. This difference may have inflated the odds ratio comparing the prevalence of bar workers with the prevalence of the general population. Coupled with the likely under-sampling of foreign workers and students, this general population sample may underestimate the true smoking prevalence in Ireland. Classification of occupational class may not be completely comparable between the two samples but this should not affect the overall findings. And finally, different questions were used to assess self reported smoking status; the general population sub-sample was asked ‘Do you smoke more than 1 cigarette per week?’ while bar workers were asked whether they were current, occasional, ex or never smokers. Very light smoker may have underestimated their smoking in the bar worker sample, however, the availability of cotinine concentrations for most of the bar workers allowed us to identify non-reporting smokers. The fact that only five individuals were so re-categorised showed that bar workers’ self reporting was reasonably accurate.
As cotinine concentrations were not available for 28 individuals, we were not able to validate all self reports. We cannot fully exclude systematic bias, i.e. that particularly smokers refused to provide a saliva sample. However, as only 14 (50%) of those without cotinine samples were due to refusal (5 of whom were self reported smokers), and the rest of missing cotinine samples was caused by insufficient or contaminated samples (10 of whom were self reported smokers). In addition missing cotinine values were fairly evenly distributed among smokers and non-smokers: 15 reported being smokers, 5 reported being ex-smokers and 7 reported being never smokers. Re-analysis including only those individuals who had cotinine data (n = 101) showed rates that were generally very similar to those reported in Table 2: a smoking rate (cotinine-validated) of 59.4% and a very similar distribution of smokers between the genders (53% in males, 73% in females) and both occupational classes (managers 48%, staff 69%), but a slightly higher rate in the youngest age group of 18–28 years (77%).
Establishing baseline prevalence among this vulnerable occupational group will facilitate post-ban examinations of the impact of the smoking ban, a legal measure that is currently considered in several countries. The effect of the Irish smoking ban on passive smoking are well documented such as the reduction in exposure to secondhand smoke in non-smoking bar workers [3], exposure to particulate matter and benzene [18] and subsequent improvements in respiratory symptoms and respiratory health [3, 18]. However, as the health consequences of active smoking are more pronounced than those of passive smoking, the impact of the ban on active smoking behaviour in addition to existing evidence of positive effects on passive smoke levels may constitute important scientific evidence for future policy planning.
References
Jarvis M, Foulds J, Feyerabend C (1992) Exposure to passive smoking among bar staff. Br J Addict 87(1):111–113. doi:10.1111/j.1360-0443.1992.tb01906.x
Bates M, Fawcett J, Dickson S, Berezowski R, Garrett N (2002) Exposure of hospitality workers to environmental tobacco smoke. Tob Control 11(2):125–129. doi:10.1136/tc.11.2.125
Allwright S, Paul G, Greiner B et al (2005) Legislation for smoke-free workplaces and health of bar workers in Ireland: before and after study. Br Med J 331(7525):1117. doi:10.1136/bmj.38636.499225.55
Mulcahy M, Evans DS, Hammond SK, Repace JL, Byrne M (2005) Secondhand smoke exposure and risk following the Irish smoking ban: an assessment of salivary cotinine concentrations in hotel workers and air nicotine levels in bars. Tob Control 14(6):384–388. doi:10.1136/tc.2005.011635
Jones S, Love C, Thomson G, Green R, Howden-Chapman P (2001) Second-hand smoke at work: the exposure, perceptions and attitudes of bar and restaurant workers to environmental tobacco smoke. Aust N Z J Public Health 25(1):90–93. doi:10.1111/j.1467-842X.2001.tb00557.x
Bang K, Kim J (2001) Prevalence of cigarette smoking by occupation and industry in the United States. Am J Ind Med 40(3):233–239. doi:10.1002/ajim.1094
Chapman S, Borland R, Scollo M, Brownson R, Dominello A, Woodward S (1999) The impact of smoke-free workplaces on declining cigarette consumption in Australia and the United States. Am J Public Health 89(7):1018–1023
Woodruff TJ, Rosbrook B, Pierce J, Glantz SA (1993) Lower levels of cigarette consumption found in smoke-free workplaces in California. Arch Intern Med 153(12):1485–1493. doi:10.1001/archinte.153.12.1485
Brenner HFB (1994) Smoking regulations at the workplace and smoking behavior: a study from Southern Germany. Prev Med 23:230–234. doi:10.1006/pmed.1994.1031
Longo DR, Johnson JC, Kruse RL, Brownson RC, Hewett JE (2001) A prospective investigation of the impact of smoking bans on tobacco cessation and relapse. Tob Control 10(3):267–272. doi:10.1136/tc.10.3.267
Fichtenberg C, Glantz S (2002) Effect of smoke-free workplaces on smoking behaviour: systematic review. BMJ 188(7357):188. doi:10.1136/bmj.325.7357.188
Office CS www.cso.ie
Standard Occupational Classification (1995) 2nd edn, London
Averbach ARLD, Lam LJ, Sharfstein J, Cohen B, Koh H (2002) Smoking behaviours and attitudes among male restaurant workers in Boston’s Chinatown: a pilot study. Tob Control 11:34–37
SLÁN The National Health and Lifestyle Surveys Centre for Health Promotion Studies, Galway: National University of Ireland (1999) Galway: Centre for Health Promotion Studies, National University of Ireland
SLÁN The National Health and Lifestyle Surveys Galway: Centre for Health Promotion Studies, National University of Ireland (2003)
Holbrook AL, Green MC, Krosnick JONA (2003) Telephone versus face-to-face interviewing of national probability samples with long questionnaires: comparisons of respondent satisficing and social desirability response bias. Public Opin Qual 67:79–125. doi:10.1086/346010
Goodman P, Agnew M, McCaffrey M, Paul G, Clancy L (2007) Effects of the Irish smoking ban on respiratory health of bar workers and air quality in Dublin pubs. Am J Respir Crit Care Med 175:840–845. doi:10.1164/rccm.200608-1085OC
Acknowledgments
We thank Sangeetha N. Kalimuthu and Meenakshi Uppel, for help with interviewing; Ann Kelly for help with data entry, Dr. Tony Fitzgerald for statistics advice. We especially thank the bar workers who participated in this study.
The research was ethically approved by the clinical research ethics committee of the Cork Teaching Hospitals. Research ethics committee of the Faculty of Public Health Medicine, Royal College of Physicians of Ireland.
The research was funded by Health Research Board of Ireland (Research project grant RP/2005/290). Department of Epidemiology and Public Health, University College Cork; Office of Tobacco Control through the Research Institute for a Tobacco Free Society (Republic of Ireland); the National Cancer Institute of the United States (R01 CA90955); Irish Cancer Society; Irish Heart Foundation. All authors’ work was independent of all funders.
Conflicts of interest
SA is a member of the Board of the Irish Office of Tobacco Control (unpaid position). IJP is the unpaid chair of the Irish Research Institute for a Tobacco Free Society.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mullally, B.J., Greiner, B.A., Allwright, S. et al. Prevalence of smoking among bar workers prior to the Republic of Ireland smokefree workplace legislation. Ir J Med Sci 177, 309–316 (2008). https://doi.org/10.1007/s11845-008-0196-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11845-008-0196-1