
Abstract
Background
Non-union in children is considered a rare but real complication of fracture management; however there is no information available in the literature regarding its incidence. The aim of this work was to investigate the incidence of fractures and non-union in children for different anatomical regions/age groups, and for the first time to publish data regarding the rate of non-union per fracture in children in a large population.
Method
Prospective data for all hospital admissions for paediatric fractures and paediatric fracture non-union in Scotland between 2005 and 2010 was obtained. Regional data for total paediatric fracture numbers was also available enabling total fracture numbers and non-union incidence at a national level to be calculated.
Results
There were 180 non-unions in the 0–14 year olds and 242 non-unions in 15–19 year olds recorded over 5 years in a population of 1.2 million children (0–19 years). The number of fractures during this time period for the same age groups were 92,200 and 68,900 respectively. The risk of fracture increased steadily with age; it was greater in boys than girls and far higher in the upper than lower limb. The overall rate of non-union per fracture was 0.2 % in those 14 years and younger and 0.35 % in the 15–19 year olds. Non-union was highest in the male 15–19 year olds at 0.45 % of all fractures. The risk of non-union was far greater in the lower limb fractures than in the upper limb fractures throughout childhood until the age of 15 where the upper limb NU rate per fracture exceeded that of the lower limb.
Conclusions
The calculated risk of non-union per fracture is low throughout childhood with a risk of approximately 1 in 500 or less per fracture in boys aged under 14 years and in girls of all ages, however NU increases to approximately 1 in 200 fractures for the older teenage (15–19 years) boys.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Non-union has significant health and social implications; the treatment for non-union can require multiple operative procedures, the use of strong chemotherapeutics, such as antibiotics and growth factors, and prolonged periods in hospital.
Fracture non-union is considered to be an unusual complication in children; however to date there are no large studies in publication to confirm this.
Aim
The aim of this work was to investigate the incidence of fractures and non-union in a large population of children for different anatomical regions and age groups and to publish for the first time large population data regarding the rate of non-union per fracture in children.
Method
A large population was needed as the incidence of non-union in children is considered to be so low. In Scotland every child admitted as an inpatient (including day case) to hospital is coded on discharge according to its diagnosis using the ICD-10 classification. The paediatric population in Scotland has been stable in both size and migration statistics [1] making it a good population for the study. The data is collected centrally by ISD Scotland (Information Services Division, a department of NHS Scotland) and can be obtained upon request.
The non-union and fracture data for each patient is available according to age (5 year age groups), sex, anatomical distribution (as coded by ICD-10), individual hospital, health board and financial year.
As non-unions by definition require intervention in order to heal each treated case of non-union has an inpatient episode that is recorded and coded. Therefore the ISD data provides a good estimate of the non-union figures. However, as many children’s fractures are treated conservatively and are only seen in the outpatient setting their data is not captured by the ISD (inpatient) dataset. A previous study in Edinburgh [2] recorded and categorised every inpatient and outpatient paediatric fracture in Lothian (a defined region of Scotland with its own health board). Using the total fracture data from Lothian and the ISD inpatient numbers for both Lothian and the rest of Scotland it was possible to calculate the ratio of inpatient to total patient fracture numbers in Lothian children. This ratio was then applied to the rest of the Scottish paediatric inpatient figures, thereby calculating the total number of fractures in Scottish children.
The anatomical groupings in which the fresh fracture data was recorded was relatively detailed using the ICD-10 system, however the non-union data had a far more limited range of coding options. For example non-unions of the foot were not separated from non-unions of the ankle. To enable direct comparison, the fresh fractures were arranged into the same anatomical groups as the non-unions.
Results
The incidence of non-union and fractures in Scotland (Tables 1, 2, 3, 4, 5; Chart 1)
Over a 5-year period (2005–2010) in Scotland there were 180 children under the age of 15 years treated for non-union (60.6 % in males, 39.4 % in females), in the same period there were 424 treated fracture non-unions between the ages of 15 and 19 years (71.9 % and 28.1 % male and female respectively in the under 20 age group). There was a small rise with age in the number of non-unions under the age of 15, with males having a consistently higer number that females with a sharp rise in the older teenage age group, particularly the males. There were almost twice as many non-union in the upper limb (94) than in the lower limb (57) in those under the age of 15 (reflecting the higher total number of fractures in the upper limb). There were almost three times as many NU’s in the older teenager group (168 upper limb and 59 lower limb) compared to those 14 years and under. The forearm accounted for 44 % of all NU’s up to the age of 16 years, followed by the tibia (20 %), foot and ankle (8 %) and humerus (5.5 %).
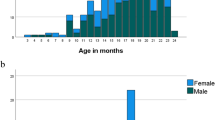
Using the ISD fracture data and applying the corrective ratio there were 92,201 fractures in the 0–14 year age group (161,068 in the 15–19 year olds) treated in Scotland between 2005 and 2010 resulting in an overall fracture incidence of 2,158 per 100,000 per annum in children (Table 4; Chart 1). The incidence of fractures in children increases through childhood, with a steady rise in each 5-year age group, starting at around 1 % risk in the under 5’s, 2 % in the 5–9 year olds and 3 % in the 10–14 year olds. The incidence in boys remains consistently higher than that in girls with a widening gap in the teenage years, peaking at 5 % in the older male teenagers.

The mean number of fractures sustained per 100 children per year (2005–2010) according to age
The risk of non-union per fracture (Table 6; Charts 2, 3, 4)
The overall rate of non-union per fracture in those younger than 15 years of age was 1 in 512 fractures (0.2 % risk per fracture). The risk of non-union per fracture remained consistently low in all age groups for both boys and girls under the age of 15 years. For every fracture in the 0–14 age group the risk of non-union was between 0.001 and 0.003. In the older teenage group (15–19 years) the risk remained low in females at 0.002 per fracture (1 in 528) but in the male it was higher at 0.005 per fracture (1 in 222 fractures).

The risk of non-union per fracture according to age and sex

The risk of non-union per fracture in the upper and lower limbs according to age

The relative anatomical distribution of non-union per fracture according to age
As Chart 3 illustrates when the data was divided into the upper and lower limb, the risk of non-union per fracture was far greater in the lower limb compared to the upper limb in those younger than 15, however in the 15–19 year age group the number of upper limb non-unions per fracture increased considerably (and the lower limb figures fell) to marginally exceed the risk of NU in the lower limb (Table 7).
Chart 4 displays the anatomical distribution of NU per fracture according to its relative frequency. The site with the greatest risk of non-union was the tibia, this risk increased consistently with age, peaking at 1.5 % risk per fracture (1 in 65) in the 15–19 age group. Foot and ankle non-union remained very low through out; measuring 0.2 % risk per fracture at its peak in the 5–9 year olds. Similar figures were seen for the shoulder (clavicle and scapula), peaking at 0.18 % in the 15–19 age group and 0.05 % or less in those younger than 15. The NU rate per fracture in the humerus remained at 1 in 500 or more fractures in those under the age of 15 years, in the older teenagers the rate was 1 in 85 fractures was likely to develop a non-union. NU of the forearm followed a similar trend to the humerus with a negligible risk in childhood but almost 2 % risk in the 15–19-year-olds.
Discussion
The risk of non-union in children is rare with only around 1 in 500 fractures not uniting (0.002 risk per fracture). There are no other non-union rates published in the literature apart from a handful of case series and those looking at particular anatomical sites [3–5].
Shrader et al. [6] in 2009 described a consecutive series of 43 paediatric non-unions over a 15 year period in those under the age of 15 years. The total number of fractures during this period was not recorded so they were not able to calculate the non-union case per fracture but as with our series they found more non-unions in the upper limb, especially in boys, with an average age of 9 years. Arslan et al. [7] reported 26 non-unions predominately in the lower limb non-union (22 lower to 4 upper). The average age was 9 years. Lewallen et al. [8] published a series of 30 paediatric non-unions over a 10 year period with a male lower limb predominance, peaking at 13 years of age. However none of these studies were able to compare their non-union numbers to their population size or fracture numbers. Studies of open tibial fractures in children [3, 4] have suggested that non-union risk was related to increasing age and did not occur in the under 6 year old age group. In our study the 0–4 year age group had the lowest number of non-unions, 31 (within which 5 were tibial) over a 5 year period in a 276,164 population of 0–4 year olds, however the incidence of fracture was also very low in that population group resulting in a similar risk of non-union per fracture to those up to the age of 15.
We have performed a similar study in the adult Scottish population, the overall risk for non-union in adult fractures was 1.43 %, ranging from 0.25 to 5.77 % (males 1.54 % and females 1.31 % risk) (currently unpublished data). This is 7.3 times higher than it is in children. The age group with the greatest risk of NU was in the 30–44-year-old age group at 1.99 %, ten times more likely than in children. Unlike the paediatric population the highest rate of non-union in adults was found in the clavicle at 5.77 % (>8 % in some age groups), but closely followed by the tibia at 5.17 % (peaking at 7.16 % in 30–44-year-olds) (currently unpublished data). Similar to children the foot/ankle and hand had the lowest risk of developing a NU per fracture in almost all the adult age groups (0.91 and 0.25 %, respectively).
A weakness in this study is that sum total fracture number is extrapolated from a regional figure, however the benefit of using Lothian data is that it is a captured orthopaedic population with all those age 14 years and under being treated in one single hospital and those 15 years and above seen in another single hospital, the population is also stable and representative of the rest of the Scottish population. Furthermore there is the possibility of a few fracture non-unions going clinically undetected or being treated conservatively, e.g.- lateral condyle fractures, this is only likely to be the situation if there was no adverse clinical sequelae or patient symptoms. Given that there were only 180 non-unions treated over a 5-year period and 92,201 fractures sustained, a non-union underestimation of 10 % would not change the overall risk per fracture by more than 0.0002 to a non-union risk of 0.21 %. Unfortunately due to the nature of the ICD-10 classification system we were unable to further sub classify the anatomical distribution of the data—for example the risk for different fracture configurations around the elbow.
The infrequent nature of non-union as a complication in children, as confirmed by this study, requires a large population to calculate the relative risk. Achieving more accurate data and results without setting up a multicentre/national study is unlikely, this study shows that the need to resource such a study is not necessary.
Conclusion
This study is the first to estimate the incidence of non-union in children. It has looked at the overall rate of non-union and fractures in a large population (almost 1.2 million) of children and young adults. The risk of non-union per fracture in those under the age of 15 is approximately 1 in 500 for both boys and girls; in the 15–19 year age group the risk of non-union per fracture is approximately 1 in 500 in girls and 1 in 200 for boys. It remains a rare complication.
References
Scotland’s Population (2010) The registrar general’s annual review of demographic trends, 156th edn. Edinburgh
Rennie L, Court-Brown CM, Mok JY, Beattie TF (2007) The epidemiology of fractures in children. Injury 38(8):913–922. doi:10.1016/j.injury.2007.01.036
Kreder HJ, Armstrong P (1995) A review of open tibia fractures in children. J Pediatr Orthop 15(4):482–488
Grimard G, Naudie D, Laberge LC, Hamdy RC (1996) Open fractures of the tibia in children. Clin Orthop Relat Res 332:62–70
Duteille F, Dautel G (2004) Non-union fractures of the scaphoid and carpal bones in children: surgical treatment. J Pediatr Orthop B 13(1):34–38 pii:00009957-200401000-00007
Shrader MW, Stans AA, Shaughnessy WJ, Haidukewych GJ (2009) Nonunion of fractures in pediatric patients: 15-year experience at a level I trauma center. Orthopedics 32(6):410. doi:10.3928/01477447-20090511-11
Arslan H, Subasy M, Kesemenli C, Ersuz H (2002) Occurrence and treatment of nonunion in long bone fractures in children. Arch Orthop Trauma Surg 122(9–10):494–498. doi:10.1007/s00402-002-0439-y
Lewallen RP, Peterson HA (1985) Nonunion of long bone fractures in children: a review of 30 cases. J Pediatr Orthop 5(2):135–142
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Mills, L.A., Simpson, A.H. The risk of non-union per fracture in children. J Child Orthop 7, 317–322 (2013). https://doi.org/10.1007/s11832-013-0521-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11832-013-0521-8