
Abstract
Purpose
This study was designed to assess the relationship between skeletal and chronological ages among current American adolescents using the Greulich and Pyle atlas for skeletal age determination.
Materials and methods
We used the Greulich and Pyle atlas to prospectively determine skeletal age in a group of 138 otherwise healthy American adolescents from 12 to 18 years of age. 62 males and 76 females were enrolled in this cohort. Paired Studentt-tests were used to statistically compare the skeletal and chronological ages in this population. Subgroup analysis examined the effect of gender on differences between chronologic age and skeletal age.
Results
For the entire cohort, mean skeletal age was significantly greater than chronological age (mean 0.80 years, P < 0.01). In 29 cases (21%) the skeletal age was at least 2 years greater than the chronologic age. Among females, such cases with marked discrepancy occurred exclusively in those chronologically between 12 and 15 years of age (P < 0.01). Males demonstrated a 2-year or greater discrepancy more commonly than females (26 vs. 17%). In males, 2-year discrepancies were equally likely across chronologic ages (P = 0.82).
Conclusions
Current American adolescents are significantly more mature by skeletal age, as determined by the Greulich and Pyle method, than their chronological age would suggest. The skeletal ages of females are most likely to markedly exceed chronologic age between the ages of 12–15 years.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
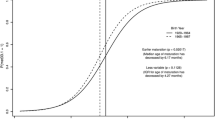
The assessment of skeletal maturation in children and adolescents is necessary in clinical practice to determine the timing of varied interventions such as growth hormone administration and surgical epiphysiodesis. One of the most common techniques used to detect differences between skeletal age and chronologic age is the Greulich and Pyle method. This technique, developed in 1959, is based on a reference population of above-average social class adolescents from the 1930s [1]. Utilizing this technique, a postero-anterior skeletal radiograph of the subject’s left hand is compared to an atlas of “normal” radiographs to assign a skeletal age. Specifically, the reviewer assesses similarities in epiphyseal development and physeal appearance between the subject’s radiograph and the reference standards for gender-specific skeletal maturity in the atlas. This technique assumes that the skeletal development of the hand and wrist is representative of the individual’s overall skeletal maturation [1, 2].
It is unknown whether the skeletal maturation of current American adolescents is similar to the cohort which provided the basis for the Greulich and Pyle atlas. This study was performed to test the hypothesis that current American adolescents are maturing faster than predicted by the Greulich and Pyle atlas. Our null hypothesis was that the chronologic age would match the skeletal age.
Materials and methods
After Institutional Review Board (IRB) approval, subjects were recruited from the clinic population of the principal investigator and collaborators at a pediatric orthopedic hospital. One hundred thirty-eight adolescents between the ages of 12 and 18 years comprised this prospective cohort, with 62 males (45%) and 76 females (55%). Subjects were predominately Caucasian (n = 116) with a minority of African American (n = 10), Hispanic (n = 2), Asian (n = 1), and other (n = 9). Potential subjects were excluded if they had either a pre-existing diagnosis of, or were being evaluated for, any genetic syndrome, growth abnormality, congenital abnormality of the upper extremity, or history of any upper extremity fracture or pain.
The purpose of the study, which was performed in conjunction with several others requiring isolated, standardized hand radiographs, was explained to the subjects and parents, and informed consent was obtained. A single posterior–anterior radiograph of the left hand and wrist was taken to determine skeletal age. All films were of satisfactory quality, and we did not exclude any films from analysis. The radiographs were de-identified of any personal health information, and each participant’s hand radiograph was coded for chronological age to allow further analysis. Race data on individual subjects were not recorded per IRB stipulation. The reviewer was blinded to the chronologic age of the subjects but was aware of gender. A single attending orthopaedic surgeon trained in the Greulich and Pyle method analyzed all radiographs to determine skeletal age [1]. The technique, as detailed in the atlas, begins with a comparison of the radiograph in question with an estimated chronological age comparison in the atlas. The reviewer then compares the radiograph to nearby chronological age radiographs to allow the best match. Differing features are used to determine the best chronological age fit, including physeal development, fusion of epiphyses, and bone morphology. A second physician, also trained in the Greulich and Pyle technique, evaluated a subset of 20 radiographs that were randomly selected to confirm inter-rater reliability.
Analysis of data
Data analysis was performed using the SPSS statistical software (version 15.0.1, SPSS, Inc., Chicago, IL, USA). Tests of frequency were done to evaluate overall skeletal age and chronological age as well as means at each age point. The paired Students t-test was utilized to compare mean skeletal age versus chronologic age for the cohort stratified by gender. Chi-square tests of independence analyzed the relationship between chronologic age and the presence of discrepancy between the chronologic and skeletal ages of at least 2 years. Spearman correlations were determined for the relationship of chronologic age to skeletal age by gender. The intra-class correlation coefficient for skeletal age determined by two independent reviewers was utilized to assess inter-rater reliability. Significance was set at α = 0.05.
Results
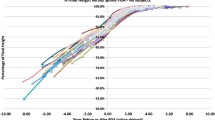
For the entire cohort, mean skeletal age was significantly greater than chronological age (mean 0.80 years, P < 0.01). The mean chronological age for females was 14.36 years (standard deviation 1.92 years) with a skeletal age mean of 15.0 years (standard deviation, 1.98 years). The mean skeletal age was greater than the mean chronological age in females, with a 0.66-year difference (P < 0.001). Forty-one of the 76 females (54%) had a more advanced skeletal age than chronological age, with 13 (17%) of these demonstrating a 2-year or greater difference. As seen in Table 1, among females, the presence of skeletal age found to be at least 2 years advanced beyond chronologic age was significantly more likely among those chronologically 12–15 years of age (P < 0.01). Twenty-seven females (36%) had a skeletal age equal to their chronological age, and 8 females (11%) had a skeletal age less than their chronological age. In no case was the skeletal age determined to be at least 2 years less than chronologic age. Skeletal age correlated significantly (P < 0.001) with chronologic age across the age spectrum (r s = 0.890).
Mean chronological age for males was 14.3 years (standard deviation, 1.73 years) with a skeletal age mean of 15.3 years (standard deviation, 2.11 years). The mean skeletal age was more advanced than the mean chronological age in males, with a 0.98-year difference (P < 0.001). Forty-eight of the 62 males (77%) had a higher skeletal age than chronological age, with 16 (26%) of these demonstrating a 2-year or greater difference. The data failed to indicate any correlation between chronologic age range and the presence of skeletal age exceeding chronologic age by at least 2 years (P = 0.82); suggesting that the 2-year discrepancy is possible across this entire population (Table 2). Nine males (15%) had a skeletal age equal to their chronological age and 5 had a skeletal age less than their chronological age (8%). In no case was the skeletal age determined to be at least 2 years less than the chronologic age. Skeletal age and chronologic age were significantly correlated (P < 0.001) across the age spectrum (r = 0.879).
We also assessed inter-observer reliability. The original mean skeletal age for 20 randomly chosen radiographs was 14.95 years, with a standard deviation of 2.04 years. A second physician evaluated the same 20 radiographs and demonstrated a mean skeletal age of 15.15 years with a standard deviation of 1.98. The difference between the two physicians was not statistically significant (P = 0.1). The intra-class correlation for these twenty measures was 0.982, indicating substantial inter-observer reliability between individual reads for each radiograph.
Discussion
There have been several reports in the last 20 years assessing trends in the maturation of children and adolescents [3–7]. Each investigation has examined cohorts of subjects to compare skeletal age and chronologic age within populations hypothesized to differ from the original cohort that comprised the basis of the Greulich and Pyle atlas. These new populations have included subjects from various countries and of differing races. Several of these investigations have focused on the “applicability” of the Greulich and Pyle atlas to the new populations of interest. These data have not yielded any uniform conclusions.
Van Rijn et al. [7] and Groell et al. [3] demonstrated a high correlation between skeletal age and chronological age in European cohorts of young males and females, and concluded that the Greulich and Pyle atlas was still applicable for their populations. Studies in the United States from 1993 to 2001 have reported an increased discrepancy between the chronological and skeletal age among the racially diverse populations, and have questioned the continued applicability of the atlas [4–6]. The data in these previous reports vary, and the report by Loder et al. [4] is most comparable to ours. They reported that, over childhood and adolescence, skeletal age exceeded chronological age by 0.31 years (±1.04 years) in girls and by 0.8 years (±1.13 years) in boys. Adolescent boys and girls together demonstrated a skeletal age exceeding chronological age by 0.41 years (±1.21 years). Subgroup analysis showed larger differences based on race. Our skeletal age–chronological age discrepancy was approximately double, with skeletal age exceeding chronological age by 0.8 years.
The difference between skeletal and chronological ages in our largely adolescent population is higher than the differences in most previous reports. Furthermore, 21% of our subjects had a 2-year or greater difference, a gap that clearly affects surgical and medical treatment. However, this gap should not be surprising, as patterns of maturation change over time, and Himes [8] suggested that skeletal maturation would increase by approximately 0.22–0.66 years per decade. Based on our findings, together with other reports, the current gap between skeletal and chronological ages is on the lower end of this possible spectrum.
Despite a more rapid skeletal maturation and a variability in maturation rates based on race and other factors, there is no indication that specific bony maturation patterns have changed since the Greulich and Pyle atlas was introduced. Our data confirm that skeletal age and chronological age remain highly correlated. We believe that these data, indicating advanced skeletal age beyond chronologic age in a current cohort of American adolescents, represent a note of caution for those planning medical or surgical treatment for growth abnormalities. We still find the Greulich and Pyle atlas useful, and believe that the accurate assignment of skeletal age is more important now than ever before, as today chronological age is less likely to accurately represent remaining skeletal growth.
There are several weaknesses of this investigation. First, despite a similar number of participants to previous investigations, the number of males and females for each age group is limited [5, 9, 10]. Therefore, it is likely that, with an increased number of subjects, the absolute differences between skeletal age and chronologic age may have varied, but we believe the overall trends would remain similar to those identified in these 138 subjects. Second, we recognize that the gap in skeletal and chronological ages is affected by numerous factors not assessed in this manuscript, including race, socioeconomic status, and nutritional status. These are more difficult to assess and would require a dramatically larger number of subjects; furthermore, our clinic population may not be amenable to an assessment of racial disparities. Additionally, the authors note that the chronologic age of subjects was assessed in yearly increments without “rounding up” to the next advanced year. This introduces a slight discrepancy with the Greulich and Pyle method, as some years are broken into 6-month intervals. As these 6-month intervals are inconsistently included in the atlas, any uniform treatment of chronologic age would introduce some discrepancy. As our current data analysis would tend to bias toward the subjects that appear slightly more skeletally mature, we focused on and reported on those subjects of each gender in which skeletal age exceeded chronologic age by at least 2 years. Finally, in this study, a single senior reviewer evaluated skeletal age for all 138 participants. This attending physician was trained in the Greulich and Pyle method and regularly utilizes this technique; furthermore, on re-evaluation of a subgroup of the X-rays by an independent physician, similar results were found, with a high reliability confirmed. We presume that this review with a subset analysis for inter-rater reliability is sufficient given the exceptionally high previously documented inter- and intra-rater reliability of senior evaluators using the Greulich and Pyle method [4–7].
In conclusion, this investigation demonstrated an unexpectedly high percentage of otherwise normal American adolescents born between 1989 and 1996 who demonstrate skeletal maturity exceeding chronologic age. Females between the chronologic ages of 12 and 15 are most likely to demonstrate a discrepancy of at least 2 years between skeletal and chronologic age, while males demonstrate this potential throughout adolescence.
References
Greulich W, Pyle S (1959) Radiographic atlas of skeletal development of the hand and wrist. Stanford University Press, Stanford
Hansman CF, Maresh MM (1961) A longitudinal study of skeletal maturation. Am J Dis Child 101:305–321
Groell R, Lindbichler F, Riepl T, Gherra L, Roposch A, Fotter R (1999) The reliability of bone age determination in central European children using the Greulich and Pyle method. Br J Radiol 72:461–464
Loder RT, Estle DT, Morrison K, Eggleston D, Fish DN, Greenfield ML, Guire KE (1993) Applicability of the Greulich and Pyle skeletal age standards to black and white children of today. Am J Dis Child 147:1329–1333
Mora S, Boechat MI, Pietka E, Huang HK, Gilsanz V (2001) Skeletal age determinations in children of European and African descent: applicability of the Greulich and Pyle standards. Pediatr Res 50:624–628
Ontell FK, Ivanovic M, Ablin DS, Barlow TW (1996) Bone age in children of diverse ethnicity. AJR Am J Roentgenol 167:1395–1398
van Rijn RR, Lequin MH, Robben SG, Hop WC, van Kuijk C (2001) Is the Greulich and Pyle atlas still valid for Dutch Caucasian children today? Pediatr Radiol 31:748–752
Himes JH (1984) An early hand-wrist atlas and its implications for secular change in bone age. Ann Hum Biol 11:71–75
Koc A, Karaoglanoglu M, Erdogan M, Kosecik M, Cesur Y (2001) Assessment of bone ages: is the Greulich–Pyle method sufficient for Turkish boys? Pediatr Int 43:662–665
Rikhasor RM, Qureshi AM, Rathi SL, Channa NA (1999) Skeletal maturity in Pakistani children. J Anat 195(Pt 2):305–308
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Calfee, R.P., Sutter, M., Steffen, J.A. et al. Skeletal and chronological ages in American adolescents: current findings in skeletal maturation. J Child Orthop 4, 467–470 (2010). https://doi.org/10.1007/s11832-010-0289-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11832-010-0289-z