
Abstract
Study design
Outcome investigation to verify the internal consistency, reproducibility and validity of the adapted Chinese version of the Scoliosis Research Society-22 (SRS-22) questionnaire for measuring health-related quality of life (HRQoL) in children with idiopathic scoliosis.
Objective
To develop this questionnaire for the outcome measurement in treating Chinese adolescents with idiopathic scoliosis and evaluate its metric qualities.
Summary of background data
The SRS-22 questionnaire has proven to be a valid instrument for clinical assessment of patients with idiopathic scoliosis and has been successfully translated into Spanish and Turkish. In most developing countries, however, quality of life and psychological health have been poorly described when treating children with idiopathic scoliosis.
Methods
Trans-cultural adaptation of the SRS-22 questionnaire was carried out according to the International Quality of Life Assessment Project guidelines. The final version was approved by a committee of experts. The questionnaire was completed by 86 adolescents with idiopathic scoliosis who had been treated with a brace; this included 11 males and 75 females, aged from 10 to 18 years (mean 13.9 years). Curve magnitude ranged from 25° to 45° (mean 35.6°). A subgroup of 30 patients completed the questionnaire again in 3 or 4 weeks.
Results
Five common factors were acquired from factorial analysis, and the cumulative contribution ratio was 67.66%. The overall alpha coefficient of the questionnaire was 0.88. Coefficients for individual domains were as follows: function/activity, 0.70; pain, 0.80; self-image, 0.80; mental health, 0.88; and satisfaction, 0.81. The questionnaire as a whole had a test–retest correlation coefficient of 0.97. Test–retest correlation coefficients for individual domains were as follows: function, 0.85; pain, 0.96; self-image, 0.96; mental health, 0.95; and satisfaction, 0.91.
Conclusion
The Chinese version of the SRS-22 questionnaire is eligible in terms of reliability and validity, and can be used to measure HRQoL for adolescent idiopathic scoliosis patients in Mainland China.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The health-related quality of life (HRQoL) has frequently been ignored in evaluating both the spine deformity and the effectiveness of treatment in patients with idiopathic scoliosis [1–4]. Furthermore, there has been no questionnaire about outcome assessment, which is accepted world-wide for evaluating such patients, and the effectiveness of treatment, especially in most developing countries, where the health-related conditions such as quality of life, psychological health and healthcare systems are poorly described. Haher et al. designed a simple, practical and disease-specific outcome instrument to assess patients with idiopathic scoliosis. It contains seven domains and has a better score distribution, internal consistency and concurrent validity than Short Form 36 (SF-36), another well-recognized, validated instrument for generic measurement of quality of life [5]. After further modifications to this instrument, Asher et al. developed a new questionnaire consisting of 22 items—the Scoliosis Research Society 22 Patient Questionnaire (SRS-22 PQ)—which has been widely used in English-speaking countries and several non-English-speaking countries [6–11]. However, a trans-cultural adaptation of the contents has been necessary for its application in those non-English-speaking countries.
The purpose of this study was to determine metric qualities of the Chinese version of the SRS-22 questionnaire by factorial analysis and using an assessment of its internal consistency and test–retest reproducibility.
Materials and methods
The SRS-22 questionnaire consisting of 22 questions is separated into 5 domains: function/activity, 5 items (5, 9, 12, 15, 18); pain, 5 items (1, 2, 8, 11, 17); self-perceived image, 5 items (4, 6, 10, 14, 19); mental health, 5 items (3, 7, 13, 16, 20); and satisfaction with treatment, 2 items (21, 22). Each item is scored from 1 (the worst) to 5 (the best). The total sum score of each domain ranges from 5 to 25, except for the satisfaction domain, which ranges from 2 to 10. The first four domains have a maximum subtotal score of 100; the maximum total score is 110 by adding the satisfaction domain.
According to the guidelines of the International Quality of Life Assessment (IQOLA) Project [12–15], the translations were performed by two native Chinese speakers and two native English speakers—this involved forward and backward translations of the questionnaire and cross-cultural comparisons. The first step was that the original English version of the questionnaire (according to the SRS official website) was translated into Chinese independently by two Chinese-speaking translators. With the modifications, a preliminary version of forward translation was produced and approved. This was then referred to two other bilinguals, who evaluated its quality to develop a revised preliminary version of forward translation. Then this forward translation was back translated into English independently by two English-speaking translators. A committee of experts in spine deformity was organized to evaluate the quality for each item of the translated version, and the final version was produced by consensus of the committee. The final Chinese version of the questionnaire can be consulted in Appendix A of the Electronic Supplementary Material.
This investigation was carried out according to the “Ethics Principles for Medical Research Involving Human Subjects” (World Medical Association Declaration of Helsinki, Geneva, 2000). The questionnaires of SRS-22 Chinese version were completed by 86 patients with idiopathic scoliosis and bracing treatment. The patients or their legal guardians provided informed consent to participate, and the study was approved by the University Human Research Committee. There were 75 females and 11 males with a mean age of 13.9 years (range 10–18 years). Cobb’s angles of the major curve ranged from 25° to 45° (mean 35.6°). All patients completed the questionnaire by themselves, and a random subgroup of 30 patients filled out the questionnaire again 3–4 weeks after the first test.
SPSS 10.0 package software was used for the statistical analyses. Reliability was evaluated by internal consistency, which was determined by Cronbach’s alpha coefficient, and reproducibility, which was determined by the correlation coefficient. Structure validity was assessed by factorial analysis.
Results
Reliability analysis
As is shown in Table 1 [with date of English and Spanish versions from Spine 29(15):1676–1680, 2004], the overall alpha coefficient and coefficients for each corresponding domains of the questionnaire are as follows: total score 0.88; function/activity, 0.70; pain, 0.80; self-image, 0.80; mental health, 0.88 and satisfaction, 0.81.
Guttman split-half tests for five domains were performed independently, and for individual domains were: function/activity, 0.51; pain, 0.77; mental health, 0.74; self-image, 0.81; and satisfaction, 0.81.
After a reproducibility test (Table 2), intraclass correlation coefficients of the overall questionnaire and every domain were: overall, 0.97; function, 0.85; pain, 0.96; self-image, 0.96; mental health, 0.95; and satisfaction, 0.91
Validity analysis
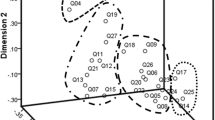
Five common factors were acquired from factorial analysis, and the cumulative contribution ratio was 67.66%. As shown in Table 3, each domain had a fairly good structure validity, in accordance with their theoretical structure, except for the function/activity domain, which was affected by item 15. Table 4 provides the results of item-to-domain correlation analyses.
Comparison of scores between Chinese version and English original version
Table 5 shows the mean of the adapted and the original versions for each domain.
Table 6 presents the maximum and minimum scores of the adapted version, the floor effect and the ceiling effect for individual domains in both the adapted and original versions.
Discussion
It has been necessary progress to measure HRQoL when treating idiopathic scoliosis in children and adolescents. The SRS-22 questionnaire has proven to be a valid instrument for clinical assessment of patients with this condition and has been translated and validated in Italian, Spanish, Turkish and even Chinese languages [11–14]. However, the same language does not represent similar culture. It is thus necessary to adapt these tools not only for use in non-English-speaking countries, especially in most developing countries where HRQoL and psychological conditions are frequently ignored, but also for use in different cultures and even healthcare systems. This study aimed to adapt this tool in Mainland China. In order to assure equivalence between these versions and rule out side effects of cultural and linguistic discrepancy, the trans-cultural adaptation of the SRS-22 from English to Chinese was performed according to the IQOLA Project guidelines.
In this study, reliability analysis showed that the internal consistency of the questionnaire was adequate, either in total score or in individual domain, which had a Cronbach’s alpha coefficient beyond 0.70. This is quite similar to that of the original versions. Item-to-domain correlation analyses demonstrated correlation coefficients greater than 0.6 for all the items. The analysis of construct validity showed that five common factors from factorial analysis were in accordance with their theoretical structure—except the function/activity domain—and the cumulative contribution rate was 67.66%. It is obvious that there is a cultural variable, such as differences in healthcare payment schemes, which has a considerable effect on question no. 15 (relating to financial considerations), between developed countries and Mainland China. Asher et al. [16] mentioned this issue in their latest study, and similar phenomena were also found in other trans-cultural adaptations of the SRS-22 questionnaire [10, 11]. This occurs even where there are similar linguistics; for example, the healthcare system in Mainland China is quite different from that in Hong Kong China. The scoliosis treatment usually takes a long period of time and most patients have to rely on their own for the expenditure of medical care in Mainland China. Traveling to the medical centers for follow-up and brace making cost a lot. Many of our patients came to visit us from hundreds of kilometers away. However, most of the patients take the welfare healthcare service for their medical treatment in Hong Kong SAR.
Compared with Asher’s results, scores for several domains were significantly lower than those of the original version (Table 5), mainly because the braced patients had a poorer self-image and mental health, and a reduced activity level. Cheung et al. also found that bracing had a greater negative impact on the quality of life, especially on a function or activity level in patients with mild curves. In patients with severe curves, bracing did not seem to have as great an effect on the quality of life. They suggested that the utility of the SRS-22 questionnaire as a HRQoL questionnaire should take into account not only the physical health of the patient, but also the emotional and psychosocial factors previously overlooked in traditional outcome studies [17]. This study demonstrated that the floor and ceiling effects in the Chinese version are very similar to those of the English original, with the exception of satisfaction with treatment.
The effect of bracing on the quality of life of individuals has not been well described. Some presumed that it should be a negative impact. This may be related to the use of different kinds of braces, different bracing regimes and cultural differences in patients’ abilities to accept bracing. In Mainland China, 80% of the population lives in rural areas. Interestingly, although not concluded in this study, we found that, in most cases, the patients living in rural areas were more compliant with bracing. However, the patients in urban areas were more concerned about their daily function and self-image and less compliant. We take adolescence as the period of not only physical growth but also psychological instability. Therefore, more attention should be paid to both the physical and psychological impact of bracing among adolescents from different populations. It is proposed that psychological intervention should be introduced along with bracing treatment.
In summary, the Chinese version of the SRS-22 questionnaire has eligible reliability and validity in comparison with the English original version. It can be applied to measure the HRQoL of Chinese adolescent idiopathic scoliosis patients. Given cultural differences between developed countries and developing countries, such as Mainland China, especially under healthcare payment policies, some questions especially with regard to function/activity domain should be revised. Further studies are required for the better adaptation to this particular situation.
Conclusion
The Chinese version of the SRS-22 outcome instrument has excellent reliability and validity in comparison with the original English one. This study suggests that the adapted Chinese version of this questionnaire be apparently equivalent to the original. It can be used to measure the HRQoL for adolescent idiopathic scoliosis patients in Mainland China. Linguistic translation and cultural and social-economic adaptation are essential in any attempt to use a HRQoL questionnaire across lands.
Key points
-
The HRQoL has become a unique aspect for evaluating both spine deformity itself and the effectiveness of treatment. However, some difficulties still exist when its application is performed in different cultures, especially in most developing countries, where the health-related conditions such as quality of life, psychological health and healthcare system have been poorly described.
-
The SRS-22 HRQL questionnaire has been shown to be a valid instrument for clinical assessment of patients with idiopathic scoliosis and has been successfully translated into some other languages.
-
Trans-cultural adaptation of the SRS-22 questionnaire in Mainland China was carried out according to the IQOLA Project guidelines. The final version was approved by a committee of experts. The questionnaire was finished by 86 adolescent idiopathic scoliosis patients who were braced—this included 11 males and 75 females, aged 10 to 18 years (mean 13.9 years). Curve magnitude ranged from 25° to 45°(mean 35.6°). A randomized subgroup of 30 patients completed the questionnaire again in 3 to 4 weeks. Reliability and validity analyses were performed.
-
The Chinese version of the SRS-22 questionnaire has eligible reliability and validity in comparison with the English original version. It can be used to measure the HRQoL for adolescent idiopathic scoliosis patients in Mainland China. Given the differences in culture between developed and developing (such as China) countries, especially with regard to healthcare payment policies, some questions, especially those concerning function/activity domain, should be revised in further studies.
References
Matsunaga S, Hayashi K, Naruo T et al (2005) Psychologic management of brace therapy for patients with idiopathic scoliosis. Spine 30(5):547–550
Danielsson A, Wiklund I, Pehrsson K et al (2001) Health-related quality of life in patients with adolescent idiopathic scoliosis: a matched follow-up at least 20 years after treatment with brace or surgery. Eur Spine J 10:278–288
Noonan KJ, Dolan LA, Jacobson WC et al (1997) Long-term psychosocial characteristics of patients treated for idiopathic scoliosis. J Pediatr Orthop 17(6):712–717
Freidel K, Reichel D, Steiner A et al (2002) Idiopathic scoliosis and quality of life. Stud Health Technol Inform 88:24–29
Haher TR, Gorup JM, Shin TM et al (1999) Results of the Scoliosis Research Society instrument for evaluation of surgical outcome in adolescent idiopathic scoliosis: a multicenter study of 244 patients. Spine 24(14):1435–1440
Asher MA, Lai SM, Burton DC (2000) Further development and validation of the Scoliosis Research Society (SRS) outcomes instrument. Spine 25(18):2381–2386
Asher M, Min Lai S, Burton D et al (2003) The reliability and concurrent validity of the Scoliosis Research Society-22 Patient Questionnaire for idiopathic scoliosis. Spine 28(1):63–69
Asher M, Lai S, Burton D et al (2003) Scoliosis Research Society-22 Patient Questionnaire responsiveness to change associated with surgical treatment. Spine 28:70–73
Monticone M, Carabalona R, Negrini S (2004) Reliability of the Scoliosis Research Society-22 Patient Questionnaire (Italian version) in mild adolescent vertebral deformities. Eura Medicophys 40(3):191–197
Bago J, Climent JM, Ey A et al (2004) The Spanish version of the SRS-22 patient questionnaire for idiopathic scoliosis: transcultural adaptation and reliability analysis. Spine 29(15):1676–1680
Alanay A, Cil A, Berk H et al (2005) Reliability and validity of adapted Turkish Version of Scoliosis Research Society-22 (SRS-22) questionnaire. Spine 30(21):2464–2468
Beaton D, Bomardier C, Guillemin F et al (2000) Guidelines for the process of cross-cultural adaptation of self-report measures. Spine 25:3186–3191
Bullinger M, Alonso J, Apolone G et al (1998) Translating health status questionnaires and evaluating their quality: the IQOLA project approach. J Clin Epidemiol 51:913–923
Cheung KM, Senkoylu A, Alanay A et al (2007) Reliability and concurrent validity of the adapted Chinese version of Scoliosis Research Society-22 (SRS-22) questionnaire. Spine 32(10):1141–1145
Guillemin F, Bombardier C, Beaton D (1993) Cross-cultural adaptation of health-related quality of life measures: literature review and proposed guidelines. J Clin Epidemiol 46:1417–1432
Asher MA, Lai SM, Glattes RC et al (2006) Refinement of the SRS-22 health-related quality of life questionnaire function domain. Spine 31(5):593–597
Cheung KM, Cheng EY, Chan SC et al (2007) Outcome assessment of bracing in adolescent idiopathic scoliosis by the use of the SRS-22 questionnaire. Int Orthop 31(4):507–511
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
About this article
Cite this article
Zhao, L., Zhang, Y., Sun, X. et al. The Scoliosis Research Society-22 questionnaire adapted for adolescent idiopathic scoliosis patients in China: reliability and validity analysis. J Child Orthop 1, 351–355 (2007). https://doi.org/10.1007/s11832-007-0061-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11832-007-0061-1