
Abstract
Objectives
Cancer survivors can experience difficulties returning to and/or remaining at work. Sociodemographic, health and well-being, symptom burden, functional limitations in relation to work demands, work environment, and various work policies and procedures can be related to work function.
Methods
This study analyzed cross-sectional data of a sample of cancer survivors (n = 1,525) who were diagnosed and treated for various types of cancer. The data were obtained from a survey of cancer survivors collected by the LiveStrong Foundation. Using a cancer survivorship and work model proposed in 2010, this study used structural equation modeling to predict work ability (whether survivors reported lower work ability following cancer) and work sustainability (whether survivors had ever lost or left a job because of cancer, i.e., work retention). Potential predictors included health and well-being, symptom burden (e.g., fatigue, pain, and distress), cancer-related worry, worry about family’s cancer risk, functional impairment (i.e., physical, cognitive, and interpersonal), workplace support, and workplace problems.
Results
The overall model predicting work ability (CFI = 0.961, TLI = 0.952, and RMSEA = 0.027) indicated that a greater level of functional limitations (B = 5.88, p < 0.01) and workplace problems (B = 0.22, p = 0.05) were significantly related to lower levels of work ability. Structural equation modeling (CFI = 0.961, TLI = 0.952, and RMSEA = 0.027) also indicated that workplace problems was a significant predictor (B = 0.498, p < 0.001) of the likelihood of losing or leaving a job because of cancer.
Conclusions
Functional limitations and problems at work including poor treatment, discrimination, being passed over for promotion, and lack of accommodations were directly related to the ability to work. Problems at work were associated with lower work sustainability (work retention).
Implications for Cancer Survivors
Employed cancer survivors, health care providers, and employers need to be aware of the potential implications of limitations in function (e.g., physical, cognitive, and interpersonal/social) as it relates to ability to work. In many cases, these functional limitations are responsive to rehabilitation. Workplaces also need to be educated on how to better respond to the needs of cancer survivors at work.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background
The number of cancer survivors in the USA has surpassed 13 million, and 40 % of these survivors are of working age [1]. The successful transition back to work and maintenance of employment can be concerns for many of those survivors, because paid employment provides income, access to health insurance (in the USA), as well as self-identity, self-esteem, representation of an individual’s talents and abilities, and a basis for forming and maintaining social relationships [2]. However, many cancer survivors face difficulties in achieving optimal work outcomes. Employed breast cancer survivors, for example, experience higher levels of fatigue, depression, and cognitive limitations than noncancer comparison groups [3, 4], as well as greater work limitations [4]. Cancer survivors are more likely to be unemployed than healthy controls [5] and are more likely to file claims related to job loss or differential treatment because of workplace policies compared with workers with other medical conditions [6]. One study of cancer survivors in the USA found that while 92 out of 100 returned to work, 57 % of those reduced their working hours by more than 4 h/week and 56 % reported a change in their occupational role [7].
The cancer survivor’s health status, symptom burden, and limitations in function [8–11] have been related to return to work and perceived work ability. There is very little information on the interrelationships among these variables and their association with work outcomes. Understanding the complex relationships among these factors is necessary to better inform individual and system-level interventions to improve both employers’ and cancer survivors’ work outcomes.
Feuerstein and colleagues developed a conceptual model of cancer survivorship and work based upon existing research on occupational outcomes in cancer survivors and the field of work disability in general [12]. The model provided a theoretical framework that proposed relationships among health and well-being, symptom burden, and functional limitations in relation to work demands and work outcomes (return to work, work ability, and work sustainability) in individuals post-primary treatment for cancer. The model also proposed that the work environment can directly affect work outcomes. Factors such as sociodemographic characteristics and system-level policies, procedures, and economic variables were also proposed as potentially influencing return to work, work ability, and/or work sustainability.
The present study investigated the direct relationships among sociodemographic characteristics, health and well-being, symptom burden, functional impairment, and work environment, on work ability and work sustainability (work retention). Although return-to-work is well studied in cancer survivors, other work outcomes such as work sustainability are not as well understood and merit further study [12]. This study was designed to validate major elements of the cancer survivor and work model. Specifically, this study examined the interrelationships among multiple variables related to work ability and work sustainability in cancer survivors with a history of many types of cancers and cancer treatment exposures.
Methods
Data collection
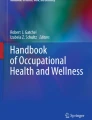
The data for the present study were obtained from the 2010 LiveStrong Foundation Survey, which was administered online and disseminated by the LiveStrong Foundation and collaborating partners from June 2010 to February 2011 [13]. The cancer survivors and work model [12] provided the overall structure for the analyses and items from the LiveStrong Foundation Survey were extracted to provide proxy measures for the various elements in the model as related to work ability and work sustainability (Fig. 1). The specific items listed in Fig. 1 were selected based on availability in the survey and face validity.

Factors related to limitations in work ability. Note: CFI = 0.96; TLI = 0.95; RMSEA = 0.027. ***p < 0.001
Participants
Inclusion criteria for the current analyses were: (1) prior diagnosis of cancer as an adult (age 18 or above), (2) completion of primary cancer treatment for the cancer (e.g., radiation therapy, chemotherapy, and/or surgery), (3) age 18–74 [14], (4) actively working at time of diagnosis or since diagnosis, (5) residing in the USA, and (6) ability to read English. Out of the original sample of 12,037 cancer survivors who completed the survey, 1,542 or 12.8 % met inclusion criteria for the current study. Participants indicated consent online before accessing the survey. The original survey was reviewed and approved by the Western Institutional Review Board. Participants were not compensated for completion of the survey. A data use agreement was completed between the investigators and the LiveStrong Foundation. Considering the absence of any identifiers in the dataset, this study was exempt by the Internal Review Board at the Uniformed Services University of the Health Sciences.
The final sample of 1,542 meeting inclusion criteria was compared with the full survey sample (N = 12,037) on demographic measures of age, gender, education, income, age at diagnosis, primary cancer site, treatment type, and time from end of primary treatment to survey completion. The groups did not differ on any of these variables except for time post-completion of primary treatment. A Wilcoxon signed-rank test found a significant difference between the final sample (median = 37) and the original sample (median = 23; Z = 17.658, p < 0.001) in months post-primary cancer treatment. This variable was accounted for in all subsequent analyses.
Measures
Factors related to work outcomes
Specific survey items were extracted, and a mean score was created for each of the following variables: comorbidity, lifestyle health, social well-being, cognitive problems, distress, fatigue, cancer worry, worry about family’s cancer risk, physical function, cognitive function, social function, workplace support, and workplace problems. The final model to be tested included the following constructs: health and well-being (comorbidity, lifestyle health, and social well-being), symptom burden (cognitive problems, distress, fatigue, cancer worry, and worry about family’s cancer risk), functional limitations (physical, cognitive, and social function), workplace support, and workplace problems. When possible, a minimum of three survey items were used to constitute a measure. Confirmatory factor analysis was used to verify construct validity [15]. Items were retained if confirmatory factor analysis indicated that the items reliably formed the underlying construct. The original as well as final survey items used in the analysis appear in Appendix 1.
Specific work outcomes
This study examined two dichotomous work outcomes: (1) Work ability: Participants identified whether they were unable to work full time, unable to work the same as before cancer, or unable to work at all; and (2) Work sustainability: Participants identified whether they had ever lost and/or left a job because of cancer. Participants who endorsed any of the three work-ability items were considered to have limited work ability. These items are analogous to but distinct from traditional measures of work ability, which asked respondents to compare their current work ability to the best work ability in their lifetime and assess degree of impairment because of disease and work ability in relation to job demands [16]. Two separate models (work ability and work sustainability) were tested using structural equation modeling (SEM) in MPlus Version 7.11 [17].
Results
Demographics and cancer characteristics
The average age of the sample was 49 years. The majority of participants were Caucasian (90.7 %), women (61.6 %), married or in a domestic partnership (72.1 %), received a bachelor’s degree or higher (56.4 %), and were currently employed full (59.3 %) or part-time (41.7 %). The demographic characteristics of the sample are presented in Table 1. The current sample was younger than the US population of cancer survivors, whose median age is between 60 and 69 years [1]. The most common cancer types were breast (24.5 %), followed by testicular (8.8 %), colorectal (7.3 %), prostate (6.7 %), Hodgkin lymphoma (5.8 %), and non-Hodgkin lymphoma (5.8 %). The representation of different cancer sites was comparable to the national population of cancer survivors [1]. Average time since completion of treatment was 3 years. In this sample, 15.8 % of respondents reported a second cancer or recurrence.
Constructs in the final model
Confirmatory factor analysis using SEM measurement models was first conducted to empirically determine the items to indicate each construct. The measurement model for each construct demonstrated acceptable fit indices for social well-being, cognitive problems, fatigue, distress, cancer worries, worry about family’s cancer risk (CFI > 0.9, TLI > 0.9, RMSEA < 0.8) [18], and did not require revision. Results of the SEM measurement models for each of the constructs (i.e., social well-being, lifestyle health, cognitive problems, fatigue, distress, cancer worries, worry about family’s cancer risk, work support, and work problems) are indicated in Table 2.
A covariance matrix of all factors (health and well-being, symptoms, function, work support, and work problems) included in the final SEM analyses was generated to determine each factor’s association with work ability and work sustainability; the matrix is displayed in Table 3. Table 3 indicates a positive association between symptoms and function and among work problems, health and well-being, symptoms, and function. An inverse relationship between work problems and work support was also observed. The final models, illustrated in Figs. 1 and 2, include the constructs with robust construct validity.

Factors related to work sustainability. Note: CFI = 0.96; TLI = 0.95; RMSEA = 0.027. ***p < 0.001
Factors related to work ability and work sustainability
When work ability was the outcome (see Fig. 1), the model obtained an overall good fit (CFI = 0.961, TLI = 0.952, RMSEA = 0.027). This model indicated that only functional limitations and workplace problems were directly and significantly related to work ability.
For the outcome of work sustainability (having lost or left a job because of cancer), the model (see Fig. 2) obtained an overall good fit (CFI = 0.961, TLI = 0.952, RMSEA = 0.027). For this model, all constructs were specified as predictors of work sustainability. The final results indicated that only the construct workplace problems were significantly related to work sustainability.
Discussion
Each construct in the cancer survivor and work model that was tested was related to work ability and work sustainability. However, when all constructs were considered using an overall model, only functional limitations and workplace problems (including poor treatment, discrimination, being passed over for promotion, and not receiving accommodations) remained significant and directly related to work ability. When all constructs were entered into the SEM with work sustainability as the outcome, only negative work environment (workplace problems) was significantly and directly related to work sustainability.
Prior research has indicated that flexibility in the workplace is an important characteristic of successful work outcomes among employees with chronic medical illnesses [19–21]. A recent prospective study of 290 cancer survivors of four different cancer types found that greater sense of control over work among breast cancer survivors (HR, 1.2; 95 % CI, 1.09–1.37) and greater work flexibility among urological cancer survivors (HR, 1.70; 95 % CI, 1.07–2.7) predicted earlier return to work [22]. Qualitative studies of those working with chronic illnesses also report that flexibility in quantity of work hours [23], control over workday pacing, adjustment of physical demands, and reduction in work-related travel requirements [24] facilitate return to work and work sustainability. A systematic review further highlights the relationship among cancer survivors’ experiences of employer accommodation and flexible employment arrangements and employment status [25]. Qualitative [23, 24, 26–28] and quantitative studies [8, 29–32] have also reported evidence for the positive role of social support in the workplace as it relates to various work outcomes.
However, in the present study, workplace support and positive workplace accommodations were not independently related to either work outcome. Rather, workplace problems, including reports of discrimination, poor treatment, being passed over, and an unwillingness to make accommodations, were significantly related to both perceived work ability and work sustainability. Poor workplace support has also been associated with lower work ability in cancer survivors [33].
The finding that functional impairment is a stronger predictor of work ability than health and well-being or symptoms highlights the importance of assessing employed cancer survivors’ functional abilities in relation to work demands. Such assessment may identify whether there is an opportunity to improve observed functional limitations, which may increase the likelihood that a cancer survivor can meet certain demands of the job. This differs from exclusively considering symptoms and health problems when attempting to improve work outcomes. Recent research on the association between physical training and return to work in cancer survivors with different cancer types (breast, ovarian, Hodgkin’s and non-Hodgkin’s lymphoma, and colon) and treatment histories provides additional support for targeting physical function [34]. Once at work, physical training was effective in resuming pre-diagnosis levels of hours worked. The current findings emphasize the need to address both function (physical, cognitive, and interpersonal) and workplace problems to reduce friction in the workplace. The willingness on the part of the employer to provide realistic accommodations that both the employer and employee can agree upon may reduce the friction between cancer survivor and employer.
The data used for this investigation were collected for a very different reason (survey of many aspects of cancer survivorship) than that reported in this paper [13]. The development of constructs using existing items from the LiveStrong Survey is not as preferable as using reliable and valid measures that are available in the scientific literature. It is possible that the use of well-established measures may have led to different results. However, the current findings are consistent with research in the occupational health and disability literature. In addition, given the method of data collection, we were unable to independently confirm specific diagnoses, disease severity, and treatment regimen and therefore cannot definitively conclude that these factors are not also related to the work outcomes of interest, only that self-report of these variables were not related to these work outcomes at 3 years posttreatment.
In addition, the survey items related to workplace problems and support asked participants to “check all [workplace problems] that apply” rather than marking “yes” or “no” for each of the eight items. Therefore, while unlikely, it is possible that participants who experienced certain negative work outcomes (such as losing job because of cancer) did not check all items related to type of workplace problem and were misclassified as not having the problem.
As with many past studies in the area of cancer survivorship, the sample was primarily Caucasian with relatively high income and education, limiting the generalizability of the findings to other groups [10, 35, 36]. In addition, job type was not available as it was not collected in the survey. Education level of the sample suggests that it likely represents white-collar knowledge workers more than manual laborers. However, this limitation must be considered in light of a recent population-based study indicating that cancer survivors are more likely at this point in time to be white-collar workers than noncancer survivors in the USA [37].
Almost the entire sample (96.9 %) reported having health insurance. Although this rate is exceptionally high, it is consistent with a population-based survey that found that cancer survivors had a higher rate of health insurance than those without a history of cancer (93.2 vs. 84.8 %) [38]. Notably, three quarters of participants in this sample reported obtaining insurance from their employers, demonstrating the well-known entanglement of employment with health insurance in the USA, which is an important quality-of-life concern for cancer survivors [39].
This study analyzed cross-sectional data. Although the path analysis can illustrate the direct links of independent variables and work outcomes, it can only indicate associations between variables rather than determining the direction of the causal pathway of these variables. Furthermore, certain baseline characteristics are unknown, such as employer factors (e.g., size, industry, and availability of benefits), the quality of the work environment prior to diagnosis, the employee’s baseline work characteristics (e.g., job type, skill level, and productivity), or the presence of specific work problems before cancer diagnosis. Therefore several alternative explanations of the findings are plausible. For example, we suggest that lack of accommodations may lead workers to leave their jobs after cancer diagnosis. However, it is possible that “better” workers are more likely to work for “better” employers, such as large companies that provide more generous benefits, quality work climate, and accommodations. It is also possible that employers are more willing to develop accommodations for better workers. In fact, it is likely that feedback loops among these relationships exist; however, the present study cannot confirm this.
Despite these limitations, the results indicate that functional status in physical, cognitive, and social areas, and workplace problems (being treated poorly, discrimination, being passed over, and lack of accommodations) are associated with perceived work ability, and workplace problems are associated with work sustainability. The potential clinical implications of these findings are clear. When the goals are to return to or to successfully remain in the workplace, there is a need to query the cancer survivor regarding specific aspects of work. The systematic evaluation of function (physical, cognitive, emotional, and interpersonal) in relation to the actual demands at work and perceived ability to meet work demands can be instrumental in facilitating the survivor’s sense of ability to work. However, it is also critical that clinicians consider the survivor’s work environment. The cancer survivor’s view of the workplace including the need for realistic accommodations is also related to the likelihood of remaining at work.
Many cancer patients are remaining at work during treatment or returning to work soon afterward. Attention to functional limitations relative to work demands and negative features of the work environment, particularly in those who desire or need to work, is warranted. Simple communication strategies may be all that are needed [40, 41]. However, there are also several approaches to improve the functional outcomes of employees with a range of health problems [42], as well as the selection and implementation of work accommodation [43] found in the area of work disability prevention. A recent cancer survivorship and work model [44], which synthesizes two previous models [12, 25], also advocates for the development of interventions to educate cancer survivors’ employers. The current findings support the development of such approaches in cancer survivors and their workplaces.
References
Howlader N, Noone A, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2010. Bethesda: National Cancer Institute; 2013.
Wells M, Williams B, Firnigl D, et al. Supporting ‘work-related goals’ rather than ‘return to work’ after cancer? A systematic review and meta-synthesis of 25 qualitative studies. Psycho-Oncol. 2013;22(6):1208–19. doi:10.1002/pon.3148.
Calvio L, Peugeot M, Bruns GL, et al. Measures of cognitive function and work in occupationally active breast cancer survivors. J Occup Environ Med/Am Coll Occup Environ Med. 2010;52(2):219–27. doi:10.1097/JOM.0b013e3181d0bef7.
Hansen JA, Feuerstein M, Calvio LC, et al. Breast cancer survivors at work. J Occup Environ Med/Am Coll Occup Environ Med. 2008;50(7):777–84. doi:10.1097/JOM.0b013e318165159e.
de Boer AG, Taskila T, Ojajarvi A, et al. Cancer survivors and unemployment: a meta-analysis and meta-regression. JAMA J Am Med Assoc. 2009;301(7):753–62. doi:10.1001/jama.2009.187.
Feuerstein M, Luff GM, Harrington CB, et al. Pattern of workplace disputes in cancer survivors: a population study of ADA claims. J Cancer Surviv Res Pract. 2007;1(3):185–92. doi:10.1007/s11764-007-0027-9.
Steiner JF, Cavender TA, Nowels CT, et al. The impact of physical and psychosocial factors on work characteristics after cancer. Psycho-Oncol. 2008;17(2):138–47. doi:10.1002/pon.1204.
Fantoni SQ, Peugniez C, Duhamel A, et al. Factors related to return to work by women with breast cancer in northern France. J Occup Rehabil. 2010;20(1):49–58. doi:10.1007/s10926-009-9215-y.
Munir F, Yarker J, McDermott H. Employment and the common cancers: correlates of work ability during or following cancer treatment. Occup Med. 2009;59(6):381–9. doi:10.1093/occmed/kqp088.
Bouknight RR, Bradley CJ, Luo Z. Correlates of return to work for breast cancer survivors. J Clin Oncol Off J Am Soc Clin Oncol. 2006;24(3):345–53. doi:10.1200/JCO.2004.00.4929.
Taskila T, de Boer AG, van Dijk FJ, et al. Fatigue and its correlates in cancer patients who had returned to work—a cohort study. Psycho-Oncol. 2011;20(11):1236–41. doi:10.1002/pon.1843.
Feuerstein M, Todd BL, Moskowitz MC, et al. Work in cancer survivors: a model for practice and research. J Cancer Surviv Res Pract. 2010;4(4):415–37. doi:10.1007/s11764-010-0154-6.
Rechis R, Reynolds K, Beckjord E, et al. “I learned to live with it” is not good enough: challenges reported by post-treatment cancer survivors in the LiveStrong surveys. Austin: LiveStrong, 2011.
Division of Labor Force Statistics. Labor force statistics from the current population survey. Washington, DC: U.S. Bureau of Labor Statistics, 2013.
Kline RB. Principles and practice of structural equation modeling. 3rd ed. New York: The Guilford Press; 2011.
de Zwart BC, Frings-Dresen MH, van Duivenbooden JC. Test-retest reliability of the Work Ability Index questionnaire. Occup Med. 2002;52(4):177–81.
Muthen LK, Muthen BO. Mplus user’s guide. Los Angeles: Muthen & Muthen; 2010.
McDonald RP, Ho M. Principles and practice in reporting structural equation analysis. Psychol Methods. 2002;7:64–82.
Byrne ZS, Hochwarter WA. I get by with a little help from my friends: the interaction of chronic pain and organizational support on performance. J Occup Health Psychol. 2006;11(3):215–27. doi:10.1037/1076-8998.11.3.215. [published Online First: Epub Date]|.
Koolhaas W, van der Klink JJ, Vervoort JP, et al. In-depth study of the workers’ perspectives to enhance sustainable working life: comparison between workers with and without a chronic health condition. J Occup Rehabil. 2013;23(2):170–9. doi:10.1007/s10926-013-9449-6.
Varekamp I, van Dijk FJ. Workplace problems and solutions for employees with chronic diseases. Occup Med. 2010;60(4):287–93. doi:10.1093/occmed/kqq078.
Cooper AF, Hankins M, Rixon L, et al. Distinct work-related, clinical and psychological factors predict return to work following treatment in four different cancer types. Psycho-Oncol. 2013;22(3):659–67. doi:10.1002/pon.3049.
Kennedy F, Haslam C, Munir F, et al. Returning to work following cancer: a qualitative exploratory study into the experience of returning to work following cancer. Eur J Cancer Care. 2007;16(1):17–25. doi:10.1111/j.1365-2354.2007.00729.x.
Main DS, Nowels CT, Cavender TA, et al. A qualitative study of work and work return in cancer survivors. Psycho-Oncol. 2005;14(11):992–1004. doi:10.1002/pon.913.
Mehnert A. Employment and work-related issues in cancer survivors. Crit Rev Oncol Hematol. 2011;77(2):109–30. doi:10.1016/j.critrevonc.2010.01.004.
Yarker J, Munir F, Bains M, et al. The role of communication and support in return to work following cancer-related absence. Psycho-Oncol. 2010;19(10):1078–85. doi:10.1002/pon.1662.
Amir Z, Neary D, Luker K. Cancer survivors’ views of work 3 years post diagnosis: a UK perspective. Eur J Oncol Nurs Off J Eur Oncol Nurs Soc. 2008;12(3):190–7. doi:10.1016/j.ejon.2008.01.006.
Johnsson A, Fornander T, Rutqvist LE, et al. Factors influencing return to work: a narrative study of women treated for breast cancer. Eur J Cancer Care. 2010;19(3):317–23. doi:10.1111/j.1365-2354.2008.01043.x.
Spelten ER, Sprangers MA, Verbeek JH. Factors reported to influence the return to work of cancer survivors: a literature review. Psycho-Oncol. 2002;11(2):124–31.
Taskila T, Lindbohm ML. Factors affecting cancer survivors’ employment and work ability. Acta Oncol. 2007;46(4):446–51. doi:10.1080/02841860701355048.
Taskila T, Lindbohm ML, Martikainen R, et al. Cancer survivors’ received and needed social support from their work place and the occupational health services. Support Care Cancer Off J Multinatl Assoc Support Care Cancer. 2006;14(5):427–35. doi:10.1007/s00520-005-0005-6.
Torp S, Nielsen RA, Gudbergsson SB, et al. Worksite adjustments and work ability among employed cancer survivors. Support Care Cancer Off J Multinatl Assoc Support Care Cancer. 2012;20(9):2149–56. doi:10.1007/s00520-011-1325-3.
Lindbohm ML, Taskila T, Kuosma E, et al. Work ability of survivors of breast, prostate, and testicular cancer in Nordic countries: a NOCWO study. J Cancer Surviv Res Pract. 2012;6(1):72–81. doi:10.1007/s11764-011-0200-z.
Thijs KM, de Boer AG, Vreugdenhil G, et al. Rehabilitation using high-intensity physical training and long-term return-to-work in cancer survivors. J Occup Rehabil. 2012;22(2):220–9. doi:10.1007/s10926-011-9341-1.
Taskila T, Martikainen R, Hietanen P, et al. Comparative study of work ability between cancer survivors and their referents. Eur J Cancer. 2007;43(5):914–20. doi:10.1016/j.ejca.2007.01.012.
Drolet M, Maunsell E, Mondor M, et al. Work absence after breast cancer diagnosis: a population-based study. CMAJ Can Med Assoc J Journal de l’Association Medicale Canadienne. 2005;173(7):765–71. doi:10.1503/cmaj.050178.
Clarke TC, Soler-Vila H, Lee DJ, et al. Working with cancer: health and disability disparities among employed cancer survivors in the U.S. Prev Med. 2011;53(4–5):331–4. doi:10.1016/j.ypmed.2011.07.022.
Hewitt M, Rowland JH, Yancik R. Cancer survivors in the United States: age, health, and disability. J Gerontol A Biol Sci Med Sci. 2003;58(1):82–91.
Bradley CJ, Bednarek HL. Employment patterns of long-term cancer survivors. Psycho-Oncol. 2002;11(3):188–98. doi:10.1002/pon.544.
Nieuwenhuijsen K, Verbeek JH, de Boer AG, et al. Supervisory behaviour as a predictor of return to work in employees absent from work due to mental health problems. Occup Environ Med. 2004;61(10):817–23. doi:10.1136/oem.2003.009688.
Brown RF, Owens M, Bradley C. Employee to employer communication skills: balancing cancer treatment and employment. Psycho-Oncol. 2013;22(2):426–33. doi:10.1002/pon.2107.
Loisel P, Anema JR. Handbook of work disability. New York: Springer; 2013.
Chan F, da Silva CE, Copeland J, et al. Workplace accommodations. In: Feuerstein M, editor. Work and cancer survivors. New York: Springer; 2011. p. 233–54.
Mehnert A, de Boer A, Feuerstein M. Employment challenges for cancer survivors. Cancer. 2013;119 Suppl 11:2151–9. doi:10.1002/cncr.28067.
Acknowledgments
The authors wish to acknowledge Ruth Rechis, PhD, Stephanie Nutt, MA, MPA, and the LiveStrong Foundation for providing access to the data used in this study.
Conflict of interest
The authors have no conflicts of interest to disclose.
Source of funding
The original survey was conducted and funded by the LiveStrong Foundation.
Author information
Authors and Affiliations
Corresponding author
Additional information
The opinions and assertions contained herein are the private views of the authors and are not to be construed as being official or as reflecting the views of the Uniformed Services University of the Health Sciences or the Department of Defense.
Appendix
Appendix
Rights and permissions
About this article
Cite this article
Moskowitz, M.C., Todd, B.L., Chen, R. et al. Function and friction at work: a multidimensional analysis of work outcomes in cancer survivors. J Cancer Surviv 8, 173–182 (2014). https://doi.org/10.1007/s11764-013-0340-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11764-013-0340-4