
Abstract
Purpose
We have a limited understanding of the objectively determined physical activity levels of cancer survivors at the population level. Further, we have even less of an understanding of this behavior by weight status (i.e., normal weight, overweight, and obese). Therefore, the purpose of this study was to describe accelerometer-assessed physical activity levels among US cancer survivors and to do so across weight status.
Methods
Data from the 2003–2006 NHANES was used. One hundred twenty-six adult cancer survivors wore an accelerometer for ≥4 days, with weight status determined from measured body mass index.
Results
Approximately 13 % of cancer survivors were sufficiently active (i.e., met current physical activity guidelines). Results were not significant for light-intensity physical activity; however, results showed that obese cancer survivors engaged in 47 % less MVPA than normal weight cancer survivors (rate ratio = 0.53; 95 % CI, 0.29–0.93).
Conclusion
Most adult cancer survivors are insufficiently active and obese cancer survivors engage in less MVPA than their counterparts.
Implications for Cancer Survivors
Health care professionals are encouraged to increase cancer survivors’ awareness of the minimum levels of MVPA needed for optimal health, particularly among obese cancer survivors. Additionally, cancer survivors should also be informed of the positive health outcomes associated with light-intensity physical activity.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Regular physical activity participation may help to reduce the risk of cancer, particularly breast, prostate, colon, rectal, lung, endometrium/uterus, ovarian, and pancreatic cancer [1]. Currently, there are more than 11 million US cancer survivors and 5-year survival rates continue to improve [2]. Regular participation among cancer survivors is especially important as they may have increased risk of late medical effects from their cancer and regular engagement in physical activity may help to reduce cancer recurrence and cancer-related mortality [3, 4]. An important first step in the development, implementation, and evaluation of effective physical activity interventions for cancer survivors is to understand their physical activity patterns. Although studies have described physical activity patterns among cancer survivors, the studies have primarily been small in scale (e.g., nonrepresentative samples) and/or used nonobjective measures of physical activity [5–14]. Subjective measures of physical activity are prone to considerable measurement error [15]. As a result, we have a limited understanding of the activity patterns of cancer survivors at the population level. Therefore, the first objective of this study was to describe the objectively determined physical activity patterns of US adult cancer survivors.
In addition to promoting physical activity among cancer survivors, preventing excessive weight gain among cancer survivors is particularly important as excessive weight gain has been shown to increase the recurrence of cancer [3]. To help prevent such weight gain after cancer diagnosis and treatment, patients are encouraged to engage in physical activity, which has been shown to reduce adiposity [16]. For oncologists and other health care professionals to effectively promote physical activity among cancer patients and cancer survivors, it is important to understand the physical activity patterns of cancer survivors across weight status (i.e., normal weight, overweight, and obese). This information can help health care professionals develop targeted and effective strategies to increase the physical activity levels of cancer survivors, which is particularly important as there are a limited number of studies reporting lifestyle advice for cancer survivors. At this point, there is little population data that describes the activity patterns of cancer survivors across weight status. As a result, the second objective of this study was to describe objectively measured physical activity levels by weight status (normal weight, overweight, and obese) among US cancer survivors.
Methods
Design and participants
Data from the present study were obtained from the 2003–2006 National Health and Nutrition Examination Survey (NHANES). NHANES is an ongoing survey conducted by the Centers for Disease Control and Prevention that uses a representative sample of non-institutionalized US civilians, selected by a complex, multistage probability design. The multistage design consists of four stages, including the identification of counties, segments (city blocks), random selection of households within the segments, and lastly, random selection of individuals within the households. The survey examines a nationally representative sample of approximately 5,000 individuals each year, with data collected in 15 counties across the country each year. Briefly, participants were interviewed in their homes and then subsequently examined in mobile examination centers by NHANES personnel. Further details about NHANES can be found elsewhere [17]. NHANES study procedures were approved by the National Center for Health Statistics ethics review board, with informed consent obtained from all participants prior to data collection.
Twenty thousand four hundred seventy (20,470) participants provided data in the 2003–2006 cycles. Participants were asked if they had ever been told by a doctor or health care professional that they had cancer or malignancy of any kind. Only participants with certain types of cancer were included in the analyses, specifically cancer sites that are associated with physical activity. Based on the Physical Activity Guideline Advisory Committee Report [1], physical activity has been shown to be associated with the following cancer sites: breast, prostate, colon, rectal, lung, endometrium/uterus, ovarian, and pancreatic. However, in the present study, few participants had pancreatic, rectal, ovarian, or lung cancer; therefore, only participants known to have been diagnosed with breast, colon, prostate, and endometrium cancer were included. Of the 2003–2006 NHANES participants, 9,752 had sufficient accelerometry data. Among these, 239 were diagnosed with breast, colon, prostate, or uterine cancer. Participants who had been diagnosed with cancer within 5 years were excluded from analyses of the present study as it is possible that they were still receiving treatment for their cancer, which ultimately may influence their activity patterns. After excluding those with a diagnosis of cancer within 5 years (or if it was not possible to determine time since diagnosis due to missing data), 132 remained. Lastly, after excluding those with missing data on the weight status variable or the covariates, 126 remained, which comprised the analytic sample ranging in age between 34 and 84 years.
Based on the study design and use of sample weights, these cancer survivors represent a population-weighted sample of 2,295,003 adult cancer survivors. Information on the use of sample weights to generate population weighted estimates is available elsewhere [18]. Briefly, each person in the NHANES dataset is assigned a sample weight. This sample weight is created using three steps [19]: first, the base weight is calculated for each person which takes into consideration the participant’s probability that their county, city block, household, and then her/himself is selected; second, the sample weight is adjusted for non-response (i.e., whether they were a non-respondent to either the interview portion and/or the exam portion); and third, post-stratification adjustment is made to the sample weights to match the 2000 US Census population.
Measurement of physical activity
Participants who were not prevented by impairments of walking or wearing an accelerometer were issued an ActiGraph 7164 accelerometer. Participants were asked to wear the accelerometer during waking hours (and while not in water [e.g., shower and swimming]) on the right hip for 7 days following their examination. The accelerometer was affixed to an elastic belt worn around the waist. The output of an accelerometer is activity counts, which are proportional to an individual’s acceleration. The accelerometer output is digitized using an analog-to-digital converter, and once digitized, the signal passes through a digital filter that detects accelerations ranging from 0.05 to 2.00 g in magnitude with frequency responses ranging from 0.25 to 2.5 Hz to filter motion outside normal human movement. The filtered signal is then rectified and summed over a pre-determined epoch period. After the activity count is sorted into an epoch, it is stored in the internal memory and then the integrator is reset to zero. Detailed information on the ActiGraph accelerometer can be found elsewhere [20]. For the present study, accelerometry data was collected in 1-min epoch intervals, with data presented as 1-min bouts. Time spent at different physical activity intensities was assessed, including light, moderate, and vigorous physical activity intensity. Activity counts between 100 and 2,019 counts per minute were used to classify time spent in light-intensity physical activity; activity counts ≥2,020 but <5,999 were considered moderate intensity; and activity counts ≥5,999 were considered vigorous-intensity activity [21]. Participants were classified as meeting physical activity guidelines if they engaged in 150-min of moderate intensity or 75-min of vigorous-intensity physical activity per week or some combination of the two [22].
To account for a combination of moderate and vigorous-intensity physical activity, minutes of vigorous intensity per week were multiplied by 2 before being added to time spent at moderate intensity per week [23], as vigorous-intensity physical activity (6 + metabolic equivalents) is two times the energy cost than moderate-intensity physical activity (3–5.9 metabolic equivalents). For the analyses described here, and to represent habitual physical activity patterns, only those participants with at least 4 days with 10 or more hours per day of monitoring data were included in the analyses [21]. Non-wear was defined by a period of a minimum of 60 consecutive minutes of zero activity counts, with the allowance of 1–2 min of activity counts between 0 and 100 [21].
Weight status
The first objective of the study was to describe activity patterns among adult cancer survivors. The second objective was to describe activity patterns across weight status. Body mass index (BMI) was calculated from measured weight and height (weight in kilograms divided by the square of height in meters). Participants were considered to have normal weight if there BMI was <25 kg/m2; overweight was defined as a BMI ≥ 25 and <30 kg/m2; and obese was defined as a BMI ≥ 30 kg/m2 [24].
Other measurements
For the second objective examining activity patterns across weight status, various covariates were included in the analytic model based on previous research showing these variables to associate with physical activity and/or weight status [21, 25–28]. A questionnaire administered in the home was used to obtain information on age, gender, race–ethnicity, poverty-to-income ratio (PIR), and whether they had been told by a health care professional that they had coronary heart disease, stroke, or arthritis. As a measure of socioeconomic status, a PIR value below 1 is considered below the poverty threshold. The PIR is calculated by dividing the family income by the poverty guidelines, which is specific to the family size, year assessed, and state of residence. Lastly, accelerometer wear time was included as a covariate as it can influence activity estimates.
Data analysis
Statistical analyses were performed using Stata (version 12.0, College Station, TX). Where appropriate (i.e., when the cell size was large enough [e.g., >100]), procedures from sample survey data (e.g., using sample weights) were used to account for the complex survey design used in NHANES; these analyses were computed using Stata’s survey commands (e.g., “svy:”), with unweighted estimates generated from analyses by not using “svy” commands. New sample weights were created for the combined NHANES cycles following analytical guidelines for the continuous NHANES [29]. Specifically, the 4-year MEC sample weights (i.e., 2003–2006) were created by dividing the 2-year MEC sample weights by 2. In the situation where an analysis resulted in a stratum with a single cluster, the variance contribution from a stratum with a single cluster was centered at the overall cluster mean.
Means and standard errors were calculated for continuous variables and proportions were calculated for categorical variables. Multivariate assessment of the association between MVPA and weight status was examined using a negative bionomial regression as MVPA (outcome variable expressed in integral minutes) failed tests of normality. Rate ratios from the negative binomial model represent the rate of events for each variable in the model while holding the other variables in the model constant. One model was computed, with the weight status variable, along with the covariates, entered into the model. For the weight status variable, normal weight served as the referent group.
To examine the association between light-intensity physical activity (outcome variable) and weight status, a multivariate linear regression was employed. Covariates in the linear regression and negative bionomial models included age, gender, race–ethnicity, PIR, coronary heart disease, stroke, arthritis, and accelerometer wear time. Statistical significance was established at the p < 0.05 level.
Results
Among the analyzed sample (n = 126), the mean (SE) age was 68.3 years (1.1); 76.8 % (2.9) were female; 84.8 % (2.8) were non-Hispanic white; mean PIR was 2.8 (0.1); mean BMI was 28.9 kg/m2 (0.7); 7.1 % (2.6) had coronary heart disease; 5.6 % (2.5) previously had a stroke; 58.0 % (4.9) had arthritis; and 26.2, 38.4, and 35.2 %, respectively, were normal weight, overweight, and obese.
With regard to the first objective, accelerometer-determined physical activity levels across cancer sites are shown in Table 1. Given the relatively small sample for each cancer site, unweighted estimates are provided for each separate cancer site. However, a weighted estimate is provided for all cancers combined. The findings showed that these cancer survivors (n = 126), representing a population weighted sample of 2,295,003, engaged in 295, 10, and 0.4 min/day, respectively, of light, moderate, and vigorous-intensity physical activity. Additionally, 12.6 % of cancer survivors were sufficiently active (i.e., met current physical activity guidelines).
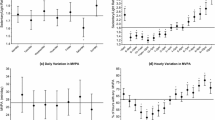
The second objective of the present study was to examine the association between physical activity and weight status. After controlling for age, gender, race–ethnicity, PIR, coronary heart disease, stroke, arthritis, and accelerometer wear time, the negative binomial regression results showed that obese cancer survivors engaged in 47 % less MVPA than normal weight cancer survivors (rate ratio = 0.53; 95 % CI, 0.29–0.93) (Table 2). Significant covariates included age, gender, coronary heart disease, and stroke, suggesting that those who were older, female, and had a history of coronary heart disease or stroke engaged in less physical activity than their counterparts. Notably, there was no association between light-intensity physical activity and weight status.
Discussion
The aim of this study was to describe the activity pattern of cancer survivors and describe these patterns across weight status and weight control practices. Major findings of this study are threefold: (1) cancer survivors are insufficiently active, with 87 % of cancer survivors not engaging in the recommended levels of physical activity; (2) obese cancer survivors engaged in less MVPA than their counterparts; and (3) there was no association between light-intensity physical activity and weight status.
With regard to our first objective, most cancer survivors are insufficiently active and may be at risk for the negative health outcomes associated with physical inactivity. These findings are similar to those by Smith et al. [30] who showed that 95 % of cancer survivors did not meet objectively determined physical activity guidelines. However, these authors used the 1996 physical activity recommendation of the Surgeon General who indicated that individuals were sufficiently active if they engaged in at least 30-min of moderate-intensity physical activity on most and preferably all days of the week or at least 20-min of vigorous-intensity physical activity on at least 3 days a week [31]. Our findings are likely slightly different because we used the updated 2008 government guidelines [22], which state that individuals can meet guidelines if their total summed physical activity over a week period is at least 150 min of moderate intensity or 75 min of vigorous-intensity physical activity, or some combination of the two. Extending the work of Smith et al. [30], the present study also reports objectively measured light-intensity physical activity levels among cancer survivors which, to our knowledge, have not been previously reported in the literature. Although there is considerable evidence showing the benefits of moderate-to-vigorous-intensity physical activity, at this point, we have a limited understanding of the potential health benefits associated with light-intensity physical activity. However, emerging evidence suggest that light-intensity physical activity may be associated with favorable health outcomes. For example, Loprinzi and colleagues [32] showed that light-intensity physical activity was associated with various cardiovascular disease risk factors, along with the metabolic syndrome, in a dose–response manner. These findings showed that in the general population, individuals engaging in over 450-min/day of light-intensity physical activity were 45 % less likely to have metabolic syndrome.
At this point, it is unclear what dose of physical activity is associated with favorable health outcomes among cancer survivors. However, based on the results of Loprinzi and colleagues [32] in the general population, it is likely that cancer survivors are not engaging in sufficient levels of light-intensity physical activity to obtain meaningful health benefits as the average minutes per day of light-intensity physical activity observed in the present study was only 295. Given that light-intensity physical activity levels were not different across weight status underscores the importance of promoting this intensity level among cancer survivors, which, compared to higher intensity levels, may be a more palatable intensity level given the potential medical side effects associated with cancer, age-related declines in physical activity, and other comorbidities and/or secondary conditions that some cancer patients may have. It is not surprising that light-intensity levels were not different across weight status, as current government guidelines do not include light-intensity level physical activity recommendations.
Based on the present findings, cancer survivors who are not trying to lose or maintain their weight, in particular, may be in need of counseling to promote physical activity. Clinicians are well suited to promote physical activity among cancer survivors and are encouraged to do so using evidenced-based counseling strategies [33], such as motivational interviewing, which have been shown to be effective among cancer survivors [34]. Rather than providing traditional advice to be active or simply telling the patient to be active, motivational interviewing involves a patient-centered approach that explores the individual’s perspective and potential ambivalence to changing their behavior. In motivational interviewing, the counselor, for example, uses open-ended questions, reflective listening, affirmation, provision of summary statements, and eliciting change talk. For detailed information on delivering motivational interviewing, the reader is referred to the work of Resnicow [35–37] and the text by Miller and Rollnick [38].
Limitations to the present study include the cross-sectional study design, which does not allow for changes in physical activity to be determined over time. However, despite this limitation, major strengths of this study include employing an objective measure to determine time spent in light, moderate, and vigorous-intensity physical activity, describing activity estimates among cancer survivors, and describing these estimates across weight status in a sample of US cancer survivors.
In summary, the majority of US cancer survivors do not engage in sufficient levels of physical activity; obese cancer survivors engage in less MVPA than their counterparts; and light-intensity physical activity levels do not appear to differ across weigh status. Further efforts are needed to promote physical activity among cancer survivors, particularly among obese cancer survivors. Future investigations are also encouraged to determine the specific dose of physical activity (for both light-intensity and MVPA) needed to elicit improvements in favorable health outcomes among cancer survivors. Additionally, it would be of interest for future research to determine whether race–ethnicity, adiposity, and drug treatment, for example, moderate the association between weight status and physical activity behavior.
References
Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report, 2008. Washington, DC: U.S. Department of Health and Human Services; 2008.
Ries LAG, Melbert D, Krapcho M, Stinchcomb DG, Howlader N, Horner MJ, et al., editors. SEER Cancer Statistics Review, 1975–2005. Bethesda: National Cancer Institute; 2008.
Loprinzi PD, Cardinal BJ, Winters-Stone K, et al. Physical activity and the risk of breast cancer recurrence: a literature review. Oncol Nurs Forum. 2012;39:269–74.
Lee IM, Wolin KY, Freeman SE, et al. Physical Activity and Survival after Cancer Diagnosis in Men. J Phys Act Health. 2012
Moskowitz MC, Feuerstein M, Todd BL. Job stress and physical activity related to elevated symptom clusters in breast cancer survivors at work. J Occup Environ Med. 2013;55:93–8.
Blaney JM, Lowe-Strong A, Rankin-Watt J, et al. Cancer survivors’ exercise barriers, facilitators and preferences in the context of fatigue, quality of life and physical activity participation: a questionnaire-survey. Psychooncology. 2013;22:186–94.
Chung JY, Lee DH, Park JH, et al. Patterns of physical activity participation across the cancer trajectory in colorectal cancer survivors. Support Care Cancer. 2013;21(6):1605–12.
Zhao G, Li C, Li J, et al. Physical activity, psychological distress, and receipt of mental healthcare services among cancer survivors. J Cancer Surviv. 2012;7(1):131–9.
Charlier C, Pauwels E, Lechner L, et al. Physical activity levels and supportive care needs for physical activity among breast cancer survivors with different psychosocial profiles: a cluster-analytical approach. Eur J Cancer Care (Engl). 2012;21:790–9.
Buffart LM, Thong MS, Schep G, et al. Self-reported physical activity: its correlates and relationship with health-related quality of life in a large cohort of colorectal cancer survivors. PLoS One. 2012;7:e36164.
Hsu HT, Huang CS, Liu Y, et al. Exercise behaviors in breast cancer survivors in Taiwan. Cancer Nurs. 2012;35:E48–56.
Wrosch C, Sabiston CM. Goal adjustment, physical and sedentary activity, and well-being and health among breast cancer survivors. Psychooncology. 2013;22(3):581–9. doi:10.1002/pon.3037.
Paxton RJ, Phillips KL, Jones LA, et al. Associations among physical activity, body mass index, and health-related quality of life by race/ethnicity in a diverse sample of breast cancer survivors. Cancer. 2012;118:4024–31.
Szymlek-Gay EA, Richards R, Egan R. Physical activity among cancer survivors: a literature review. N Z Med J. 2011;124:77–89.
Shephard RJ. Limits to the measurement of habitual physical activity by questionnaires. Br J Sports Med. 2003;37:197–206. discussion 206.
Shaw K, Gennat H, O’Rourke P, et al. Exercise for overweight or obesity. Cochrane Database Syst Rev. 2006;CD003817.
Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey. http://www.cdc.gov/nchs/nhanes/about_nhanes.htm. Accessed 25 Feb 2013.
Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey, 2010. Overview of NHANES Survey Design and Weights. http://www.cdc.gov/nchs/tutorials/environmental/orientation/sample_design/. Accessed 25 Feb 2013.
National Health and Nutrition Examination Survey: Specifying Weighting Parameters. Available at: http://www.cdc.gov/nchs/tutorials/NHANES/SurveyDesign/Weighting/OverviewKey.htm#base_weight. Accessed 25 Feb 2013.
Chen KY, Bassett Jr DR. The technology of accelerometry-based activity monitors: current and future. Med Sci Sports Exerc. 2005;37:S490–500.
Troiano RP, Berrigan D, Dodd KW, et al. Physical activity in the United States measured by accelerometer. Med Sci Sports Exerc. 2008;40:181–8.
U.S. Department of Health and Human Services (2008). Physical Activity Guidelines for Americans. October 2008. http://www.health.gov/paguidelines/. Accessed 25 Feb 2013.
Tucker JM, Welk GJ, Beyler NK. Physical activity in U.S.: adults compliance with the physical activity guidelines for Americans. Am J Prev Med. 2011;40:454–61.
World Health Organization (2000). Obesity: preventing and managing the global epidemic. Report of a WHO Consultation. WHO Technical Report Series 894. Geneva: World Health Organization, 2000.
Hawkins MS, Storti KL, Richardson CR, et al. Objectively measured physical activity of USA adults by sex, age, and racial/ethnic groups: a cross-sectional study. Int J Behav Nutr Phys Act. 2009;6:31.
Herrmann SD, Barreira TV, Kang M, et al. (2013) How many hours are enough? Accelerometer wear time may provide bias in daily activity estimates. J Phys Act Health (in press).
Ball K, Salmon J, Giles-Corti B, et al. How can socio-economic differences in physical activity among women be explained? A qualitative study. Women Health. 2006;43:93–113.
Kaptein SA, Badley EM. Sex differences, age, arthritis, and chronic disease: influence on physical activity behaviors. J Phys Act Health. 2012;9:540–8.
Centers for Disease Control and Prevention. National Health and Nutrition Examination Survey. Specifying Weight Parameters. http://www.cdc.gov/nchs/tutorials/NHANES/SurveyDesign/Weighting/Task2.htm. Accessed 25 Feb 2013.
Smith WA, Nolan VG, Robison LL, et al. Physical activity among cancer survivors and those with no history of cancer—a report from the National Health and Nutrition Examination Survey 2003–2006. Am J Transl Res. 2011;3:342–50.
U.S. Department of Health and Human Services. Physical activity and health: a report of the surgeon general. Atlanta, GA: Centers for Disease Control and Prevention (CDC), National Center for Chronic Disease Prevention and Health Promotion, 1996.
Loprinzi PD, Lee H, Cardinal BJ. Dose response association between physical activity and biological, demographic, and perception of health variables. Obes Facts. 2013 (in press).
Cardinal BJ, Levy SS, John DH, et al. Counseling patients for physical activity. Am J Med Sports. 2002;4:364–71.
Bennett JA, Lyons KS, Winters-Stone K, et al. Motivational interviewing to increase physical activity in long-term cancer survivors: a randomized controlled trial. Nurs Res. 2007;56:18–27.
Resnicow K, DiIorio C, Soet JE, et al. Motivational interviewing in health promotion: it sounds like something is changing. Health Psychol. 2002;21:444–51.
Resnicow K, McMaster F, Rollnick S. Action reflections: a client-centered technique to bridge the WHY-HOW transition in motivational interviewing. Behav Cogn Psychother. 2012;40(4):474–80. doi:10.1017/S1352465812000124.
Resnicow K, McMaster F. Motivational Interviewing: moving from why to how with autonomy support. Int J Behav Nutr Phys Act. 2012;9:19.
Miller WR, Rollnick S. Motivational interviewing: Preparing people for change. 2nd ed. New York: Guilford Press; 2002.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Loprinzi, P.D., Lee, H. & Cardinal, B.J. Objectively measured physical activity among US cancer survivors: considerations by weight status. J Cancer Surviv 7, 493–499 (2013). https://doi.org/10.1007/s11764-013-0293-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11764-013-0293-7