
Abstract
Introduction
While fatigue has been associated with work limitations the combined influence of specific diagnosis and treatment exposures based on medical records on work limitations in breast cancer survivors is currently unknown. Since symptom burden and perceived health can interfere with work, the present study investigated the relationship among these variables and work outcomes.
Methods
Medical chart abstraction, demographic measures, SF 36, the Work Limitations Questionnaire (WLQ) and measures of symptom burden, including hot flushes were obtained in 83 breast cancer survivors a mean of three years post treatment. OLS and poisson regression were used to determine the relationship of these factors to work productivity and work absences.
Results
Breast cancer survivors reported a mean reduction in productivity of 3.1% below the healthy worker norm. This amounts to a loss of 2.48 hours of work over two weeks of full time employment. Stages 1 and 2 were related to work limitations. After controlling for stage, fatigue and hot flashes were each associated with work performance losses of 1.6% (p = 0.05) and 2.2% (p < 0.001), respectively. Protective factors included marriage and greater personal earned income.
Conclusions
Fatigue and hot flashes are important factors related to work productivity in breast cancer survivors even at three years post treatment.
Implications for survivors
Therapy for hot flashes should be given serious consideration in breast cancer survivors who are experiencing work limitations.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Background and significance
About 2.4 million women in the US are living with a history of breast cancer [1]. Factors associated with breast cancer treatment and survivorship have been documented in recent research [2–13].
In a study using the nationally representative Current Population Survey, Bradley and colleagues demonstrated that a diagnosis of breast cancer other than ductal carcinoma in situ (DCIS) (Stage 0) is significantly associated with not working 6 months later [4]. Patients who continued to work did so for significantly fewer hours than those not diagnosed with cancer. Drolet and colleagues found similar results for employment in survivors 3 years after diagnosis [7]. Factors that were associated with unemployment were older age, low incomes (less than $20,000 per year), union membership and any new cancer event during follow-up. In other research, advanced tumor stage, black race and low health status have been associated with lower rates of return to work [6]. Yet at least one study of return to work in cancer found that when job characteristics were controlled, race and income were no longer significant predictors of return to work [8]. Chemotherapy treatment has not been associated with return to work [6, 7].
Most survivors who leave the workforce report doing so for personal reasons, not employer discrimination or lack of accommodation [7, 14]. Among survivors who were denied pay increases or who “had trouble with their bosses,” most attributed these events to factors other than their cancer survivorship [15]. Yet perceived employer discrimination because of cancer has a negative effect on return to work within 12 months of diagnosis [7].
Among women who remain employed after diagnosis and treatment for breast cancer, higher wages and hours worked (relative to a control group) have been observed [5]. These results suggest that job characteristics, more than the specific diagnosis and treatment, are important in predicting career success after diagnoses.
Questions remain regarding work performance [16]. Many common side effects of breast cancer and its treatment are factors likely to be associated with work, including fatigue, reductions in the range of motion of the arm on the affected side, lymphodema and pain. Most recently, a cross-sectional survey study by Hansen and colleagues (2008) found that breast cancer survivors reported significantly lower work productivity than their peers who never had cancer [2]. Fatigue was the symptom complaint with the strongest association with reduced work productivity [2].
Work productivity has been studied in other chronic conditions. The validated Work Limitations Questionnaire (WLQ) [17, 18] has been used in studies of brain tumors, depression, arthritis and migraine [19–22]. For example, Feuerstein et al. (2007) found that brain tumor survivors reported more time lost from work and lower work productivity than a comparison group [19]. Differences were associated with modifiable factors [19]. Lerner, et al. (2004) documented higher rates of new unemployment, job turn-over, absenteeism and lost work productivity among employees with depression compared to rheumatoid arthritis or a control group [21].
In the case of breast cancer, understanding the relationship between survivorship and work performance is particularly important for several reasons: (1) breast cancer survivors often continue to work for many years after treatment, (2) the expected prevalence of breast carcinoma is high [1], and (3) indications for adjuvant chemotherapy have expanded as an increasing number of studies demonstrate significant, albeit small, improvements in outcomes [23–25].
This study had the following goals: (1) To measure absenteeism and productivity at work in subjects who were diagnosed with ductal carcinoma in situ or Stage I–III breast cancer and completed all treatment at least 12 months previously, (2) To compare lost work productivity among survivors to healthy worker norms, and (3) To identify factors associated with deficits in productivity while working, specifically cancer and treatment characteristics, demographics and current health problems and symptoms, including fatigue and mental health.
Methods
Overview
We conducted a medical chart review to identify all patients who were diagnosed with Stage 0 ductal carcinoma in situ (DCIS) or Stage I, II or III breast cancer between December 1996 and December 2002 and completed all therapy at least 12 months prior to recruitment at the James P. Wilmot Cancer Center in Rochester, New York. All subjects had received radiation therapy. Subjects who met inclusion criteria were screened and recruited by their oncologist at regularly scheduled follow-up appointments. Subjects who agreed to participate in the study consented to release their oncology medical records and received a survey which they returned through the mail in a pre-addressed postage-paid envelope.
Sample
Subject identification and screening
Using oncology medical records, we first identified women diagnosed with DCIS or Stage I, II, or III breast cancer between December 1996 and December 2002 who received radiation treatments (mean total dose = 6,400 Gy) and who finished all treatment at the James P. Wilmot Cancer Center in Rochester, New York at least 1 year prior to enrollment in the study in 2003–2004. These subjects were then contacted at their regular follow-up visits for screening and recruitment. Exclusion criteria were assessed at screening. Exclusion criteria included unemployment, metastatic disease, history of stem cell rescue with high dose chemotherapy and pregnancy. All study procedures were approved by the Institutional Review Board at the University of Rochester.
Recruitment and informed consent
Subjects who met screening criteria at their regularly scheduled follow-up oncology visits were recruited by their oncology health care team (physicians, nurse practitioners and nurses) during the same visit. Each enrolled subject provided written informed consent to participate at the time of enrollment. At the visit, subjects were given surveys and self-addressed, stamped envelopes and asked to complete and return the surveys within 3 days of their visit. Research staff called non-responders 1 week after their visit. If a subject could not be reminded by phone, then research staff sent a duplicate survey to that subject’s mailing address.
Participants consented to both complete the survey and permit the study personnel to extract data from their medical charts.
Data collection
Data were drawn from radiation and medical oncology records as well as patient surveys. Medical chart review provided detailed data about each subject’s diagnoses, concurrent medications, comorbidities and treatment (including chemotherapy regimen, doses, and number of cycles). Surveys provided detailed data about demographics, menopause, current health and general functioning, work outcomes, symptoms and current medication use.
Measurement of absences and productivity while working (“Lost work productivity”)
We specifically asked respondents to report only absences caused by their own health. All work outcomes were derived from the self-administered written survey. Performance while sick at work (“lost work productivity”) was evaluated using the Work Limitations Questionnaire (WLQ) [17]. The validity and reliability of the WLQ has been established (17–18). The WLQ measures specific areas of performance in separate sub-scales, including Time Management, Physical Demands, Mental-Interpersonal Demands and Output Demands. Scale scores range from 0 (limited none of the time) to 100 (limited all of the time). The reference period is the past 2 weeks. Scales are then scored using methods developed from objective production and survey data collected from more than 900 employees in earlier research. The WLQ Productivity Index Score indicates the percentage difference in output from a healthy benchmark population (18).
Self-reported absences in the previous 2 weeks have been shown to be accurate [26]. Absences may be caused by many factors of which employee health is only one. For example, women with young children are often absent from work because their children are sick.
Defining cancer therapy variables
In subjects treated with chemotherapy, we collected detailed information on chemotherapeutic agents, doses (normalized to body surface area), interval between chemotherapy courses, and number of courses of each chemotherapy regimen. Surgery type was defined as breast conserving or mastectomy. All subjects received radiation (mean total dose = 6,040, range 4,600–6,840). Adjuvant hormonal therapy (tamoxifen) and use of gabapentin (Neurontin) were determined from medical charts and confirmed by self-report at the time of enrollment.
Defining fatigue, poor mental health and overall health status
Following the methods employed by Bower, Ganz, et al. (2006) we defined fatigue as a score of greater than or equal to one standard deviation below the US age–sex norm on the SF-36 vitality scale [27]. Following the guidelines in the manuals for the SF-36, we defined poor mental health as a score of greater than or equal to one standard deviation below the US age–sex norm on the SF-36 mental health inventory [28]. Excellent overall health was defined by the global self-rated health item on the SF-36: “In general, would you say your health is excellent, very good, good, fair or poor?” Responses to this self-rated health item have been shown to be predictive of survival in cancer and other patients independent of clinical measures [29, 30]. We controlled for excellent health because the majority of our sample of employed survivors had a distribution of scores in the good to very good range. In our data, the correlation between Excellent Health and Fatigue was small (Pearson Product Moment Correlation = −0.26).
Statistical methods
T-tests were used to compare group differences for continuous outcomes while chi-square tests were employed for testing the associations of categorical variables for analyses of demographic and other related variables at baseline.
All dependent variables have reference periods of the previous 2 weeks. Poisson regression was used to estimate models of absences due to employee health.
Ordinary least squares (OLS) regression with robust standard errors was used to model lost work productivity as a percentage reduction relative to normalized age–sex scores as measured by the WLQ Index. Variables were selected a priori. Insignificant variables were removed for parsimony. Regression diagnostics were used to check assumptions, including omitted variable bias, heterosckedasticity, kurtosis and outliers. A single observation that exerted significant leverage on the overall model was excluded. Only two observations involved Stage 3 cancers and these were also dropped from the model. The Ramsey RESET test was insignificant, finding no evidence of multicollinearity. Variance inflation factors were 75–90% for all variables except the categorical Stage variables, as expected. All analyses were conducted using Stata SE Version 8.
Results
Our initial search of oncology medical records identified 140 possible candidates, of whom only 92 met the study requirements. Thirty eight were unemployed and therefore excluded. Clinical exclusion criteria included metastatic disease (n = 2), exposure to high dose chemotherapy with stem cell rescue (n = 4), multiple sclerosis (n = 1), cardiac catheterization (n = 1), and fracture (n = 1) or pregnancy (n = 1).
Of the 92 eligible subjects, 6 declined to participate and 3 never returned their surveys. Of our 83 subjects, 6 returned incomplete surveys and 1 had incomplete chemotherapy data due to having received some treatment at a different hospital. Therefore, some analyses include fewer than 83 subjects.
Characteristics of the study sample are given in Table 1. Subjects exposed to cyclophosphamide and doxorubicin (CA), a commonly used regimen, did not differ significantly from the patients who received other chemotherapy regimens. Non-participants resembled those who enrolled in terms of age (mean: 52.5), cancer treatment and time since radiation treatment completion.
Employment
Forty-three subjects (51.8%) were working part-time and 48.2% (n = 40) were working full-time. None were working more than one job. About one-third of employed survivors (n = 28 or 33.7%) reported going to work even though they “did not feel well” at some point in the past 2 weeks. Two reported feeling unwell everyday during the past 2 weeks, but most reported going to work while feeling sick on only one (n = 8) or two (n = 10) days. As a result of working while feeling unwell, 12 subjects reported that it took longer for them to get their work done than usual. They worked an average of 1.4 extra hours to complete their work (SD = 0.74) with a range of 0.5 hours to 2 hours. No one reported working extra hours to make up for a sickness absence in the previous 2 weeks.
There were no significant differences between DCIS and Stage 1–3 survivors in terms of the proportion who reported working extra hours to make up for being sick at work or the number of hours worked.
Lost work productivity: the Work Limitations Questionnaire (WLQ)
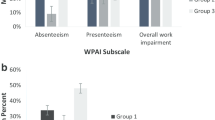
The mean WLQ Productivity Index Score indicated that productivity at work was 3.01% (SD 2.91) below the healthy worker norm. This represents a loss of 2.48 hours of work over 2 weeks of full-time employment [28]. Subscales are not benchmarked but reduced values appeared in all scales except Physical Demands.
Regression models
Lost work productivity
Higher scores on the WLQ Productivity Index Score indicate worse productivity, or greater work limitation. Compared to Stage 0 (DCIS) cancer survivorship, Stage 1 and 2 cancers were associated with reductions in performance while working of 1.63% (p = 0.10) and 3.05% (p < 0.001), respectively (Table 2). Insignificant were type of surgery, time since completing radiation therapy, type and number of cycles of chemotherapy, and current use of tamoxifen. These were dropped from our model. Fatigue and hot flashes were independently associated with work performance losses of 1.55% (p = 0.05) and 2.18% (p < 0.001), respectively. Protective factors included a score of ‘excellent overall health on the SF-36 general health status item (a reduction in loss of 1.38%, p < 0.10), being married (a reduction in loss of 1.84%, p < 0.001) and each additional $1,000 in current personal earned income (a reduction of 0.03%, p < 0.05, for every $1,000 of earned income). The correlation between “Excellent health status” and fatigue was small (Pearson Product Moment correlation = −0.26). Age was not statistically significant nor were the number of hours worked. The overall model explained 47% of the variance in lost work productivity and was significant at p < 0.001 (Table 2). Menopause, poor mental health and current tamoxifen use were insignificant after controlling for other variables and were dropped from the model.
Antidepressant use was prevalent in our sample (n = 18) (Table 1) but was not associated with lost work productivity. Only three subjects had SF-36 Mental Health Inventory scores suggestive of clinical depression and 4 more had scores suggestive of poor mental health. None of these factors was significant in our model.
Absences
Absences from work due to illness in the past 2 weeks were reported by 9 (10.8%) of subjects. Absences ranged in duration from 1–3 days. Subjects with lost work productivity had significantly more absences in 2-sided t-tests. Poisson regression (with exposure defined as the number of hours typically worked in a 2-week period) (see Table 3) revealed that after controlling for typical work hours and excluding a single outlier case due to leverage, only two variables approached statistical significance: Being married and being the primary caregiver of a child or other dependent. The incident rate ratio was 3.38 (p < 0.06, 1 tailed) for caregivers and 0.09 (p < 0.002) for married subjects.
Discussion
The survivors in our study, who had completed all treatment for ductal carcinoma in situ or Stage I–III breast cancer at least 12 months and an average of 3 years before enrollment, reported work productivity significantly below the healthy worker benchmark. The loss in productivity was important, amounting to a mean of approximately 2.4 hours per 2 weeks of work. Productivity was inversely and significantly associated with stage, fatigue and the presence of hot flashes. Protective factors included older age, being married, and higher personal earned income from employment.
This study builds on the work of Hansen, at al. (2008) and others by using medical record data in addition to survey data to study work productivity [2]. For example, we incorporated chemotherapy exposure, dosing, and timing between courses in our data collection. This study also drew on patient opinion to elicit the most important symptoms reported on a symptom battery. In doing so, we were able to identify hot flashes as a pressing problem among Stage I–III and DCIS survivors. Hot flashes are not typically assessed in symptom profiles of cancer survivors, although they may follow chemotherapy-induced menopause. Even when induced by aging, hot flashes are known to affect sleep, a factor associated with reduced productivity [2].
Consistent with Hansen et al. (2008), our results show that fatigue is a factor associated with productivity [2]. Similarly, excellent health status was a factor associated with relatively better productivity in our study, just as “healthy behaviors” were in the Hansen study. Our sample of survivors demonstrated mean group scores on the SF-36 that matched those of women of similar age who visit primary care doctors. Their rates of absence from work (<10% incidence in a 2-week period with absences averaging 1 day) were comparable to healthy worker norms. No survivors worked extra hours to compensate for reduced productivity at work.
Our finding that absences were associated with higher work productivity losses during the same time period are consistent with the findings by Brouwer et al. (2002) who found that about 25% of absent workers reported productivity losses at work preceding the absence and 20% reported reduced productivity after returning to work from a sickness absence [31].
Limitations include the combination of longitudinal clinical data and cross-sectional productivity data. The design does not allow for the determination of causality with regard to productivity. Similarly, this was not an intervention study and so did not include a control group. Rather, we provide productivity loss estimates benchmarked to healthy worker norms using the widely used Work Limitations Questionnaire. Similarly, we compare our results across Stages, including Stage 0 or ductal carcinoma in situ (DCIS). These factors combined with the relatively small sample size of 83 make these preliminary results only more robust. Finally, the results may not be generalizable to the larger US population given the demographics of the Rochester, New York area. According to the American Community Survey (2006), Monroe County, in which Rochester is located is predominantly white (79.2% cf. US 73.9%) [32].
Implications for clinical practice include the importance of inquiring about and managing hot flashes in survivors, which were associated with both significant symptom complaints and reduced productivity in our study. Breast cancer survivors may be assisted at work by better identification and treatment of hot flashes and fatigue. Gabapentin has been shown to reduce hot flashes in breast cancer patients [33], yet in January 2008 the FDA issued an alert noting an unexpected increase in suicidal ideation and behavior in patients exposed to anti-epileptics including gabapentin [34]. Given the prevalence of anti-depressant use and active clinical depression in our subjects, future research should examine interactions between gabapentin for the treatment of hot flashes and adverse side effects.
References
American Cancer Society. Breast cancer facts and figures, 2007–2008. Atlanta: American Cancer Society, Inc.
Hansen JA, Feuerstein M, Calvio LC, Olsen CH. Breast cancer survivors at work. J Occup Environ Med 2008;50(7):777–84.
Bradley CJ, Oberst K, Schenk M. Absenteeism from work: the experience of employed breast and prostate cancer patients in the months following diagnosis. Psycho-Oncol 2006;15(8):739–47. doi:10.1002/pon.1016.
Bradley CJ, Neumark D, Bednarek HL, Schenk M. Short-term effects of breast cancer on labor market attachment: results from a longitudinal study. J Health Econ 2005;24:137–60. doi:10.1016/j.jhealeco.2004.07.003.
Bradley CJ, Bednarek HL, Neumark D. Breast cancer survival, work and earnings. J Health Econ 2002;21:757–79. doi:10.1016/S0167-6296(02)00059-0.
Bouknight RR, Bradely CJ, Luo Z. Correlates of return to work for breast cancer survivors. J Clin Oncol 2006;24:345–53. doi:10.1200/JCO.2004.00.4929.
Drolet M, Maunsell E, Brisson J, Brisson C, Masse B, Deschenes L. Not working 3 years after breast cancer: predictors in a population-based study. J Clin Oncol 2005;23:8305–12. doi:10.1200/JCO.2005.09.500.
Satariano WA, DeLorenze GN. The likelihood of returning to work after breast cancer. Public Health Rep 1996;111:236–41.
Ahles TA, Saykin AJ, Furstenberg CT, Cole B, Mott LA, Skalla K, et al. Neuropsychologic impact of standard-dose systemic chemotherapy in long-term survivors of breast cancer and lymphoma. J Clin Oncol 2002;20:485–93. doi:10.1200/JCO.20.2.485.
Brezden CB, Phillips KA, Abdolell M, Bunston T, Tannock IF. Cognitive function in breast cancer patients receiving adjuvant chemotherapy. J Clin Oncol 2000;18:2695–701.
Mar Fan HG, Houede-Tchen N, Yi QL, Chemerynsky I, Fownie FP, Sabate K, et al. Fatigue, menopausal symptoms, and cognitive function in women after adjuvant chemotherapy for breast cancer: 1 and 2-year follow-up of a prospective controlled study. J Clin Oncol 2005; 23:8025–32.
Schagen SB, van Dam FS, Muller MJ, Boogerd W, Lindeboom J, Bruning PF. Cognitive deficits after postoperative adjuvant chemotherapy for breast carcinoma. Cancer 1999;85:640–50. doi:10.1002/(SICI)1097-0142(19990201)85:3<640:AID-CNCR14>3.0.CO;2-G.
Tchen N, Juffs HG, Downie FP, Yi QL, Hu H, Chemerynsky I, et al. Cognitive function, fatigue, and menopausal symptoms in women receiving adjuvant chemotherapy for breast cancer. J Clin Oncol 2003;21:4175–83. doi:10.1200/JCO.2003.01.119.
Maunsell E, Drolet M, Brisson J, Brisson C, Masse B, Deschenes L. Work situation after breast cancer: results from a population-based study. J Natl Cancer Inst 2004;96:813–22.
Hensley ML, Dowell J, Herndon JE, Winer E, Stark N, Weeks JC, et al. Economic outcomes of breast cancer survivorship: CALGB study 79804. Breast Cancer Res Treat 2005;91:153–61. doi:10.1007/s10549-004-6497-9.
Bonadonna G, Hortobagyi GN, Gianni AM. Textbook of breast cancer: a clinical guide to therapy. London: Martin Dunitz; 2001.
Lerner D, Amick BC, Rogers WH, Malspeis S, Bungay K, Cynn D. The work limitations questionnaire. Med Care 2001;39:72–85. doi:10.1097/00005650-200101000-00009.
Lerner D, Amick BC 3rd, Lee JC, Rooney T, Rogers WH, Chang H, et al. Relationship of employee-reported work limitations to lost work productivity. Med Care 2003;41:649–59. doi:10.1097/00005650-200305000-00012.
Feuerstein M, Hansen JA, Calvio LC, Johnson L, Ronquillo JG. Work productivity in brain tumor survivors. JOEM 2007;49(7):803–11.
Lerner D, Adler DA, Chang H, Berndt ER, Irish JT, Lapitsky L, et al. The clinical and occupational correlates of lost work productivity loss among employed patients with depression. J Occup Environ Med 2004a;46:S46–S55. doi:10.1097/01.jom.0000126684.82825.0a.
Lerner D, Adler DA, Chang H, Lapitsky L, Hood MY, Perissinotto C, et al. Unemployment, job retention, and productivity loss among employees with depression. Psychiatr Serv (Wash, D.C.) 2004b;55:1371–8. doi:10.1176/appi.ps.55.12.1371.
Adler DA, McLaughlin TJ, Rogers WH, Chang H, Lapitsky L, Lerner D. Job performance deficits due to depression. Am J Psychiatr 2006;163:1569–76. doi:10.1176/appi.ajp.163.9.1569.
Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomized trials. Lancet 2005;365:1687–717. doi:10.1016/S0140-6736(05)66544-0.
Mano MS, Awada A, Kerr J, Canney P. Adjuvant anthracycline-based chemotherapy for early breast cancer: do the dose and schedule matter? Cancer Treat Rev 2005;31:69–78. doi:10.1016/j.ctrv.2004.11.001.
Wefel JS, Lenzi R, Theriault RL, Davis RN, Meyers CA. The cognitive sequelae of standard-dose adjuvant chemotherapy in women with breast carcinoma: results of a prospective, randomized, longitudinal trial. Cancer 2004;100:2292–9. doi:10.1002/cncr.20272.
Ferrie JE, Kivimaki M, Head J, Shipley MJ, Vahtera J, Marmot MG. A comparison of self-reported sickness absence with absences recorded in employers’ registers: evidence from the Whitehall II study. Occup Environ Med 2005;62:74–9. doi:10.1136/oem.2004.013896.
Bower JE, Ganz PE, Desmond KA, Bernaards C, Rowland JH, Meyerowitz BE, et al. Fatigue in long-term breast carcinoma survivors: a longitudinal investigation. Cancer 2006;106:751–8. doi:10.1002/cncr.21671.
Ware JE, Snow KK, Kosinski M, Gandek B. SF-36 health survey: manual and interpretation guide. Boston: The Health Institute; 1993.
Shadbolt B, Barresi J, Craft P. Self-rated health as a predictor of survival among patients with advanced cancer. J Clin Oncol 2002;20(25):2514–18. doi:10.1200/JCO.2002.08.060.
Kaplan MS, Bertholet JM, Feeny D, McFarland BH, Khan S, Orpana H. The predictive validity of health-related quality of life measures: mortality in a longitudinal, population-based study. Qual Life Res 2007;16(9):1539–46. doi:10.1007/s11136-007-9256-7.
Brouwer WBF, van Exel NJA, Koopmanschap MA, Rutten FFH. Productivity costs before and after absence from work: as important as common? Health Policy (Amsterdam) 2002;61 (2):173–87. doi:10.1016/S0168-8510(01)00233-0.
US Census Bureau.American Community Survey. 2006 Table for the Rochester, New York Metropolitan Area. Last accessed online on August 28, 2008 at: http://factfinder.census.gov.
Pandya K, Morrow G, Roscoe J, Zhao H, Hickok J, Pajon E, et al. Gabapentin for hot flashes in 420 women with breast cancer: a randomized double-blind placebo controlled trial. Lancet 2005;366(9488):818–24. doi:10.1016/S0140-6736(05)67215-7.
US Food and Drug Administration Alert. January 31, 2008. Suicidality and Antiepileptic Drugs. Last accessed on-line on June 27, 2008 at: http://www.fda.gov/cder/drig/infopage/antiepileptics/default.htm.
Author information
Authors and Affiliations
Corresponding author
Additional information
Sources of Support: Department of Defense Breast Cancer Research Program Concept Development Award: “Chemo-Brain,” “Lost work productivity and Career Success: A Pilot Study” (DAMD 17-01-0785).
Rights and permissions
About this article
Cite this article
Lavigne, J.E., Griggs, J.J., Tu, X.M. et al. Hot flashes, fatigue, treatment exposures and work productivity in breast cancer survivors. J Cancer Surviv 2, 296–302 (2008). https://doi.org/10.1007/s11764-008-0072-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11764-008-0072-z