
Abstract
Introduction
Oncology health care professionals frequently lack the background to implement needed survivorship activities and follow-up care. The purpose of this project is to assist providers in the clarification and initiation of potentially durable changes in survivorship care by developing a health professional curriculum, recruiting participants, implementing the course, conducting course evaluation and following participants’ defined goals over time.
Materials and methods
The curriculum was developed based on recommendations from the Institute of Medicine Report-From Cancer Patient to Cancer Survivor—Lost in Transition. Three concepts were used to structure the course: cancer survivorship quality of life, changing practice via performance improvement, and principles of adult education. Expert faculty designed and implemented the curriculum and teaching methods using adult learning principles and an interactive approach. Competitively-selected, two-person interdisciplinary teams for the first course (July 12–15, 2006, Pasadena, California) were selected based on stated interests, three projected goals, and letters of commitment from administrators.
Results
Participants represented 52 cancer care settings from 28 states. Teams included Nurses (48.1%), Social Workers (20.7%), Physicians (18.8%), Directors/Administrators (6.6%), Psychologists (2.8%), and others (3%). The institutional barriers identified by teams were lack of survivorship knowledge (94 %), financial constraints (61%), lack of administrative support (6%), and staff philosophy that excluded survivorship (15%). Evaluation of content from the first course was consistently positive.
Conclusions
Dissemination of survivorship education for health care professionals stimulates participants to define and begin to implement goals for improving survivors’ care.
Implications for cancer survivors
A training program such as the one described provides professional knowledge regarding survivorship that has the potential to facilitate change in the health care that cancer survivors receive thus ideally improving long term health and well being.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
In 1971 cancer survivors numbered approximately 3.2 million [1, 4]. In 2006 these numbers have increased to over ten million individuals [16] The health needs of this population are different from those who have not survived a cancer diagnosis. These health needs are unique, related to both the cancer disease as well as the cancer treatment, and require surveillance and follow up care frequently unknown to the health care community [2–6]. Changes in the health care system are needed.
Recognition of the needs of cancer survivors has recently been addressed through the landmark publication by the Institute of Medicine, From Cancer Patient to Cancer Survivor—Lost in Transition [6]. This evidence-based report authored by a group of cancer researchers and cancer survivors reviewed research describing what is currently known about cancer survivors. Organizing the content under a four dimensional quality of life framework (physical, psychological, social and spiritual well being), the report illustrates what little is currently known about survivorship needs. The report addresses the areas for improving the research base and the care of cancer survivors. Ten recommendations are identified in the report, with one being the need for increased education of health care professionals on the needs of cancer survivors and coordination of care [6]. Models of professional education for improving survivorship activities need to be designed, implemented and evaluated to identify successful approaches to improve survivorship care.
The purpose of this paper is to describe a course developed to respond to the need for increased education of health care professionals in cancer survivorship and provide the foundation for survivorship programs across the US. While several specific objectives are addressed in the training program including: (1) development of the cancer survivorship curriculum, (2) recruitment of health professional teams to attend an intensive cancer survivorship course, (3) identification of evaluation methods for the course, (4) description of support activities following the course and (5) description of participating institutions and their projected post course goals, the present paper describes the program and provides some initial descriptive data.
Improvements in care of cancer survivors need to begin with the education of health professionals who can initiate needed changes in settings that care for these patients. Health professionals cannot practice what they do not know. However, passive education alone is insufficient to change behavior and systems [7]. The education needed must reach beyond the classroom to include support of participants following educational activities. This project builds on approaches used by the authors to successfully change approaches to care in pain management and end of life [8–10]. Recognizing that providing knowledge alone is not sufficient to lead to a change in behaviors, our goal was to provide teaching strategies that facilitate behavior change in an effort to initiate and sustain a change in the actual delivery of care [7].
Materials and methods
Curriculum development
The development and implementation of the survivorship curriculum was made possible by support from the National Cancer Institute, National Institutes of Health [11]. Four annual three-day courses are planned between 2006–2009. The first course took place in July 2006. The grant provides resources for recruiting nationally known faculty to assist in development and implementation of curriculum content, travel stipends to accepted participants, and support for a rigorous evaluation of the results of participants’ goal implementation following the intensive course at 6, 12, and 18 months.
The educational framework for designing the curriculum included three concepts: Cancer Survivor Quality of Life, Changing Practice via Performance Improvement, and Principles of Adult Education. These three concepts were woven together to provide the content and teaching methods for the survivorship curriculum (Fig. 1). Each of these concepts guided the development of the content and teaching methods used in this course.

Framework.
The first concept, Cancer Survivor Quality of Life, was used to identify course content. This content was designed from two primary documents: the evidence-based content in the IOM report, this was organized under the four-dimensional quality of life model [6] (Fig. 2), and The Quality Cancer Care—Declaration of Principles, published by the National Coalition of Cancer Survivorship (NCCS) in 1996 [12] (Table 1). These two documents were combined with a rigorous literature review conducted by faculty selected for their expertise in the dimensions of quality of life and survivorship experience.

Quality of life model for cancer survivors.
The second concept used to design the course was the concept of changing practice via performance improvement. Changing practice in clinical settings is a major challenge [13]. Previous work by the research team had identified several approaches that have resulted in changing practice in pain management and end-of-life care [14–17]. For example, to assure that organizational change projects were identified, participant teams were selected based on background, interest statements, and projected goals to be implemented following the course. To assure support for change by organizations, letters of commitment from two hospital administrators from each institution were required. The concept of performance improvement includes information on quality assurance and focus on the challenge of institutional change. Presentations on these topics were placed throughout the curriculum, and participants were given time to refine their post course goals to fit performance improvement activities at their individual institutions.
For the third concept of the framework, principles of adult education were identified in studies by the National Research Council (Table 2) [18]. The first principle focuses on the learner. The adult learner is self directed, having a resource of life experience, is ready to learn, and concerned about solving problems [19, 20]. These aspects were emphasized to course faculty, and used to provide for discussion periods, case study use, demonstrations, and small group work. Effective educational models include: active learner engagement through interactive goal based strategies which provide an impetus to implement change. Multifaceted activities that allow for networking and collegial relationships and sharing of success stories or strategies were used [8, 20] (Table 2).
The knowledge, attitude and skills the participants would bring to the program and their comfort with working collaboratively was important. Part of the application requirement was the inclusion of two-person teams and statements of interest by each applicant. Inclusion of pre-course goals in the application provided for assuring that the content presented matched the learner’s goals.
The second adult learning principle used in the present training program is providing knowledge centered education. This principle emphasizes the need for faculty who are experts in the content to be taught, as well as being expert teachers. Expert faculty were identified and asked to synthesize material under a specific topic area (e.g. physical well being of cancer survivors). The content was reviewed by the course director and co-investigators. Recommendations for refinement of material and development of slides were sent to the faculty, and a final product was designed and agreed on by all.
The third principle is that the learning experience needs to be assessment centered, focusing on the need to assess changes in knowledge, behavior, or activities resulting from the course. The application process required three goals that were refined throughout the program. Revisiting these goals during the course demonstrated how participants were able to develop survivorship goals based on course content and interaction with faculty.
The fourth learning principle applied was that leaning needs to be community-centered. This principle focuses on what happens to the participant learner as he or she returns to their community, as well as the community within the training program. Several activities occurred to provide resources to participants after the course. Names and addresses including e-mails for all participants and faculty were provided so that contacts could continue after the course. Also a newsletter was developed and sent out every 3 months following the course the newsletter included new resources as available and featured achievements of specific participants [22].
In addition to these four adult education principles we were also concerned about creating an environment that encouraged participant communication, interaction and support. The environment needed to be comfortable and participants needed to be provided with meals and opportunities for communal interactions [8, 18]. To facilitate interactions among the participants and the faculty, an informal reception was held the evening before the course. Light refreshments were served, and conversation among participants and faculty were encouraged. The Lilly art display, “Lilly Oncology on Canvas-Expressions of a Cancer Journey” was obtained [14]. This is a patient centered art program that allows those affected by cancer an opportunity to express their feelings and emotions in their journey to healing and hope. The art display provided a background for discussion among participants and faculty.
In summary, development of the curriculum included a number of activities. The overall course objective was to describe the current status of adult cancer survivorship in the United States and to recognize the impact of cancer survivorship on quality of life. After several reviews by individual faculty and the course directors, a final agenda was developed, and consisted of State of the Science Sessions on the four quality of life domains, long-term follow up content specific to the pediatric population, and many examples of specific survivorship activities (Table 3). Plenary sessions, concurrent smaller group sessions, and small group activities were developed. The first and second day ended with small group work on participants’ goals. The pediatric population was addressed separately, to provide adequate content on the life-long effects of cancer and its treatment on this specific population. Expert faculty were selected to present current successful examples of activities under each dimension. A two and a half day course resulted. A list of participating faculty is found in Table 4.
Recruitment and selection of teams
The application process to attend the course was designed to facilitate team commitment and institutional support. A competitive selection process was conducted by the authors based on background, interest statements, projected goals, representative disciplines, and geography. A competitive application promotes active learning [8]. Eligibility requirements included a team of two professional members of an institution, with at least one member being a nurse, physician, or an administrator. The second member could be one of the same, or other professionals potentially involved in survivorship activities at the institution. We expected to have teams that included rehabilitation experts, pharmacists, social workers, spiritual counselors, and a variety of others.
The application form identified who the two team members were, professional credentials and background, and statements of interest in attending the course. Previous experience with survivorship activities was requested. Institutional commitment was obtained by requiring applications be accompanied by two letters of commitment and support from the Director of Nursing/Patient Care Services, the Chief of Staff/Medical Director or an Institutional Administrative Official. This requirement encourages communication among administrators and participants and provides administrative support [8].
Recruitment activities involved a mailing to all the NCI-designated cancer centers, as well as those cancer centers belonging to the Association of Community Cancer Centers. Mailings were directed to the administrator of the institution as well as someone involved in educational activities. Other mailing lists were obtained from the many other educational activities presented by the authors. Advertisements were placed in professional journals, and flyers were developed to distribute at local and national professional meetings attended by the authors. A website was developed for potential applicants to obtain information on the course, and to download the application form [23].
Evaluation of initial program
Evaluation began with materials submitted prior to the course, and will continue up to 18 months post course. The application form provided background, educational status, discipline, and survivorship interest statements from each team member. The institutions were described in relation to cancer center status, population served, and geographic location. Once accepted, several additional descriptive questionnaires were required. The institutional assessment was a questionnaire about what survivorship services and activities were currently available at an institution. This questionnaire is repeated 12 months later. The institution survey is a short form for participants to identify their view of the institution’s readiness to change. It is repeated at 6 and 12 months post course.
The course itself was evaluated with standardized forms on faculty, content, and teaching methods. One of the most important evaluation components is that of goal refinement and follow-up. Each team submitted three goals with their application. These goals were refined during the course according to principles of institutional change, and then followed up regarding implementation and completion at 6, 12, and 18 months post course. With these evaluation approaches, both team accomplishments and institutional change are examined.
Follow-up support post course
Sustaining interest of participants to implement institutional changes when they return home following the course is a major challenge of every educational endeavor. For this survivorship course, several follow up approaches were implemented in order to keep participants engaged and provide additional resources. The extensive syllabus provided to each participant included all course content, slides, bibliographies, resources, and faculty and participant addresses. The participant lists were organized three ways: alphabetized by last name, by institution, and by state. Thus it was easy for a participant to connect with someone for a local collaborative activity such as setting up a joint support group for a specific disease. Also, project personnel and faculty were available by phone and e-mail to participants seeking more information, clarification, and general support.
However, we did not wait until they contacted us. We began a quarterly Newsletter that provided information on additional resources, other survivorship courses, and identified specific projects that course participants were implementing. The first Newsletter was e-mailed to all participants, as well as administrators, 2 months after the course in an effort to keep people tuned in to the cancer survivorship movement. Participant and institution names are highlighted. A website specifically for the course participants was created. Additional resources such as journal articles, news clips, and other resources are available on the website. Post course evaluation of goal achievement at 6, 12, and 18 months will provide an opportunity to evaluate what goals have been achieved as well as provide support and suggestions to those teams meeting institutional barriers. These evaluations are completed on the telephone, with an appointment made in advance and a goal evaluation sheet used to record progress. Participants frequently describe challenges and barriers during the telephone calls, and the project director conducting these interviews can provide resources and suggestions to surmount these challenges.
Results-first course
Course participants came from across the United States, representing 28 states, and located primarily on the east coast (Fig. 3). Institutional settings most commonly represented either an adult outpatient setting, or a combined adult and pediatric outpatient setting (Table 5). The primary cancer survivor population the participants work with were adults (71%). Participants came from a variety of disciplines, with nurses representing almost half of the participants, then social workers and physicians. The most common team configuration was nurse/social worker (31%). Nurse/physician teams represented 21% of the participants, and nurse/nurse teams 19%. While we did attract teams with second tier members from rehabilitation, pharmacy, and spiritual counselors, teams were composed of disciplines considered essential to implementing institutional change. For future courses, recruitment will target these second tier applicants as a way to expand the variety of survivor services and activities being implemented among participating institutions.

US map of participants.
Course evaluations were positive. Faculty was evaluated on a 5 point scale with 5 being the highest score. For clarity of presentation the mean score was 4.63 with individual faculty scores ranging from 4.16 to 4.96. Scores for quality of presentation averaged 4.6 and ranged from 4.19 to 4.96. Scores for value to the participant averaged 4.43 and ranged from 3.92 to 4.91.
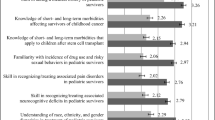
The institutional survey submitted prior to the course assesses how easily participants expected to be able to implement new survivorship activities in their institutions following the course. The survey is scored from 0 to 10 with 0 being not effective and 10 being very effective. Figure 4 illustrates the scores and provides evidence of anticipated administrative and staff support, with a clear need to improve effectiveness of survivorship care along with increasing the comfort of staff in providing this care. In response to requesting information on anticipated barriers, participants identified a lack of knowledge related to survivorship needs and care as the most frequent barrier anticipated, with financial constraints identified by well over half of the participants (Fig. 5). Only 10% of the participants anticipated a lack of administrative support.

Institutional survey.

Institutional barriers.
A total of three goals per institution resulted in a final list of 156 individual goals to be used in following participants’ progress in implementing course content. The goals were examined and divided into a number of major categories. Goals addressed educational endeavors; changes in organizational structure; development of new clinical processes; specific survivorship activities; and research on survivorship (Table 6). Follow up evaluation at 6, 12, and 18 months will address specific progress participants have made in implementing these goals. While this evaluation has not yet occurred, communication with some of the teams has identified early achievements.
The early progress our participants have achieved has thus far been described through anecdote. Team highlights have been included in our newsletters to all participants and have identified specific team achievements. One large teaching institution conducted a needs assessment of over 80 cancer survivors, held a retreat to discuss plans for the clinic development and projected a timeline for implementing these plans. A senior nurse executive presented a poster on the APN-run Survivorship Clinic to a national senior nurse executives’ meeting. Another team has focused on identifying resources already available at their institution by developing relationships between the cancer center and the Women’s Health Program to meet survivorship issues. At another institution The Institute of Medicine’s video describing the survivorship movement and the IOM-Report “From Cancer Patient to Cancer Survivorship-Lost in Transition” were used during a grand rounds presentation to provide an overview of survivorship issues and to generate discussions within their institutions [22]. It is well recognized that health care change involves a process of many factors and this professional training program represents one major element in this process.
Discussion
Our efforts to respond to one of the recommendations of the IOM report on From Cancer Patient to Cancer Survivor: Lost in Transition [6], led to the development and implementation of a course addressing the educational needs of health care professionals. The course curriculum development process combined a rigorous literature review by expert faculty and was associated with the success with which the participants viewed the course. Adult learning strategies were supported including interactive, multifaceted and personalized activities [19, 20]. Short term anecdotal evaluation of the program indicated that the majority of the participants viewed the training as meeting their goals and objectives.
We designed this course to attract multidisciplinary teams who were competitively selected, and represented a variety of health care settings and geographic locations. Our marketing approaches were successful in attracting a large group of applicants from a variety of states. The teams were composed of a number of disciplines, with the largest group being nurses, followed by social workers and physicians (Table 5). Future efforts will continue to target these disciplines plus other participants from rehabilitation, pharmacy and spiritual counseling.
Participants’ views of their institutions prior to attending the course revealed the need for improvement in survivorship care, as well as an increase in comfort of staff providing care for this population. In identifying anticipated barriers, a lack of knowledge about survivorship care was identified as the most common barrier, and points to the need for educational efforts at most of the institutions. Only 10% anticipated a lack of administrative support in carrying out goals following the course. Evaluation of follow up changes in response to specific goals at 6, 12, and 18 months will be needed to reveal whether or not these expectations will be met and if changes can be sustained over time. Follow-up goal evaluations will document the percentage of goal achievement and provide specific information on actual institutional changes and their impact on survivorship care. Clearly, over the long run this training effort requires more rigourous evaluation (e.g., PRO) to determine its specific effects. The current effort is directed at maximizing the training approach to facilitate actual practice changes that have the potential to improve the quality of health care and quality of life of cancer survivors.
Conclusions
In summary, this paper describes one model of a professional educational program to help facilitate change in the health care that cancer survivors receive post treatment. The first of the four annual courses on Survivorship Education for Quality Cancer Care shows initial success in attracting appropriate attendees ( in terms of background experience, interest and institutional support), developing a comprehensive curriculum, and implementing a robust course. Initial follow-up comments from participants indicate that survivorship activities at many of the facilities where these participants work have already begun. Further evaluation at 6, 12, and 18 months will be needed to identify the degree of change and how enduring institutional changes will be. Meanwhile, the first fifty-two teams from across the United States are currently involved in changing the face of survivorship care for cancer patients.
References
Estimated U.S. Cancer Prevalence. [online]. Available: http://cancercontrol.cancer.gov/ocs/prevalence/prevalence.html [accessed December 17, 2006].
National Coalition for Cancer Survivorship (1999). Turning Hope into Action. Silver Spring, MD, National Coalition for Cancer Survivorship.
National Coalition for Cancer Survivorship (2006). Pioneering Survivorship—20 years of advocating for quality cancer care. http://www.canceradvocacy.org.
About Survivorship Research: Survivorship Definitions. [online]. Available: http://dccps.nci.nih.gov/ocs/definitions.html [accessed December 17, 2006].
Committee on Cancer Survivorship: Improving Care and Quality of Life. National Cancer Policy Board. (2006) From cancer patient to cancer survivor—lost in transition. Washington, D.C: The National Academies Press http://www.nap.edu).
Ferris, F., Von Gunten, C., Emanuel. (2001). Office of Cancer Survivorship. http://www.psycho-oncology.net/Bethesda.html
Ferrell, B., Grant, M., Borneman, T., Juarez, G., & Virani, R. (2002). Strategies for effective continuing education by oncology nurses. Oncology Nursing Foundation, 29(6), 907–909.
Rogers, E. (1962). Diffusion of innovations. New York: The Free Press.
Ferrell, B., Virani, R., Grant, M., Rhome, A., Malloy, P., Bednash, G., & Grimm, M. (2005). Evaluation of the End-of-Life Nursing Consortium undergraduate faculty training progam. Journal of Palliative Medicine, 8(1), 107–114.
NCI Grant (2006) IR25-CA107109-01 Survivorship Education for Quality Cancer Care.
Clark, E. J., Stovall, E. L., Leigh, S., Siu, A. L., Austin, D. K., & Rowland, J. H. (1996). Imperatives for Quality Cancer Care: Access, Advocacy, Action, and Accountability. National Coalition of Cancer Survivorship, 7–8.
Walrath, J. M., Mugan;inskaya, N., Shepherd, M., Award, M., Reuland, C., Makary, M. A., et al. (2006). Interdisciplinary medical, nursing, and administrator education in practice: the Johns Hopkins experience. Academic Medicine, 81(8), 744–748.
Grant, M., Rivera, L., Alisangco, J., & Francisco, L. (1999). Improving cancer pain management using a performance improvement framework. Journal of Nursing Care Quality, 13(4), 60–72.
Ferrell, B. R., & Virani, R. (1998). Institutional commitment to improved pain management: Sustaining the effort. Journal of Pharmaceutical Care in Pain & Symptom Control, 6(2), 43–55.
Ferrell, B. R., Dean, G. E., Grant, M., & Coluzzi, P. (1995). An institutional commitment to pain management. Journal of Clinical Oncology, 13, 2158–2165.
Grant, M., Hanson, J., Mullan, P., Spolum, M., & Ferrell, B. Disseminating End-of-Life Education to cancer centers: Program review and evaluation (Submitted 2006)
Bransford, J. D., Brown, A. L., & Cocking, R. R. (2000). Principles adapted from National Research Council—“How People Learn” Brian, Mind, Experience and School. Washington DC: National Academy Press.
Knowles, M. S. (1973). The adult learner. A neglected species. Houston, TX: Gulf Publishing.
Sullivan, A. M., Lakoma, M. D., Billings, J. A., Peters, A. S., Block, S. D., & the PCEP Core Faculty. (2006). Creating Enduring Change-Demonstrating the Long-Term Impact of a Faculty Development Program in Palliative Care. Journal of General Internal Medicine, 21, 907–914.
http://www.lillyoncology.com/oncology_canvas/2006_index.jsp [accessed December 18, 2006].
Survivorship Education for Quality Cancer Care Newsletter. 2006 September.
Acknowledgement
Funding Source–National Cancer Institute. 1-R25-CA 107109-01 Survivorship Education for Quality Cancer Care
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Grant, M., Economou, D., Ferrell, B. et al. Preparing professional staff to care for cancer survivors. J Cancer Surviv 1, 98–106 (2007). https://doi.org/10.1007/s11764-007-0008-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11764-007-0008-z