
Abstract
Introduction
Despite a shift in the cancer culture and language used to describe individuals diagnosed with this disease, the extent to which individuals with cancer adopt a particular cancer-related identity and the impact of these identities in relation to their well-being is virtually unknown.
Materials and methods
Using a cross-sectional study design and a metropolitan tumor registry, a mail questionnaire to examine post-treatment quality of life was sent to prostate cancer (PCa) survivors. The sample consisted of 490 PCa survivors, ranging in age from 49–88 (M = 69.7; SD = 7.8), one to eight years after diagnosis. The outcome measure used in these analyses was the PANAS to assess positive and negative affect.
Results
The most frequently reported cancer-related identity was “someone who has had PCa” (57%). The least reported self view was “victim” (1%). Twenty-six percent of men self-identified as “survivors” while 6% thought of themselves as “cancer conquerors.” Only 9% self-identified as a “patient.” Multivariate analyses, adjusted for potential confounders, show respondents who identified themselves as “survivors” or “cancer conquerors” reported significantly higher scores on positive affect than men who self-identified as “patients” (p < .001).
Conclusions
Although the majority of respondents identified themselves as “someone who has had cancer,” identifying as a “survivor” or “someone who has conquered cancer” appears to have adaptive value for positive mood.
Implications for cancer survivors
Those who perceive themselves as survivors of prostate cancer may derive some benefit in well-being associated with this self assessment.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
In recent years, expressions, such as “cancer survivor” have replaced more traditional labels, namely, “victim” and “patient” for those diagnosed with cancer. Both the National Coalition for Cancer Survivorship [10] and the Office of Cancer Survivorship at the National Cancer Institute [13] have adopted the more active term “cancer survivor” as a way to recognize this shift in the cancer culture and in recognition of the unique needs of this growing population. Despite this change in the cancer ethos, the extent to which individuals with cancer adopt one or another particular cancer-related identity is virtually unknown. Moreover, research suggests that individual’s adoption of a more active cancer-related identity, such as “cancer survivor” may have positive consequences for their health and well-being. [5, 17]
Identity theory, derived from symbolic interactionism, suggests that one’s self concept is socially constructed and reflects one’s interactions with others and society. [4, 12] As individuals with cancer construct and share their story with others, including members of their healthcare team, they create and recreate themselves and redefine the meaning of having cancer. [9] These stories are embedded in a specific cultural and historical context, which assumes reciprocity among its components. Identity theory provides a valuable framework for examining the impact that the survivorship experience and interactions with others has had on the way individuals with cancer see themselves [5] and how different cancer-related identities may be associated with well-being.
Positive and negative affect are two important components of psychological well-being. Research has shown that low positive affect and high negative affect are associated with higher anxiety and depression in survivors of breast, colorectal and prostate cancer. [15] Information on the extent to which individuals with a history of cancer adopt a specific cancer-related identity and its effects may provide clinicians engaged in providing care to these individuals with potentially useful information to help improve their well-being. [14]
Our review of the literature identified two studies that have examined adoption of different identities following a cancer diagnosis. First, a recent longitudinal study of 321 long-term (> 5 years from diagnosis) survivors of colon, breast or prostate cancer showed 86% of the sample identified as a “cancer survivor,” 13% saw themselves as a “patient” while an additional 13% adopted a “victim” orientation. [5] Respondents could have chosen more than one label. This pattern is in contrast to a cross-sectional study conducted almost a decade earlier by the same research team in which 22% of men and women (N = 50) diagnosed with a range of cancers (60% of sample < 5 years from diagnosis) indicated that they identified as a “patient” and 30% considered themselves to be a “victim.” [6] Other work from a qualitative approach has examined identity through the examination of narrative accounts of the experience of survivors of colon cancer, Hodgkin’s lymphoma and hepatoblastoma (1–25 years post diagnosis). [11] These findings suggest that cancer can threaten the element of continuity in one’s identity and that efforts to restore stability are a difficult task for some survivors, perhaps with implications for long term adjustment and well-being.
The purpose of this study was to examine (1) how men with prostate cancer self-identify, and (2) the extent to which these perceived cancer-related identities are associated with positive and negative affect. Based on limited extant research, we hypothesized that men post treatment for prostate cancer who self-identify as a survivor or conqueror, as compared with victim or patient will report higher levels of positive affect and lower levels of negative affect.
Materials and methods
Study overview
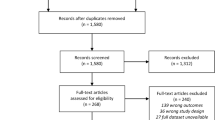
This study was part of a larger study examining predictors of health and function in men with prostate cancer. Details of the study design and recruitment procedures have been published elsewhere. [3] In brief, questionnaires were mailed to 1,500 prostate cancer survivors from a metropolitan tertiary care hospital cancer registry. The mailing resulted in 490 completed questionnaires, which represents a 34% response rate after excluding the 70 surveys that were returned as undeliverable. Respondents were similar to the total population in the cancer registry in terms of age at diagnosis, time since diagnosis, stage of diagnosis and primary treatment.
We analyzed data from 490 men with prostate cancer ranging in age from 49–88 (Mean age = 69.7, SD = 7.85). The average time since diagnosis was 46.7 months with a range from 1 to 8 years post diagnosis. Primary treatment was assessed via self-report and the distribution was as follows: 51% of men received surgery, 42% received radiation (mostly external beam radiation), and 3% received hormonal therapy (4% of the treatment data was missing). Three quarters who reported initial Gleason scores had scores of 5, 6, or 7, indicating relatively non-aggressive disease in the sample overall.
Measures
Perceived cancer-related identity
We used a single-item question to assess how individuals view themselves. We asked “when you think about yourself in relation to your prostate cancer, which adjective or phrase best describes you: a patient, a victim, someone who has had prostate cancer, cancer survivor, or cancer conqueror?” “Someone who has had prostate cancer” was included because research shows that a considerable number of men see their prostate cancer as in the past and of little impact on their current lives, and this self description seemed appropriate to reflect that group [2, 3, 7, 8]. Respondents were only allowed to endorse one of the five labels.
Positive and negative affect
The Positive and Negative Affect Schedule (PANAS) was used to measure affect, both positive and negative. [16] This scale contains 20 descriptive mood adjectives such as determined, proud, hostile, and inspired. High Positive Affect (PA) “is a state of high energy, full concentration, and pleasurable engagement, whereas low PA is characterized by sadness and lethargy. In contrast Negative Affect (NA) is a general dimension of subjective distress and unpleasurable engagement that subsumes a variety of aversive mood states, including anger, contempt, disgust, guilt, fear, and nervousness, with low NA being a state of calmness and serenity.” Participants rated the degree to which they experienced different moods using a 5-point Likert scale with 1 being “not at all” and 5 “very much.” Scores range from 0 to 50 with higher scores indicative of elevated affect. The positive and negative affect scales demonstrated good internal consistency with Cronbach’s alphas = 0.83, 0.87, respectively.
Analytic overview
Descriptive statistics were conducted to assess the prevalence of adopting a specific cancer-related identity following primary treatment for prostate cancer. Two hierarchical linear regression models were estimated with positive and negative affect as dependent variables and cancer-related identity (with multiple levels) as the main independent variable of interest; thus entered into the model last. The following covariates were associated with at least one of the dependent variables and were therefore included in the model to control for confounding: age, race, marital status, comorbid conditions and time since diagnosis. We used “patient” identity as our reference group because we were interested in comparing differences between positive or active descriptors of oneself “survivor” and cancer “conqueror” to the more traditional/passive and negatively oriented language more typically used in the past.
Results
Respondents were significantly more likely to identify as a survivor or conqueror compared with victim or patient (p < 0.001). The most frequently reported self-identifying label for men in our sample was “someone who has had prostate cancer” (57%) (Fig. 1). The least reported identification label was as a “victim” (1%). Nine percent of respondents identified as a “patient.” Lastly, 26% of men self-identified as “survivors” while 6% thought of themselves as “cancer conquerors.” The mean PANAS positive affect score for the sample was 34.3 (S.D. = 7.2) and the mean negative affect score was 14.2 (S.D. = 4.5).

How men with prostate cancer describe themselves 1–8 years post diagnosis (N = 478). Percents don’t add up to 100% because of missing data (n = 9).
Separate linear regression analyses, adjusted for potential confounders, were conducted to examine the independent association between adopting different cancer-related identities and positive and negative affect. Results showed a significant overall association between identity and positive affect, \( F_{\Delta } {\left( {4,448} \right)} \) = 4.75, p = 0.001, but a nonsignificant omnibus association with negative affect. \( F_{\Delta } {\left( {4,446} \right)} \) = 0.29, p = 0.883. Table 1 presents coefficient estimates, standard errors and corresponding p-values derived from Student t-tests. Men who self-identified as a “survivor” or “conqueror” reported higher levels of positive affect compared with men who adopted a “patient” orientation (p-values for both associations were less than 0.05).
Discussion
Respondents were more likely to identify with positively oriented labels, specifically, as a survivor or conqueror compared with negatively oriented labels (i.e., patient and victim). In our sample, however, the most frequently reported perceived identification label was “someone who has had cancer.” This latter finding suggests there may be minimal identity change in any direction, for men treated for prostate cancer. This assertion is further supported by other post hoc analyses conducted in this study. Specifically, 71% of individuals who self-identified as “someone who has had cancer” also reported that they “hardly ever think about their disease” indicating that cancer is not a significant part of their lives, at least for these men who are on average 4 years post treatment. However, those who perceive themselves as a “cancer survivor” or “cancer conqueror” do report higher positive affect compared with those who endorse the “patient” label indicating a potential benefit for self-identifying with a positively oriented cancer-related identity.
The more traditional passive labels with negative undertones, including “victim” and “patient” were seldom used in our sample of men. This finding is different from previous studies that found a higher proportion of individuals with cancer (a variety of types) self-identifying as a “victim” (13–30%) or “patient” (13–22%). [5, 6] These differences might be explained by the lack of variation in prognostic factors in our study. This study is the only one to include exclusively men with prostate cancer, which generally has a good prognosis. Most of the men in our sample had non-aggressive disease with favorable outcomes, whereas more variation in site, age and in prognostic factors existed in previously cited studies. We know from related work that men with favorable cancer outcomes report little impact of cancer on their lives [2, 3, 8], so it is not surprising to find men do not see themselves as a “victim” or “patient.” This point is further supported by our finding that the majority of men in our study reported identifying themselves as “someone who has had cancer.” In a related vein, only 26% of respondents indicated that they considered themselves to be survivors, compared with 86% in a previous study of identity and survivorship in a sample of colon, breast and prostate cancer at least 5 years post treatment. [5] Again, this difference may be due to the homogeneity in demographic and prognostic factors and low level of disease severity in our study. Conversely, in both cases there is an equally valid argument that our study was the only one that provided “someone who has had cancer” or a similar choice as a possible response. Other studies only included clearly positive or negative options. Thus, many respondents in these studies may have chosen “survivor” as the closest to their position rather than “patient,” which many feel implies active treatment, or “victim,” which they may feel is too negative. Because we know that many people do, in fact, see their cancer as something in the past, it is quite possible that many of the people who chose “survivor” in the other studies, if given the opportunity would have chosen the more neutral “someone who has had cancer” to reflect more appropriately their lack of a cancer-related identity. Future studies of identity and well-being should focus on examining disease sites with more variation in stage of disease and survival prognosis and use a sufficiently broad range of possible “labels” or identities as response choices. Moreover, future research might also focus on the impact of adopting a survivor orientation on the use of self management approaches (e.g., lifestyle changes, coping strategies) to individual’s physical and mental health.
Our findings must be considered within the limitations of our research. Some of the confines of the study include our inability to generalize these findings to men with more advanced disease. However, men diagnosed with advanced stage prostate cancer represents a relatively small percentage (< 10%) of the population of prostate cancer survivors. [1] Also, men in our study may not be representative of the broader population of men with localized prostate cancer because participants were more likely to be white and of higher SES than the typical man with localized prostate cancer in the US. Nonetheless, our sample was similar to the larger cancer registry sample, in terms of age at diagnosis, time since diagnosis, and stage of disease.
More generally, including only men who have prostate cancer is both a limitation and strength; on the one hand, it restricts generalizability, but on the other hand, it allows for less variation of prognostic factors by site of disease. Also, the relatively large sample size leads to greater confidence that the results accurately reflect the population of focus in the study. The cross-sectional nature of our data prevents us from making any causal associations between cancer-related identity and affect. It is possible that men who are high on positive affect in general are also those who adopt a “survivor” mentality. Longitudinal research could help address this limitation. As one of few studies that have looked at the adoption of different cancer-related identities and in turn how these identities relate to positive and negative affect, these data are of potential significance despite the limitations.
Clinicians who provide care to survivors of cancer should be mindful of the language used to depict those people they are treating. Perhaps using language implying a more active view of life after treatment, such as “cancer survivor” as opposed to “patient” during office visits might prove to be influential in how these individuals see themselves and ultimately their actions to become active participants in their long term management. This is especially important in light of the current findings that show a positive relationship between self-identifying as a “cancer survivor” and higher positive affect. Future research should investigate the role clinicians might play in individual’s adoption of a particular cancer-related identity.
In summary, these findings show that years after treatment many prostate cancer survivors feel little need to form a significant part of their identity around their cancer experience. Research on these individuals might help identify factors that impact this adaptive response. Also, to fully understand the meaning of cancer survivorship, it might be useful to be informed about the degree to which cancer is—or is not—a significant part of one’s identity. This knowledge may prove to be useful in long-term management of these cases. While longitudinal studies could help clarify the direct link between self perceived cancer-related identities, well being and actual use of self management strategies to optimize health, survivors of prostate cancer may derive some benefit in well-being from viewing themselves in relation to the cancer in a positive light.
References
American Cancer Society (2006). Cancer facts and figures. Atlanta, GA: American Cancer Society.
Bellizzi, K. M. (2004). Expressions of generativity and posttraumatic growth in adult cancer survivors. International Journal of Aging and Human Development, 58, 247–267.
Blank, T. O., & Bellizzi, K. M. (2006). After prostate cancer: Predictors of well-being among long-term prostate cancer survivors. Cancer, 106(10), 2128–2135.
Cooley, C. H. (1902). Human nature and the social order. New York: C. Scribner’s Sons.
Deimling, G. T., Bowman, K. F., & Wagner, L. J. (in press). Cancer survivorship and identity among long-term survivors. Cancer Investigation.
Deimling, G. T., Kahana, B., & Schumacher, J. (1997). Life-threatening illness: The transition from victim to survivor. The Journal of Identity and Aging, 2, 164–186.
Eton, D., Lepore, S., & Helgeson, V. (2001). Early quality of life in patients with localized prostate carcinoma. Cancer, 92, 1451–1459.
Eton, D., & Lepore, S. (2002). Prostate cancer and health-related quality of life: A review of the literature. Psycho-Oncology, 11, 307–326.
Ford, L. A., & Christmon, B. C. (2005). Every breast cancer is different: Illness narratives and the management of identity in breast cancer. In E. B. Ray (Ed.), Health communication in practice: A case study approach. vol. Xxii (pp. 157–169). Mahwah, NJ: Erlbaum.
Hoffman, B. (2004). A cancer survivor’s almanac: Charting your journey (3 ed.). Hoboken, NJ: Wiley.
Little, M., Paul, K., Jordens, C. F. C., & Sayers, E.-J. (2002). Survivorship and discourses of identity. Psycho-Oncology, 11, 170–178.
Mead, G. H. (1967). Mind, self and society: From the standpoint of a social behaviorist. Chicago: University of Chicago Press.
National Cancer Institute. Cancer Survivorship Research Website: http://dccps.nci.nih.gov/ocs/.
Sparks, L., & Mittapalli, K. (2004). To know or not to know: The case of communication by and with older adult Russians diagnosed with cancer. Journal of Cross-Cultural Gerontology, 19, 383–403.
Voogt, E., Van Der Heide, A., Van Leeuwen, A. F., Visser, A. P., Cleiren, M. P. H. D., Passchier, J., et al. (2005). Positive and negative affect after diagnosis of advanced cancer. Psycho-Oncology, 14(4) 262–273.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures of positive and negative affect: The PANAS Scales. Journal of Personality and Social Psychology, 54, 1063–1070.
Zebrack, B. (2000). Cancer survivor identity and quality of life. Cancer Practice, 8(5), 238–242.
Disclaimer
The ideas and opinions expressed herein are those of the authors, and endorsement by the National Cancer Institute and University of Connecticut is not intended nor should be inferred.
Funding
This study was supported by the National Institute of Aging, 1-R0317728 to the University of Connecticut (T. O. Blank, PI).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bellizzi, K.M., Blank, T.O. Cancer-related identity and positive affect in survivors of prostate cancer. J Cancer Surviv 1, 44–48 (2007). https://doi.org/10.1007/s11764-007-0005-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11764-007-0005-2