
Abstract
A 60-year-old man received mitral valve repair via right mini-thoracotomy, which was followed by unilateral re-expansion pulmonary edema on the right side and severe hemoptysis just after the surgery. Despite differential lung ventilation with unilateral high positive end expiratory pressure was initiated for the affected right lung, respiratory function did not improved and hemodynamics was collapsed in the next day. Veno-venous extracorporeal membrane oxygenation was initiated by cannulation of the right jugular and the left femoral vein. After pulmonary function recovered gradually, veno-venous extracorporeal membrane oxygenation was terminated on the fifth postoperative day. He was discharged in ambulatory condition on postoperative day 52.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Re-expansion pulmonary edema (REPE), a complication of chronically collapsed lungs, occurs after drainage of the pneumothorax or pleural effusion, with an incidence of approximately 1 % [1]. Although few cases of fatal REPE after one-lung ventilation surgery have been reported, definite treatment has not yet been established. Here, a case of severe REPE after mitral valve repair with right mini-thoracotomy treated by veno-venous extracorporeal membrane oxygenation (V-V ECMO) is described.
Case
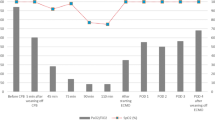
A 60-year-old man was admitted with dyspnea on exertion, atrial fibrillation, and a diagnosis of congestive heart failure (CHF) with the NYHA class IV. Trans-thoracic echocardiography (TTE) showed severe mitral regurgitation due to prolapse of the posterior leaflet, moderate tricuspid valve regurgitation, and ejection fraction of 37 %. Coronary arteriography detected no significant finding. One month after recovery from CHF by medical control (the NYHA class I), mitral valve repair, tricuspid valve repair, and left atrial MAZE procedure were performed via right mini-thoracotomy. Cardiopulmonary bypass (CPB) was established with cannulation to the right femoral artery, the right jugular and the left femoral vein because of difficulty to deliver the venous cannula into the right atrium through the right femoral vein. The right lung was decompressed with differential lung ventilation (DLV) by a double-lumen tracheal tube. Mitral valve repair was completed with plication of prolapsed part of the posterior leaflet and annuloplasty using a 28-mm CG future ring (Medtronic, Minneapolis, MN, USA). Tricuspid annuloplasty with a 30-mm Edwards MC3 tricuspid rigid ring (Edwards Lifesciences, Irvine, CA, USA) and left atrial maze procedure with Isolator Synergy Clamps (AtriCure, Inc., Ohio, USA) were added. Due to complicated surgical manipulation through the mini-thoracotomy, cross-clamp time was 236 min, and especially CPB time was very long (359 min) because of the struggling regarding setting up, hemostasis, and so on. Thirty minutes after the surgery, oxygen saturation suddenly dropped to approximately 80 %, and frothy pink sputum was blast out from the endotracheal tube. Chest radiograph showed unilateral right-sided massive infiltrate. No evidence of right pulmonary vein occlusion and residual mitral insufficiency was detected by trans-esophageal echocardiography. DLV was started for the affected right lung with high PEEP and low FiO2 (20 mmHg, 60 %, respiratory rate 5/min) by bilevel airway pressure mode (Puritan Bennett 840, Covidien), and for the unaffected left lung with low PEEP and high oxygen (10 mmHg, 100 %, respiratory rate 18/min) by assist/control mode (Evita XL, Dragel) to maintain total oxygenation. Despite the overnight DLV, PaO2/FiO2 ratio dropped under 60 and hemodynamics was collapsed on the next day. A V-V ECMO was initiated by two cannulas: venous drainage cannula (PCKC-V-24, Toyobo, Osaka, Japan) through the right jugular vein and return cannula (PCKC-A-18, Toyobo) through the left femoral vein. Following the induction of V-V ECMO, PaO2/FiO2 ratio went up 300 under 10 mmHg PEEP (both ventilators). The ventilation machines were synchronized with respiratory rate of 5/min during V-V ECMO support. DLV was converted to single ventilation on the third postoperative day. Urine output was maintained at least 30 ml/h through the perioperative period, and a mechanical renal support was not needed. Peaked serum creatinine was 2.80 mg/dl. Cardiac output was maintained with catecholamine, which was gradually attenuated within 3 days. Sivelestat was administered daily. Pulse steroid therapy with methylprednisolone was applied for 3 days. On the postoperative day 3, chest radiography showed reduced right-sided infiltration (Fig. 1), weaning of V-V ECMO began. V-V ECMO was terminated on the postoperative day 5, and PaO2/FiO2 ratio was 170 under 12 mmHg PEEP. Intensive cares thorough the postoperative course is summarized (Fig. 2). On the postoperative day 52, the patient was ambulatory and was discharged in good general condition.

Postoperative chest radiographies in time. POD postoperative day

Postoperative course and medications use are summarized. DLV differential lung ventilation, PEEP positive end expiratory pressure, ECMO extra corporeal membrane oxygenator, CI cardiac index, PAP pulmonary artery pressure
Discussion
The incidence rate of REPE after drainage of pneumothorax has been reported in several studies. Echevarria et al. reported the incidence of REPE is approximately 1 % [1]. Variation in the frequencies of REPE exists, but the reason is unclear. The mortality rate is reported to be approximately 20 % [2]. Shires et al. reported a case of intractable REPE after aortic valve replacement with right mini-thoracotomy managed with V-V ECMO [3]. In this case, copious sputum was discharged into the DLT bilaterally, and a large single-lumen tube was substituted for more effective suction. In the current case, DLV was applied with two ventilators: first, to maintain total oxygenation by one lung with normal pressure to prevent barotrauma, and second, to protect the unaffected lung from copious frothy sputum. However, early induction of DLV could not prevent cardiopulmonary failure, and a respiratory support by V-V ECMO was necessary. Due to difficulty of delivering the venous cannula through the right femoral vein in the surgery, we used the right internal jugular vein as a drainage vessel, and the left femoral vein as a return vessel. Benefits of the blood drainage from the jugular vein are to stabilize the drainage flow from the right atrium, and to decrease a risk of thrombosis and congestion of the legs and abdominal organs due to large cannula insertion through the femoral vein. Although the outcome of ECMO is usually less favorable in adult patients in hemodynamically crash situations, in REPE, ECMO support in the first several days, in which the inflammatory response is stormy, is helpful to wait until the uproar subsides because REPE usually recovers drastically after approximately 3 days from the onset. Regarding ECMO support, choice of V-V ECMO contributed to favorable result in this case. Compared to the V-A ECMO, V-V ECMO can avoid bleeding and lower limb ischemia. In general, V-V ECMO is indicated when a low oxygen (SaO2 <90 %, under FiO2 100 %), and high bicarbonate (PaCO2 >45 cmH2O, under tidal volume 200 ml/kg/min) respiratory failure continue refractory to the respiratory support. Even in hemodynamically collapsed situation, as far as the reason of the deterioration is purely respiratory function, V-V ECMO can recover the hemodynamics as well. Because the reason of collapse was only respiratory deterioration in our patient, V-V ECMO was chosen. Chronicity of collapse and rapidity of re-expansion are considered contributing factors of REPE [1]. In minimally invasive cardiac surgery, not only lung collapse but also cardiac surgery and extracorporeal circulation is implicated to be important risk factors causing, or aggravating lung injury. Keyl et al. reported that level of mean pulmonary arterial pressure, transfusion of fresh frozen plasma, and diabetes mellitus were related to be the occurrence of REPE [4]. Tutschka et al. reported that risk factors of REPE were chronic obstructive pulmonary disease, pulmonary hypertension, and increasing CPB time [5]. Irisawa et al. reported that ischemic reperfusion injury and systemic inflammatory reaction might be related to REPE [6]. In the presented case, obviously long CPB was an important trigger of REPE. However, long CPB does not always cause severe REPE. In fact, REPE is quite rare (1.7 %) in our institute where 392 patients have received mitral valve repair via mini-thoracotomy within 16 years and 15.3 % of these patients had a CPB time longer than 300 min. We assume that the reason of REPE is multi-factorial from this result. Or complete lung collapse with a double-lumen tracheal tube might be related to REPE because in the first 300 cases a bronchial blocker was used and the right lung was not collapsed completely. This incompleteness might work favorably to prevent REPE.
To prevent the REPE in minimally invasive approach via mini-thoracotomy, the surgical manipulations should be simplified as possible in order to shorten the CPB time. Intermitted bilateral lung inflation during the procedures would be effective to prevent REPE. If the surgery is anticipated to be complicated, avoidance of mini-thoracotomy approach and choice of median sternotomy approach is sensible.
Conclusion
In spite of massive unilateral pulmonary edema and hemodynamically collapse after mitral valve repair via mini-thoracotomy, V-V ECMO support for several days was helpful to wait for the recovery of the lung damage. Although the cause of REPE is multifactorial, effort to shorten the CPB time and intermitted bilateral lung inflation will avoid this deterioration and contribute to establish safe minimally invasive cardiac surgery program.
References
Echevarria C, Twomey D, Dunning J, Chanda B. Does re-expansion pulmonary oedema exist? Interact CardioVasc Thorac Surg. 2008;7(3):485–9.
Mahfood S, Hix WR, Aaron BL, Blaes P, Watson DC. Reexpansion pulmonary edema. Ann Thorac Surg. 1988;45(3):340–5.
Shires AL, Green TM, Owen HL, Hansen TN, Iqbal Z, Markan S, et al. Case 4-2009. Severe reexpansion pulmonary edema after minimally invasive aortic valve replacement: management using extracorporeal membrane oxygenation. J Cardiothorac Vasc Anesth. 2009;23(4):549–54.
Tutschka MP, Bainbridge D, Chu MW, Kiaii B, Jones PM. Unilateral postoperative pulmonary edema after minimally invasive cardiac surgical procedures: a case–control study. Ann Thorac Surg. 2015;99(1):115–22.
Keyl C, Staier K, Pingpoh C, Pache G, Thoma M, Günkel L, et al. Unilateral pulmonary oedema after minimally invasive cardiac surgery via right anterolateral minithoracotomy. Eur J Cardiothorac Surg. 2015;47(6):1097–102.
Irisawa Y, Hiraoka A, Totsugawa T, Chikazawa G, Nakajima K, Tamura K, et al. Re-expansion pulmonary oedema after minimally invasive cardiac surgery with right mini-thoracotomy. Eur J Cardiothorac Surg. 2015 (Epub ahead of print).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
We have no conflict of interest.
Rights and permissions
About this article

Cite this article
Kitahara, H., Okamoto, K., Kudo, M. et al. Successful management of severe unilateral re-expansion pulmonary edema after mitral valve repair with mini-thoracotomy using extracorporeal membrane oxygenation. Gen Thorac Cardiovasc Surg 65, 164–166 (2017). https://doi.org/10.1007/s11748-015-0592-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11748-015-0592-1