
Abstract
Epidemiological data have shown an association of the intake of industrial produced trans fatty acids (TFA) and sudden cardiac death. The present study examines the impact of elaidic acid (t18:1n-9) and linoelaidic acid (t18:2n-6) on the human aortic endothelial cell functional response. Trans fatty acids predominately incorporated into the phospholipid component while only a minute fraction of the total fatty acids (FA) incorporated into triacylglycerol. Trans fatty acids incorporated into the plasma membranes at the expense of the saturated-FA, stearic, palmitic, and to a lesser extent, myristic acid. Both t18:1n-9 and t18:2n-6 induced a pro-inflammatory response by elevating surface expression of intercellular adhesion molecule-1 (ICAM-1). Neither oleic nor linoleic evoked a pro-inflammatory phenotype under the maximal 50 µM treatments. Both TFA and stearic acid increased phosphorylation of the ICAM-1 transcriptional regulator, nuclear factor-κβ (NF-κβ), while oleic and linoleic acids did not appear to alter the phosphorylation status. Elaidic acid minimally affected endothelial cell growth, whereas linoelaidic acid completely inhibited growth at 100 µM and imparted limited cytotoxicity up to 300 µM. Stearic acid induced cytotoxicity at concentrations above 75 µM, while oleic and linoleic acids evoked gradual dose-dependent growth inhibition with cytotoxicity occurring only at linoleic acid concentrations greater than 200 µM. In conclusion, t18:1n-9 and t18:2n-6 fatty acids effectively incorporated into the phospholipid component of endothelial cells and subsequently induce a pro-inflammatory phenotype.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Trans fatty acid sources are either industrially produced (IP-TFA) or ruminant produced (RP-TFA). Industrially produced-trans fatty acids are generated by the partial hydrogenation of vegetable fats and, to lesser extent, fish oils using a high heat source, hydrogen gas, and a metal catalyst. Industrially produced-trans fatty acids account for a majority of the trans fats in the western diet, and the IP-TFA content of partially hydrogenated fat could reach as high as 60 % [1]. Naturally occurring RP-TFA arise from the bio-hydrogenation in ruminant animals, which are present in beef and sheep products, such as milk and cheese. The RP-TFA present in meat and dairy products comprise a maximum of 6 % of the fat content [1]. In European countries, such as Denmark, aggressive measures have drastically reduced IP-TFA in food products; as a result, their major source of TFA is ruminant produced. The RP-TFA intake in the general Danish population consists of 85 % dairy products and the remaining 15 % in ruminant meat products [2]. Conversely, TFA consumption in the USA population is estimated to account for 4–12 % of the total dietary fat intake, which equates to 13 g of TFA/person/day based on the highest daily intake of TFA [3]. Despite recent trends to drastically reduce trans fatty acids from dietary intake in European countries, IP-TFA are readily present in the western diet, particularly in the USA. Trans fatty acid intake in Canada was as high as 8.4 g/person/day in the mid-1990s; however, following the health Canada’s 2007 request to voluntarily reduce the quantity of IP-TFA by food manufacturers, the average daily intake dropped to 3.4 g/person/day (1.4 % food energy) in 2008 [4]. Even with the significant reduction, the TFA intake continues to exceed the World Health Organizations recommendations of <1 % of food energy consumption.
Epidemiological evidence has established a correlation of TFA consumption with the risk of death from coronary heart disease, primarily due to IP-TFA sources [5–7]. Mozaffarian et al. [8] performed a meta-analysis of four prospective cohort studies investigating the association of TFA intake with the incidence of coronary heart disease (CHD) that resulted in a pooled relative risk of 1.23 (95 % CI, 1.11–1.37; P < 0.0001). Furthermore, these investigators evaluated TFA consumption and the risk of nonfatal myocardial infarction in three retrospective case–control studies, which assessed the TFA content in adipose tissue. With the inclusion of these retrospective studies, the meta-analysis enhanced the association between TFA consumption and the risk of developing CHD (pooled relative risk 1.29; 95 % CI, 1.11–1.49; P < 0.0001). Mozaffarian et al. [8] cautions that although the correlation between TFA intake and the risk of CHD are predominantly due to IP-TFA, RP-TFA consumption could be as detrimental if consumed in significant quantities. In a Danish 18-year follow-up study, there was no indication of an association of RP-TFA intake and the risk of CHD in men. In fact, indications of an inverse correlation were observed in women [9]. Additional studies should be performed in this controversial relationship of RP-TFA consumption and the risk of developing cardiovascular disease.
While most investigations have focused on the impact of IP-TFA, Motard-Bélanger and colleagues [10] reported that both IP- and RP-TFA consumption adversely affects cholesterol homeostasis. Mozaffarian et al. [11] reviewed the effects of TFA consumption on CHD. Trans fatty acid consumption disrupts cholesterol homeostasis, resulting in increased low-density lipoprotein cholesterol with a corresponding decrease in high-density lipoprotein cholesterol levels. Additional evidence outlined in their review emphasizes the pro-inflammatory impact of TFA, including elevated levels of tumor necrosis factor-α, interleukin-6, and C-reactive protein [11]. Bendsen et al. [12] conducted a 16-week intervention study examining the effect of IP-TFA consumption on biomarkers of inflammation in overweight postmenopausal women. Elevated IP-TFA intake increased TNF-α levels as well as soluble forms of the TNF receptors. The investigators conclude that IP-TFA consumption may involve the activation of TNF-α as a possible mechanism leading to the development of cardiovascular disease.
Saturated fatty acids (SFA), stearic acid in particular, are believed to contribute to CHD by invoking lipid-mediated vascular cell dysfunction [13–17]. In a population-based cross-sectional study aimed at determining the effects of SFA and TFA intake on the mean carotid artery intimal medial thickness, elevated consumption of both of these fatty acid classes were independently associated with increased intimal medial thickness [18]. The authors conclude that elevated intake of SFA and TFA may lead to an increased risk of subclinical atherosclerosis. Based on the limited amount of evidence available, previously published data suggest linoelaidic acid is more responsible for CHD than elaidic acid [11, 19]; however, no direct assessment has been performed in primary cells derived from the vasculature. Endothelial cells (EC) are an integral component of the development and progression of CHD, which is hypothesized to possibly be the end result of chronic systemic inflammation. Previous reports published from our laboratory emphasized the significant role of long-chain saturated fatty acids in the generation of a pro-inflammatory endothelial cell phenotype [20, 21]. In the present study, we initiated in vitro studies to directly evaluate the deleterious affects of two commonly consumed TFA, elaidic and linoelaidic acids, in comparison to their saturated counterpart, stearic acid. As previously reported [22], TFA structurally resemble saturated fatty acids. We hypothesized that TFA-supplemented endothelial cells would develop a pro-inflammatory phenotype similar to cellular responses following long-chain saturated fatty acids, as previously reported [20, 21]. In this investigation, we initiated in vitro studies to compare the direct effects of the TFA, elaidic and linoelaidic acids, as well as stearic acid supplementation on the phenotypic and functional responses in human aortic endothelial cells.
Materials and Methods
Materials
Human-derived aortic endothelial cells as well as the growth medium comprised of EGM-2MV bullet kits (endothelial growth medium-2 microvascular) were purchased from Lonza Walkersville Inc. (Walkersville, MD, USA). Fetal bovine serum was obtained from Invitrogen Corporation (Carlsbad, CA, USA). Consumable tissue culture materials were purchased from Fisher Scientific (Pittsburgh, PA, USA). Western blot antibodies were acquired from Cell Signaling Technology (Danvers, MA). Fluorescently coupled antibodies were obtained from BD Pharmingen (San Diego, CA, USA). All fatty acids were purchased from Nu-Chek Prep Inc. (Elysian, MN, USA). Gas chromatography standards were purchased from Restek Corporation, Bellefonte, PA, USA). Additional chemicals and reagents were obtained from Sigma Chemical Company (St. Louis, MO, USA), unless otherwise noted.
Human Aortic Endothelial Cell Culture
Primary human aortic endothelial cells (HAEC) were maintained in endothelial basal medium-2 (EBM2) supplemented with 5 % fetal bovine serum (FBS) and bullet kit materials as specified by the manufacturer. Cell culture passages of less than ten were experimentally utilized at 80–90 % confluence. Human aortic endothelial cells were maintained at 37 °C in a humidified atmosphere in the presence of 5 % CO2.
Fatty Acid Incorporation into Endothelial Cells
Fatty acid stock solutions (1 mM) were prepared by complexing fatty acid free-bovine serum albumin (BSA) with individual free fatty acids [23]. Sub-confluent endothelial monolayers were cultured for 24 h in the presence or absence of albumin bound-fatty acids (50 µM). Following treatments, cells were trypsinized and washed in phosphate buffered saline (PBS) supplemented with 0.1 % fatty acid free-BSA. Cell pellets were resuspended in calcium and magnesium-free PBS and sonicated to lyse the cells. Internal standards (C23:0, phospholipid and triglyceride) were added to a known volume of cell lysate, whereas protein content was determined with the remaining lysate using a bicinchoninic acid (BCA) protein assay kit (R and D Systems, Elysian, MN).
Lipids were extracted using the Folch method with chloroform: methanol (2:1) [24]. Fractionation of the lipid classes into phospholipids (PL) and triacylglycerols (TAG) was performed using thin layer chromatography using a hexane: diethyl ether: acetic acid (70:30:1; by volume) solvent system. The scraped lipid fractions were subjected to acid-catalyzed esterification by heating for 90 min at 100 °C in a boron trifluoride-methanol solution (14 %). The fatty acid methyl esters were separated by gas chromatography (Shimadzu GC2010; Shimazdu, Columbia, MD, USA) as previously described [25]. Fatty acid peaks were identified by retention times in comparison to authentic standards. Data were analyzed with Shimadzu’s GC solutions software and quantified as the mean quantity of each fatty acid normalized to reflect the protein concentration of each sample.
Lipid Droplet Visualization
Excess triglycerides and cholesterol esters are often packaged and stored intracellularly in the form of lipid droplets. Human aortic endothelial cells were cultured in 4-well Permanox chamber slides in EBM-2 complete medium supplemented with albumin-bound fatty acids for 24 h. The cellular neutral lipids were stained using an oil red O staining kit as described by the manufacturer. These cells were counterstained with modified Mayer’s hematoxylin for visualization using an Olympus BX40 upright microscope at 500× magnification with an oil immersion objective.
Flow Cytometric Analysis of HAEC Adhesion Molecule Expression
Treated HAEC were trypsinized, washed in PBS containing 0.5 % BSA, and resuspended in the same buffer for antibody labeling. Cells were labeled with 0.25 µg phycoerythrin (PE)-conjugated intercellular adhesion molecule-1 (ICAM-1), which is also known as CD54, for 20 min at room temperature in the dark. Subsequently, the cells were washed with PBS containing 0.5 % BSA and resuspended in 300 µL of the wash buffer. In order to ensure binding specificity, an isotype control was established for each data set. Data analysis was performed on a FACSCalibur flow cytometer (Becton–Dickinson, San Jose, CA, USA) equipped with a 15 mW air-cooled argon-ion laser emitting at a 488 nm wavelength. The PE signal was detected through a 585 nm band pass filter and quantified using CellQuest Software (Becton–Dickinson). Results indicate the mean fluorescent intensity of gated endothelial cells, which excluded cellular debris and particles.
Western Blot Analysis
Subconfluent HAEC were grown in six-well tissue culture-treated plates in the presence or absence of albumin-bound fatty acids in EBM-2 complete medium for 24 h under standard tissue culture conditions. Treated cells were rinsed in cold PBS and lysed on ice for 15 min in a 20 mM Tris–HCl (pH 7.4) buffer containing 137 mM NaCl, 100 mM NaF, 2 mM Na3VO4, 10 % glycerol, 1 % Nonidet P-40, 2 mM PMSF, 1 µg/ml leupeptin, 0.15 units/ml aprotinin, and 2.5 mM diisopropyl fluorophosphate. Protein content was determined using a BCA protein assay kit following centrifugation of the detergent solubilized extracts to remove insoluble matter. Proteins were electrophoretically separated in 4–12 % polyacrylamide gradient gels and transferred onto nitrocellulose membranes. Membranes were blocked for 30 min at room temperature in 10 % Roche Western Blocking reagent in Tris-buffered saline supplemented with 0.1 % Triton X-100 (TBST). Blots were probed with primary antibodies according to the manufacturer’s recommendations. Secondary antibodies were peroxidase-conjugated for protein detection using an enhanced chemiluminescence (ECL) system (Amersham Pharmacia Biotechnology, Piscataway, NJ, USA). Nitrocellulose membranes were stripped in 62.5 mM Tris–HCl (pH 6.8) buffer containing 2 % SDS and 100 mM β-mercaptoethanol for 30 min at 50 °C. Stripped blots were washed six times in TBST, blocked, and reprobed with an alternative antibody.
Growth Inhibition and Cytotoxicity Assay
Determination of the influence of fatty acids on cellular growth inhibition and cytotoxicity was evaluated as previously described [20, 21]. Endothelial cells (5,000 cells/well) were plated in a 96-well flat bottom plate and maintained in EBM-2 complete medium for 6 h to permit cell adherence. A subset of established wells were utilized to determine cellular growth (X; baseline at day zero) by administering WST-1 reagent (10 µL/well) and recording optical density readings at 450 nm following a 90-minute incubation under standard tissue culture conditions. All other wells were replaced with EBM-2 complete medium supplemented with varying concentrations of albumin-bound fatty acids. Cell cultures were maintained for an additional 48 h at 37 °C in humidified 5 % CO2. Following the addition of WST-1 and 90-minute incubation, optical density values were used to calculate growth inhibition or cell loss based on the day zero baseline readings. Vehicle controls (EBM-2 complete medium supplemented with fatty acid free bovine serum albumin) determined the total growth potential (Y). Cell growth (Z) was normalized to 100 % using the formula ((Y − X / X) × 100). Effects of fatty acid supplementation were ascertained by comparing to Z values. Values from 100 to zero indicated growth inhibition, whereas values less than zero indicated cell loss. Results are expressed as the means ± standard deviations of at least four determinations.
Apoptosis Detection
Endothelial cells (1.0 × 105) were cultured in six-well plates overnight in EBM-2 complete medium. Spent media was replaced with EBM-2 complete medium supplemented with albumin-bound fatty acids and cultured under typical conditions for 24 h. Following treatments, the cells were rinsed in PBS and trypsinized from the plates. All spent medium, PBS washes, and trypsinized cells were collectively combined to ensure both adherent and non-adherent cells were harvested for analysis. Cell pellets were labeled in a solution containing Annexin V Fluorescein and propidium iodide, which was prepared as described by the manufacturer (Roche Applied Science, Indianapolis, IN). Cell suspensions were labeled in the dark at room temperature for 20 min. Analysis was performed on a FACSCalibur flow cytometer (Becton–Dickinson, San Jose, CA) equipped with a 15 mW air-cooled argon-ion laser emitting at a 488 nm wavelength. Annexin V was detected through a 530 nm band pass filter, while propidium iodide was detected through a 650 nm long pass filter. Data were quantified using CellQuest software (Becton–Dickinson). Data represent the mean ± standard deviation of three determinations.
Statistical Analysis
Data represent the mean ± the standard deviation of at least three determinations. Fatty acid profiles were compared between control and experimental groups using Student t tests. To account for multiple comparisons to a single control group, significance levels were adjusted using the Bonferroni correction, meaning differences were only considered significant when P ≤ 0.025. For the apoptosis/necrosis data, where group variances were similar, analysis of variance (ANOVA) was used for initial comparisons across all groups. If a significant difference was detected across all groups, then Dunnett’s multiple comparison test was used to compare each experimental group to control. Group variances for the ICAM-1 expression data were not assumed to be equal, so multiple Student t tests for unequal variances (Welch’s t test) were used to compare treatment groups to control. To account for the multiple comparisons to a single control group, the Bonferroni correction was used to adjust the significance levels. Here differences were only considered significant if P ≤ 0.017. Significant differences between treatment and control groups are indicated with an asterisk in the tables.
Results
Cellular Incorporation of Trans Fatty Acids
Endothelial cells were supplemented for 24 h with trans fatty acids (50 µM) prior to extraction and fractionation into phospholipids and triacylglycerols. Table 1a summarizes the fatty acid distribution in the EC phospholipids. Both elaidic and linoelaidic cellular levels constitute a minor component of the overall fatty acid profile in vehicle-treated cells; however, both of the TFA were readily incorporated into cellular phospholipids (40–54 % of total FA content). This resulted in a 190-fold (P < 0.025) and 275-fold (P < 0.025) enrichment of t18:1n-9 and t18:2n-6, respectively. Importantly, this incorporation coincides with noteworthy and significant (P < 0.025) decreases in saturated fatty acids (SFA) namely myristic acid (36 % vehicle-treated vs. 17 % TFA-treated), palmitic (32 % vehicle-treated vs. 15 % TFA-treated), +stearic (18 % vehicle-treated vs. 8 % TFA-treated), and monounsaturated fatty acid (MUFA) namely oleic acid (28 % vehicle-treated vs. 10–20 % TFA-treated) levels. The decrease in long-chain polyunsaturated fatty acids (LC-PUFA) was also significant (P < 0.05) but it was to a lesser extent than that of SFA and MUFA (approximately 12–25 %). The treatment of t18:2n-6 reduced n-3 and n-6 PUFA to approximately an equal extent, whereas effect of t18:1n-9 was very minimal on n-6 PUFA reduction than that of n-3 PUFA. Interestingly, the incorporation of TFA did not result in any significant increase in the total fatty acid content in the phospholipid fraction. Table 1b summarizes the fatty acid distribution in the EC triacylglycerols. The fatty acid amounts present in the TAG fraction remained relatively low (2 % of total FA) to that of the phospholipid fraction in vehicle-treated cells. Both TFA were also able to increase incorporation into TAGs by 30–40 % of total fatty acid content. This resulted in an enrichment of t18:1n-9 by 33-fold and t18:2n-6 by 60-fold. There appears to be a small decrease (non-significant) in palmitic acid (12–17 %), but this decrease appears to be compensated by an increase in myristic acid, resulting in no overall change in LC-SFA. It therefore appears that unlike their incorporation into phospholipids, the TFA did not incorporate at the expense of other fatty acids; rather they simply accumulated, causing an increase of total FA in TAGs by 40 or 80 % on t18:1n-9 or t18:2n-6 treatment, respectively. Furthermore, TFA also enhanced some accumulation of LC-PUFA, particularly n-3 PUFA. The overall increase in FA in TAG contributes to an increase of 3–3.5 % of total cellular fatty acids.
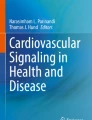
Lipid droplet formation is indicative of an accumulation of TAGs being packaged and stored intracellularly. Figure 1 depicts representative oil red O- and hematoxylin-stained EC supplemented with varying fatty acids (50 µM). Stearic acid-supplemented cells lacked the presence of detectable lipid droplets, which corresponded to the vehicle control cells. As indicated with arrows, lipid droplet accumulation was readily visible in oleic- and linoleic-supplemented EC. The trans fatty acids, elaidic and linoelaidic, did present lipid droplets; however, the abundance of these droplets was substantially less apparent than their cis fatty acid counterparts.

Effect of fatty acid supplementation on the accumulation of neutral lipid storage. Human aortic endothelial cells were supplemented with 50 µM of each individual fatty acid for 24 h at 37 °C in 5 % CO2. As described in the methods, lipid droplets containing triacylglycerols were stained with oil red O, and nuclei were counterstained with hematoxylin for cellular definition (×500 magnification). Treatments included a vehicle, b stearic acid, c oleic acid, d elaidic acid, e linoleic acid and f linoelaidic acid. Lipid droplets are indicated by the arrows. No excess accumulation of lipid droplets was observed when HAEC were co-supplemented with both fatty acids
Effect of Trans Fatty Acid Supplementation on Pro-inflammatory Responses in EC
Adhesion molecule surface expression is indicative of the inflammatory status of EC; therefore, our laboratory quantified intercellular adhesion molecule-1 (ICAM-1; CD54) levels in fatty acid supplemented EC. Cultured EC have basal levels of ICAM-1 surface expression under standard tissue culture conditions. Endothelial cells were supplemented with various fatty acids for 24 h prior to flow cytometric analysis. Table 2 summarizes the results of the relative abundance of ICAM-1 surface expression. Our laboratory previously identified the pro-inflammatory impact of saturated fatty acids, namely stearic acid, on HAEC. Trans fatty acid-supplementation met or exceeded ICAM-1 expression levels in comparison to stearic acid. The highest level of ICAM-1 expression was observed with elaidic acid (50 µM); however, it is important to note that the quantity of ICAM-1 basal expression is only a percentage of the cell’s ability to respond to cytokine stimulation. cis fatty acid supplementation did not significantly elevate basal ICAM-1 expression in comparison to the vehicle.
Although linked to various signaling mechanisms, phosphorylation of NF-κβ has been associated with the pathway leading to ICAM-1 transcription and subsequent deployment to the plasma membrane [20, 21]. Following a 24-hour fatty acid supplementation, EC lysates were electrophoretically separated, transferred, and probed using a phospho-specific (Ser468) antibody for NF-κβ in comparison to GAPDH loading controls. As shown in Fig. 2, EC supplemented with the TFA, elaidic and linoelaidic, demonstrated dose-dependent increases in NF-κβ phosphorylation. With the exception of only a very slight increase in the phospho-NF-κβ levels observed following 50 µM oleic acid supplementation, oleic and linoleic acid-supplementation did not substantially enhance the phosphorylation status of NF-κβ. As previously reported by our laboratory, stearic acid-supplemented HAEC also increased NF-κβ phosphorylation in a dose-dependent manner [20].

Effect of fatty acid supplementation on the phosphorylation of the transcriptional regulator of ICAM-1, NF-κβ. Human aortic endothelial cells were supplemented with varying concentrations of fatty acids for 24 h under typical tissue culture conditions. Endothelial cell lysates (15 µg/sample) were electrophoretically separated in a 4–12 % polyacrylamide gradient gel and subsequently transferred onto nitrocellulose membranes. Using phospho-specific antibodies to detect the activation state of the transcriptional activator, NF-κβ, the relative impact of each fatty acid was ascertained. a Elaidic and linoelaidic, b oleic and linoleic, c and stearic acid-supplemented cells were compared. Glyceraldehyde 3-phosphate dehydrogenase (GAPDH) was used as the protein loading control
Effect of Trans Fatty Acid Supplementation on HAEC Growth Inhibition and Cytotoxicity
In Fig. 3a the effect of TFA supplementation on EC growth is compared to stearic acid. Stearic acid-induced total growth inhibition was observed at 50 µM and significant cytotoxicity occurred at concentrations greater than 75 µM. While linoelaidic acid did invoke a low degree of EC cytotoxicity at the highest concentrations, a steady dose-dependent effect on growth inhibition was observed at concentrations greater than 25 µM. Elaidic acid minimally impacted EC growth and demonstrated no indication of affecting cellular cytotoxicity. Oleic and linoleic acid, the cis counterparts to the TFA, did negatively influence the growth potential of the EC, especially at concentrations greater than 150 µM. Linoleic acid supplementation was more potent than oleic, resulting in cell loss at the highest concentrations.

Effect of fatty acid supplementation on HAEC growth inhibition and cytotoxicity. Human aortic endothelial cells were supplemented with albumin-bound fatty acids at varying concentrations for 48 h at 37 °C in 5 % CO2. Cells were administered WST-1 assay reagent, as described in the methods, to ascertain the metabolic activity. Values less than 100, but above 0, represent growth inhibition, whereas values falling below 0 indicate cell loss in comparison to the day 0 initial population. Calculations of these values are described in the methods. a Elaidic, linoelaidic, and stearic acids are shown, whereas b oleic and linoleic acids portray the cis counterparts to the TFA. Data represent the mean ± the standard deviation of at least four determinations
Effect of Fatty Acid Supplementation on HAEC Apoptosis/Necrosis
To obtain evidence to support the observations in the growth inhibition and cytotoxicity studies, EC were supplemented with fatty acids (either 75 or 100 µM) for 24 h prior to assessing cell viability. Table 3 compares individual fatty acid treatments with a vehicle control in terms of the percentages of cells classified as viable, apoptotic, or necrotic. The TFA, elaidic and linoelaidic acid, slightly affected the overall viability of the cell population, which corresponded with elevated percentages of apoptotic and necrotic cells, particularly at the 100 µM dose. Oleic and linoleic supplementation affected cellular viability to a lesser extent with the exception of an unexplained shift in the population dynamics following linoleic acid (75 µM) supplementation. Stearic acid supplementation clearly demonstrated a significant decrease in cell viability with corresponding increases in apoptotic and necrotic events. This evidence reinforces the findings from the growth inhibition and cytotoxicity studies.
Discussion
Endothelial cells supplemented with either elaidic or linoelaidic fatty acids significantly altered the cellular profile. Interestingly, these fatty acids incorporated into cellular phospholipids, mainly at the expense of myristic, palmitic, and stearic acids, without causing any net gain in total fatty acid levels. Our laboratory previously reported [20] that stearic acid also incorporated into the phospholipid fraction at the expense of palmitic acid without causing any net increase in total fatty acid content in this fraction. However, in the triacylglycerol fraction, incorporation of TFA was minimal (2–4 µg/mg proteins) compared to phospholipids (100–150 µg/mg protein) and did not occur at the expense of any other fatty acid. As shown previously [20], stearic acid incorporation into the TAG fraction was minimal (8 µg/mg protein) compared to its incorporation into phospholipids (70 µg/mg protein). In contrast to saturated and trans fatty acids, oleic acid, a cis fatty acid, incorporated substantially in both phospholipid (80 µg/mg protein) and TAG (20 µg/mg proteins) fractions. This data clearly demonstrates that TFA not only structurally resemble saturated fatty acids but they also incorporate into the cell in a similar fashion to that of saturated fatty acids. The fatty acid incorporation results are consistent with the formation of lipid droplets, which are comprised of TAGs and cholesterol esters. Elaidic and linoelaidic fatty acids did generate a few lipid droplets, whereas vehicle and stearic acid supplemented cells were devoid of oil red O-stained droplets. This data suggests that the polyunsaturated fatty acids, oleic and linoleic, efficiently converted excess fatty acid accumulation into the neutral lipid packages, whereas TFA have a limited capacity for being incorporated into lipid droplets. This further suggests that TFA act more like saturated fatty acids.
Next we compared the functional properties of saturated and cis/trans unsaturated fatty acids. We have previously reported the pro-inflammatory effects of long-chain saturated fatty acids, particularly stearic acid [21]. Within this report, we demonstrated that elevated phosphorylation of NF-κβ (Ser468) corresponded with increased ICAM-1 surface expression in non-challenged endothelial cells. Both elaidic and linoelaidic acids induced phosphorylation of the transcriptional regulator, NF-κβ, consistent with stearic acid. The phosphorylation levels corresponded to increased non-challenged ICAM-1 surface expression. Importantly, the TFA enhanced ICAM-1 expression to levels equal to or surpassing those of stearic acid-supplemented cells. The cis counterparts did not appear to alter the phosphorylation status or the corresponding ICAM-1 surface expression. These results portray a pro-inflammatory endothelial cell phenotype that is consistent with our previous findings, which focused primarily on linoelaidic acid [25, 26]. Sanadgol et al. [27] reported that elaidic acid supplementation did not diminish tumor necrosis factor-α or lipopolysaccharide-induced upregulation of ICAM-1, whereas oleic acid supplementation suppressed the inflammatory response. This evidence suggests that TFA not only invoke a pro-inflammatory response, but they also assist in maintaining the activation status. Furthermore, Rezamond et al. [28] found elevated mRNA expression of pro-inflammatory markers, including interleukin-1β and ICAM-1, in bovine mammary epithelial cells supplemented with elaidic acid. In a cross-sectional study of 730 women from the nurses’ health study I cohort, TFA intake was associated with elevated plasma levels of C-reactive protein, soluble tumor necrosis factor receptor-2, E-selectin, soluble ICAM-1, and soluble VCAM-1 [29]. The authors conclude that elevated TFA intake could lead to a chronic pro-inflammatory endothelial cell phenotype, which could progress into CHD.
Consistent with our previous reports, stearic acid-supplemented endothelial cells invoke cytotoxicity at concentrations surpassing 75 µM [20, 21]. Unlike stearic acid, elaidic and linoelaidic acids do not adhere to the same growth inhibition and cytotoxicity observations. Elaidic acid appears to be well tolerated in terms of endothelial cell growth inhibition, whereas linoelaidic acid did significantly inhibit growth at concentrations >50 µM and limited cell loss was apparent at concentrations exceeding 150 µM. Flow cytometric determination of apoptosis and/or necrosis clearly demonstrated the negative impact of stearic acid supplementation on endothelial cell viability; moreover, premature cell loss in the stearic acid-supplemented EC likely skewed the overall percentages, thereby minimizing the negative impact. Trans fatty acids did slightly impact endothelial apoptosis/necrosis albeit at relatively low percentage alterations. A recent report by Qiu et al. [30] claimed that relatively high concentrations of elaidic acid induced apoptosis in HUVEC cells. This TFA-induced apoptosis involved the activation of caspases 3, 8, and 9. Zapolska-Downar et al. [31] also assessed TFA’s ability to induce apoptosis in HUVEC by comparing both elaidic and linoelaidic fatty acids. They also describe a caspase-3 dependent induction of apoptosis; however, the concentrations used in this study were exceedingly high (up to 5 mM). Consistent with our observations, linoelaidic acid appeared to be potentially more detrimental than elaidic acid.
In conclusion, both elaidic and linoelaidic fatty acids incorporate into endothelial cell phospholipids, and TFA are capable of being incorporated into triacylglycerols to a limited extent. Elaidic acid-supplemented endothelial cells portrayed the most pro-inflammatory phenotype. Furthermore, in contrast to stearic acid (as shown previously) [20], elaidic acid did not negatively impact human aortic endothelial cell growth; however, cellular incorporation of TFA from industrially produced dietary sources into the vasculature could lead to a sustained inflammatory state as elaidic acid is significantly more abundant than linoelaidic in the IP-TFA. The concentration of trans fatty acids (5–50 µM) used in the present study were within the physiological range found in fasting 20-years-old non-Hispanic white individuals (30–103 µM) [32]. The pro-inflammatory effects observed in this in vitro study, therefore, suggest an association of dietary TFA with CHD.
Abbreviations
- ANOVA:
-
Analysis of variance
- BCA:
-
Bicinchoninic acid
- BSA:
-
Bovine serum albumin
- CHD:
-
Coronary heart disease
- CO2 :
-
Carbon dioxide
- EBM2:
-
Endothelial basal medium
- EC:
-
Endothelial cell(s)
- FA:
-
Fatty acid(s)
- FBS:
-
Fetal bovine serum
- GAPDH:
-
Glyceraldehyde 3-phosphate dehydrogenase
- HAEC:
-
Human aortic endothelial cell(s)
- HUVEC:
-
Human umbilical vein endothelial cell
- ICAM-1:
-
Intercellular adhesion molecule-1
- IP-TFA:
-
Industrially produced-trans fatty acid(s)
- NF-κβ:
-
Nuclear factor-κβ
- PE:
-
Phycoerythrin
- PL:
-
Phospholipid(s)
- RP-TFA:
-
Ruminant produced-trans fatty acid(s)
- SFA:
-
Saturated fatty acid(s)
- t18:1n-9:
-
Trans ∆9-octadeca-monoenoic acid (elaidic acid)
- t18:2n-6:
-
Trans ∆9,12-octadeca-dienoic acid (linoelaidic acid)
- TAG:
-
Triacylglycerol(s)
- TBST:
-
Tris buffered saline-tween 20
- TFA:
-
Trans fatty acid(s)
- VCAM-1:
-
Vascular cell adhesion molecule-1
References
Stender S, Astrup A, Dyerberg J (2008) Ruminant and industrially produced trans fatty acids: health aspects. Food Nutr Res 52. doi: 10.3402/fnr.v52i0.1651
Jakobsen MU, Bysted A, Andersen NL, Heitmann BL, Hartkopp HB, Leth T, Overvad K, Dyerberg J (2006) Intake of ruminant trans fatty acids in the Danish population aged 1–80 years. Eur J Clin Nutr 60:312–318
Allison DB, Denke MA, Dietschy JM, Emken EA, Kris-Etherton P, Niclolosi RJ (1995) Trans fatty acids and coronary heart disease risk. Report of the expert panel on trans fatty acids and coronary heart disease. Am J Clin Nutr 62:655S–708S
Ratnayake WM, L’Abbe MR, Farnworth S, Dumais L, Gagnon C, Lampi B, Casey V, Mohottalage D, Rondeau I, Underhill L, Vigneault M, Lillycrop W, Meleta M, Wong LY, Ng T, Gao Y, Kwong K, Chalouh S, Pantazopoulos P, Gunaratna H, Rahardja A, Blagden R, Roscoe V, Krakalovich T, Neumann G, Lombaert GA (2009) Trans fatty acids: current contents in Canadian foods and estimated intake levels for the Canadian population. J AOAC Int 92:1258–1276
Willett WC, Stampfer MJ, Manson JE, Colditz GA, Speizer FE, Rosner BA, Sampson LA, Hennekens CH (1993) Intake of trans fatty acids and risk of coronary heart disease among women(see comment). Lancet 341:581–585
Pietinen P, Ascherio A, Korhonen P, Hartman AM, Willett WC, Albanes D, Virtamo J (1997) Intake of fatty acids and risk of coronary heart disease in a cohort of Finnish men. The alpha-tocopherol, beta-carotene cancer prevention study. Am J Epidemiol 145:876–887
Ascherio A (2004) Trans fatty acids and coronary heart disease. Harvard School of Public Health 1–8
Mozaffarian D, Katan MB, Ascherio A, Stampfer MJ, Willett WC (2006) Trans fatty acids and cardiovascular disease. N Engl J Med 354:1601–1613
Jakobsen MU, Overvad K, Dyerberg J, Heitmann BL (2008) Intake of ruminant trans fatty acids and risk of coronary heart disease. Int J Epidemiol 37:173–182
Motard-Belanger A, Charest A, Grenier G, Paquin P, Chouinard Y, Lemieux S, Couture P, Lamarche B (2008) Study of the effect of trans fatty acids from ruminants on blood lipids and other risk factors for cardiovascular disease. Am J Clin Nutr 87:593–599
Mozaffarian D, Aro A, Willett WC (2009) Health effects of trans fatty acids: experimental and observational evidence. Eur J Clin Nutr 63(Suppl 2):S5–S21
Bendsen NT, Stender S, Szecsi PB, Pedersen SB, Basu S, Hellgren LI, Newman JW, Larsen TM, Haugaard SB, Astrup A (2011) Effect of industrially produced trans fat on markers of systemic inflammation: evidence from a randomized trial in women. J Lipid Res 52:1821–1828
Schaffer JE (2003) Lipotoxicity: when tissues overeat. Curr Opin Lipidol 14:281–287
Unger RH (2002) Lipotoxic diseases. Annu Rev Med 53:319–336
Sheehan MT, Jensen MD (2000) Metabolic complications of obesity. Pathophysiologic considerations. Med Clin North Am 84:363–385
Eckel RH, Barouch WW, Ershow AG (2002) Report of the National Heart, Lung, and Blood Institute–National Institute of Diabetes and Digestive and Kidney Diseases working group on the pathophysiology of obesity-associated cardiovascular disease. Circulation 105:2923–2928
Jakobsen MU, O’Reilly EJ, Heitmann BL, Pereira MA, Balter K, Fraser GE, Goldbourt U, Hallmans G, Knekt P, Liu S, Pietinen P, Spiegelman D, Stevens J, Virtamo J, Willett WC, Ascherio A (2009) Major types of dietary fat and risk of coronary heart disease: a pooled analysis of 11 cohort studies. Am J Clin Nutr 89:1425–1432
Merchant AT, Kelemen LE, de Koning L, Lonn E, Vuksan V, Jacobs R, Davis B, Teo KK, Yusuf S, Anand SS (2008) Interrelation of saturated fat, trans fat, alcohol intake, and subclinical atherosclerosis. Am J Clin Nutr 87:168–174
Lemaitre RN, King IB, Mozaffarian D, Sotoodehnia N, Rea TD, Kuller LH, Tracy RP, Siscovick DS (2006) Plasma phospholipid trans fatty acids, fatal ischemic heart disease, and sudden cardiac death in older adults: the cardiovascular health study. Circulation 114:209–215
Harvey KA, Walker CL, Xu Z, Whitley P, Pavlina TM, Hise M, Zaloga GP, Siddiqui RA (2010) Oleic acid inhibits stearic acid-induced inhibition of cell growth and pro-inflammatory responses in human aortic endothelial cells. J Lipid Res 51:3470–3480
Harvey KA, Walker CL, Pavlina TM, Xu Z, Zaloga GP, Siddiqui RA (2010) Long-chain saturated fatty acids induce pro-inflammatory responses and impact endothelial cell growth. Clin Nutr 29:492–500
Roach C, Feller SE, Ward JA, Shaikh SR, Zerouga M, Stillwell W (2004) Comparison of cis and trans fatty acid containing phosphatidylcholines on membrane properties. Biochemistry 43:6344–6351
van Greevenbroek MM, Voorhout WF, Erkelens DW, van Meer G, de Bruin TW (1995) Palmitic acid and linoleic acid metabolism in Caco-2 cells: different triglyceride synthesis and lipoprotein secretion. J Lipid Res 36:13–24
Folch J, Lees M, Stanley GHS (1957) A simple method for the isolation and purification of total lipids from animal tissue. J Biol Chem 226:497–509
Harvey KA, Arnold T, Rasool T, Antalis C, Miller SJ, Siddiqui RA (2008) Trans fatty acids induce pro-inflammatory responses and endothelial cell dysfunction. Br J Nutr 99:723–731
Siddiqui RA, Harvey KA, Ruzmetov N, Miller SJ, Zaloga GP (2009) n-3 fatty acids prevent whereas trans fatty acids induce vascular inflammation and sudden cardiac death. Br J Nutr 102:1811–1819
Sanadgol N, Mostafaie A, Bahrami G, Mansouri K, Ghanbari F, Bidmeshkipour A (2010) Elaidic acid sustains LPS and TNF-alpha induced ICAM-1 and VCAM-I expression on human bone marrow endothelial cells (HBMEC). Clin Biochem 43:968–972
Rezamand P, McGuire MA (2011) Effects of trans fatty acids on markers of inflammation in bovine mammary epithelial cells. J Dairy Sci 94:316–320
Lopez-Garcia E, Schulze MB, Meigs JB, Manson JE, Rifai N, Stampfer MJ, Willett WC, Hu FB (2005) Consumption of trans fatty acids is related to plasma biomarkers of inflammation and endothelial dysfunction. J Nutr 135:562–566
Qiu B, Hu JN, Liu R, Fan YW, Li J, Li Y, Deng ZY (2011) The caspase pathway of elaidic acid (9t-C18:1)—induced apoptosis in human umbilical vein endothelial cells. Cell Biology International (in press)
Zapolska-Downar D, Kosmider A, Naruszewicz M (2005) Trans fatty acids induce apoptosis in human endothelial cells. J Physiol Pharmacol 56:611–625
Vesper HW, Kuiper HC, Mirel LB, Johnson CL, Pirkle JL (2012) Levels of plasma trans fatty acids in non-Hispanic white adults in the United States in 2000 and 2009. JAMA 307:562–563
Acknowledgments
The authors wish to thank Ms. Elaine Bammerlin for the editorial assistance and Mr. Colin Terry for the help in the statistical analysis of the data. The work was supported by a Methodist Research Institute’s summer student internship to Mr. Phillip Whitley.
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Harvey, K.A., Walker, C.L., Xu, Z. et al. Trans Fatty Acids: Induction of a Pro-inflammatory Phenotype in Endothelial Cells. Lipids 47, 647–657 (2012). https://doi.org/10.1007/s11745-012-3681-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11745-012-3681-2