
Abstract
Alterations in plasma apolipoproteins levels can influence the composition, content, and distribution of plasma lipoproteins that affect the risk of atherosclerosis. This study assessed the relationship between plasma apolipoproteins levels, mainly apoAI, and HDL subclass distribution. The contents of plasma HDL subclasses were determined by two-dimensional gel electrophoresis coupled with immunodetection in 545 Chinese subjects. Compared with a low apoAI group, the contents of all HDL subclasses increased significantly both in middle and high apoAI group, and the contents of large-sized HDL2b increased more significantly relative to those of small-sized preβ1-HDL in a high apoAI group. When apoAI and HDL-C levels increased simultaneously, in comparison to a low apoAI along with HDL-C concentration group, a significant increase (116%) was shown in HDL2b but only a slight increase (26%) in preβ1-HDL. In addition, Pearson correlation analysis revealed that apoAI levels were positively and significantly correlated with all HDL subclasses. Multiple liner regression demonstrated that the apoAI concentrations were the most powerful predictor for HDL subclass distribution. With the elevation of apoAI concentrations, the contents of all HDL subclasses increased successively and significantly, especially, an increase in large-sized HDL2b. Further, when apoAI and HDL-C concentrations increased simultaneously, the shift to larger HDL size was more obvious. Which, in turn, indicated that HDL maturation might be enhanced and, the reverse cholesterol transport might be strengthened along with apoAI levels which might be a more powerful factor influencing the distribution of HDL subclasses.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Most prospective epidemiological studies have firmly established that high density lipoprotein (HDL) as assessed by its cholesterol content is inversely correlated with the incidence and prevalence of atherosclerosis [1–3]. In recent years, it has been considered that changes in the distribution of HDL subclasses might be an important marker for susceptibility to the development of coronary heart disease (CHD) [4]. This anti-atherogenic action of HDL is probably related to the reverse cholesterol transport (RCT) by which excess peripheral cholesterol is returned to the liver.
HDL is highly heterogeneous with respect to the hydrated density, size, shape, charge and physiologic functions [5]. Using two-dimensional gel electrophoresis and subsequently the immunoblotting method, HDL can be subdivided into large-sized (HDL2a and HDL2b) and small-sized subclasses (preβ1-HDL, HDL3c, HDL3b, and HDL3a) and preβ2-HDL [6, 7]. The protein components of HDL include apolipoprotein AI (apoAI; 70%), apoAII (20%), and small amounts of apoE and apoCs. As the principal carrier protein of HDL apoAI is believed to mediate the change of HDL size [8]. ApoAI is the activator of lecithin: cholesterol acyltransferase (LCAT) and LCAT may catalyze unesterified cholesterol to cholesterol ester and promote the conversion of preβ1-HDL and HDL3 to HDL2 thus playing a functional role in the maturation process of HDL subclasses [9]. In addition, apoAI is a critical ligand of the HDL receptor scavenger receptor BI (SR-BI) and the interaction of apoAI and SR-BI may facilitate hepatic selective uptake of HDL-C in the RCT pathway [10]. Therefore, apoAI plays a vital role in the maturation and metabolism of HDL as well as the whole RCT process.
Our laboratory investigated the influence of plasmid lipids on the HDL subclass distribution and results suggested that with the increase of plasma triglyceride(TG), total cholesteryl (TC), and low density lipoprotein cholesteryl (LDL-C) levels as well as TG/HDL-C and TC/HDL-C ratios, or the decrease of plasma HDL-C levels, there was a general shift toward smaller-sized HDL [7, 11–14]. This indicated that HDL maturation might be abnormal and RCT might be weakened. In this work, we investigated the characteristic distribution of HDL subclasses along with relationship between apolipoproteins concentrations in particularly apoAI and alteration of HDL subclass distribution in the Chinese population. This might provide additional information about the potential role of HDL subclasses in the risk for CHD.
Subjects and Methods
Subjects
Six-hundred and twelve Chinese adults being either current or retired staff of the university were recruited to participate in a study examining plasma lipid and apolipoprotein concentrations. The study protocol was approved by an ethics committee, and all subjects gave informed consent. Exclusion criteria included the following: (1) presence of nephrosis, diabetes mellitus, hypothyroidism, hepatic impairment; (2) presence of major cardiovascular event (myocardial infarction, severe surgery), stroke; (3) taking lipid-altering medications in the previous 1 month; (4) consuming alcohol, and smoking cigarettes in the previous week before the study. In addition, the women had not undergone administration of hormone replacement therapy or used oral contraceptives and were not pregnant . After applying the exclusions, 545 subjects (347 males mean age 56.4 ± 9.5 years, 198 females mean age 56.9 ± 9.0 years), 395 subjects were from the West China University of Medical Science, Sichuan University and Sichuan Normal University, in Chengdu, Sichuan Province, PR China. 150 subjects were from Nan Hua University, in Hengyang Hunan Province, PR China were included in our present study.
In order to investigate the impact of plasma apoAI levels on the distribution of the HDL subclasses, we divided the subjects into three groups according to apoAI concentrations. Firstly, frequency distribution of apoAI using the Kolmogorov–Smirnov test showed a normal distribution (Fig. 1). Considering that about 68% scores fell in the range of the mean (1248.1) plus or minus 1 SD (204.5), we used 1043.6 mg/L (1248.1—204.5) and 1452.6 mg/L (1248.1 + 204.5) as the two cut-out points. So, the subjects were further subdivided into a low apoAI group (apoAI ≤ 1043.6 mg/L), a middle apoAI group (apoAI 1043.6—1452.6 mg/L) and a high apoAI group(apoAI ≥ 1452.6 mg/L). To investigate further the influence of plasma apoAI and HDL-C levels on the distributions of HDL subclasses, we divided the subjects described above into three groups according to plasma HDL-C levels, that is, high (≥1.55 mmol/L), middle (1.03—1.55 mmol/L), and low (<1.03 mmol/L). The HDL-C levels selected for classification generally conform to Adult Treatment Panel III guidelines [15].

Frequency distribution of apoAI in total subjects
Specimens
Whole blood specimens were drawn, after a 12-h overnight fast, into EDTA-containing tubes. Plasma was separated within 1–2 h. The plasma was then stored at 4 °C and used within 24 h for lipid and apolipoprotein analyses. An aliquot of plasma was stored at −70 °C for the determination of HDL subclasses.
Plasma Lipid and Apolipoprotein Analyses
Plasma TG, TC and HDL-C were measured by standard techniques. TC and TG were determined with enzymatic kits (Beijing Zhongsheng Biotechnological Corporation, Beijing). HDL-C was determined after precipitation of the apolipoprotein (apo)B-containing lipoproteins by phosphotungstate/magnesium chloride [16]. LDL-C was calculated using the Friedwald formula (TG < 4.52 mmol/L) [17]. When plasma TG ≥ 4.52 mmol/L, LDL-C was determined using the precipitation method with polyvinylsulfate (enzymatic kits). Plasma apoAI, B100, CII, CIII and E were determined by radial immunodiffusion methods [18] using kits developed at the Apolipoprotein Research Laboratory, West China Medical Center, Sichuan University. The intra-assay CV for apolipoprotein concentrations was between 2.1 and 4.8%, inter-assay CV was 3.5–7.9%[19].
HDL Subclass Analyses
For each of the enrolled subjects, apoAI-containing HDL subclasses were measured by nondenaturing two-dimensional gel electrophoresis associated with the immunodection method as described previously [7]. Briefly, 10 μl of plasma was first separated by charge on 0.7% agarose gel, into preβ and α mobility particles. After electrophoretic separation of lipoproteins in agarose gels, the developed lipoproteins on agarose gels along with a mixture of standard proteins (bovine serum albumin, ferritin, and thyroglobulin obtain from Pharmacia Uppsala, Sweden) were further separated by electrophoresis in 2–30% nondenaturing polyacrylamide gradient gel in the second dimension. In fact, after 2-D gel electrophoresis, plasma proteins and molecular markers were electrophoretically transferred to PVDF membranes, stained with 0.1% ponceau S, and the position of molecular standard protein bands labeled by pencil, and destained by diffusion, then, using 5% dylipid milk, recovered from the membrane, following interaction with horseradish peroxidase-labeled goat anti-human apo-AI-IgG. The relative concentration of each subclass was calculated as the percentage of plasma apoAI (%) according to the density of each spot. Particle diameters of the HDL subclasses were assessed by comparing the mobility of the sample with the mobility of calibration standard proteins. Then the relative percentage concentration of each HDL subclass was multiplied by apoAI concentrations in sample individuals, respectively. The result was the relative concentration of each HDL subclasses of apoAI(mg/L, apoAI in the subclasses). The inter assay CVs of relative content of preβ1-HDL, preβ2-HDL, HDL3c, HDL3b, HDL3a, HDL2a and HDL2b in plasma sample were 9.4, 9.8, 4.9, 6.2, 7.3, 11.1 and 7.9%, respectively (n = 5).
Statistical Analyses
All statistical analyses were performed using the statistical package SPSS Version 11.0 (SPSS Inc). The Kolmogorov–Smirnov test was applied to test normal distribution. Data were expressed as the mean ± SD. The significant differences between two groups were analyzed by one-way analysis of variance (ANOVA). Multiple liner correlation and regression were calculated to study correlation. Differences were considered significant at P < 0.05.
Results
Concentrations of Plasma Lipids, Apolipoproteins and Contents of HDL Subclasses
Table 1 showed that in the population, the concentration of TG was 2.4 ± 1.7 (mmol/L) which exceeds normal TG levels recommended in the third Report of the National Cholesterol Education Program (NCEP) (ATPIII) guidelines, which indicated a substantial proportion of subjects with hypertriglyceridemia. Meanwhile, concentrations of plasma lipids, lipoproteins along with contents of HDL subclasses were similar change in this population and the subjects with endogenous hypertriglyceridemia [12].
Furthermore, concentrations of TG, and the ratios of TG/HDL-C, TC/HDL-C were significantly lower while those of HDL-C, apoAI, HDL2a and HDL2b were significantly higher in female than in male.
ApoA-I Contents of HDL Subclasses
Figure 2 shows the distributions of HDL subclasses for representative subjects from the group having normolipidemic (A) and from the hyperlipidemic groups. In the hyperlipidemic subjects, spots for the small-sized subclasses(preβ1-HDL, HDL3a, HDL3b, and HDL3c)were larger, whereas large-sized HDL2(HDL2a and HDL2b) had spots that were smaller in comparison with the normolipidemic subjects.

Electrophoretic comparisons of apoA1-containing HDL subclasses. High-density li (B) proprotein subclasses were separated by nondenaturing two-dimensional gel electrophoresis and immunodetection with a goat antihuman apoAI-IgG labeled with horseradish peroxidase. a Normolipidemic. b Hyperlipidemic subjects
Concentrations of Plasma Lipids, Apolipoproteins and Contents of HDL Subclasses According to the Levels of apoAI
As shown in Table 2, with the elevation of apoAI levels, concentrations of HDL-C significantly increased while those of TG decreased significantly. Moreover, all HDL subclasses increased successively and significantly both in males and females. In addition, compared with males in the middle and low apoAI group, the contents of HDL2a and HDL2b were significantly higher for the females in the same apoAI group. In the high apoAI group, the contents of all HDL subclasses had no significant difference between males and females.
Characteristics of HDL Subclass Contents and Frequency Distribution According to apoAI Along with HDL-C
To further investigate the influence of plasma apoAI combined with HDL-C levels on the distributions of HDL subclasses, we designated apoAI ≥ 1452.6 mg/L together with HDL-C ≥ 1.55 mmol/L as the high concentrations group, apoAI 1043.6—1452.6 mg/L together with HDL-C 1.03—1.55 mmol/L as the middle concentrations group, and apoAI ≤ 1043.6 mg/L together with HDL-C < 1.03 mmol/L as the low concentrations group. As shown in Fig. 3, there were 180 (approximately 33%) subjects in the middle concentrations group and they occupied the highest percentage of the population.

Frequency distribution of subjects according to apoAI together with HDL-C levels
Table 3 presented that with elevation of apoAI combined with HDL-C concentrations, all HDL subclasses increased significantly and successively; further compared to the low concentrations group, a significant increased (116%) in large-sized HDL2b but only a slight increase (26%) in small-sized preβ1-HDL were found in high concentrations group.
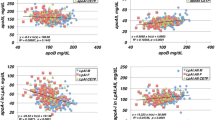
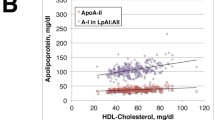
Correlation Coefficients Between Apolipoproteins and Contents of Plasma HDL Subclasses
Correlation analysis revealed that apoAI levels were positively and significantly correlated with all HDL subclasses. Furthermore, apoB100, apoCII, apoCIII and apoE showed positive correlations with preβ1-HDL and HDL3a as well as negative correlations with HDL2a, HDL2b. No significant difference was noted between males and females (Table 4).
Multiple Liner Regression Correlation Between Contents of Plasma HDL Subclasses and Apolipoproteins
Multiple liner regression showed that apoAI was associated independently and positively with all HDL subclasses and it was the most powerful predictor (SRC from 0.321 to 0.605, P < 0.001) for alterations of HDL subclass distributions. In contrast, other apolipoproteins showed positive correlation with preβ1-HDL but negative correlation with HDL2b (Table 5).
Discussion
Numerous clinical and epidemiological studies have demonstrated the inverse and independent association between HDL-C and the risk of CHD [20]. HDL exerts various potentially antiatherogenic properties and until recently, the protective features of HDL had been attributed primarily to its classical function of removing cholesterol form peripheral tissues and transferring it to the liver in a process known as RCT. In vitro experiments as well as genetic family and population studies and the investigation of transgenic animal models have revealed that plasma HDL cholesterol levels do not necessarily reflect the efficacy and antiatherogenicity of RCT [20–23]. Instead, the contents of HDL subclasses are important determinants of RCT and the risk of atherosclerosis [24]. Moreover, the physiologic basis of HDL subclasses has not been elucidated completely. It is necessary to disclose the alterations of distribution of HDL subclasses with the change of plasma apolipoproteins especially apoAI concentrations.
Our results showed that, with the elevation of apoAI levels, all HDL subclasses increased successively and significantly both in males and females. Studies in human apoAI transgenic mice have showed that the distribution of apoAI among the HDL subclasses was similar, suggesting that the content of apoAI in the major HDL subspecies was fixed and that excess apoAI was not present in HDL particles [25]. Kunitake et al. observed that preβ-HDL (discoid shape) generally contain 2 copies, and other studies found that preβ1-HDL contain 1 copy whereas large-sized HDL2 contain four copies of apoAI per particles [26–28]. Hence, apoAI levels might reflect the number of HDL particles, and with the elevation of apoAI levels, molecules of apoAI distributed to each of the subclasses increased which resulted in all HDL subclasses tending to increase. It has been postulated that RCT is indeed the mature and metabolic process that nascent preβ-HDL converted to mature α-HDL. Consequently, the contents of all HDL subclasses increased suggesting that speed of RCT might be enhanced.
Furthermore, the present study showed that the contents of large-sized HDL2b increased more obviously relative to those of the small-sized preβ1-HDL with the elevation of apoAI. In comparison to the same gender subjects in the low apoAI levels, there was an increase in HDL2b (79% in males; 68% in females) and an increase in preβ1-HDL (38% in males; 43% in females) for the subjects with high apoAI levels, which suggests that plasma apoAI levels have significantly important effects on the distributions of HDL subclasses. The variations of HDL subclass distributions are probably related to an increase in HDL-C concentrations and a decrease in TG concentrations for the subjects with high apoAI levels. Several studies have shown that enhanced LCAT, lipoprotein lipase (LPL) activities and impeded hepatic lipase (HTGL) are consistent with lower plasma TG levels [9, 29, 30] The LCAT may catalyze unesterified TC to cholesteryl and promote the conversion of preβ1-HDL and HDL3 to HDL2. LPL plays an important role in hydrolyzing TG transported in chylomicrons and very low density lipoprotein (VLDL) particles. When catabolized by LPL, chylomicrons (CM) and VLDL release TG, TC, PL, apoAI, and apoCs. Subsequent binding of these products to HDL3 results in formation of HDL2 particles. The HTGL activities promote the conversion of HDL2 to HDL3, and furthermore, excess surface phospholipids and apoAI dissociated from HDL2, impaired HTGL activity must lead to the increase of large-sized HDL2 particles and decrease of small-sized preβ1-HDL particles. In addition, it was demonstrated that LCAT activities also increased with high plasma HDL-C levels [29]. Hence, with the increase of apoAI levels, not only the number of HDL particles increased but a lot of large-sized HDL2b was generated which indicated the speed and efficiency of RCT had been enhanced.
We further analyzed the combined impact of plasma apoAI and HDL-C levels on the alterations of HDL subclass distribution. Data obtained in the present study suggested that, with elevation of apoAI along with HDL-C levels, all HDL subclass levels increased gradually and significantly, meanwhile, compared with low the concentrations group (apoAI ≤ 1043.6 together with HDL-C < 1.03), the contents of large-sized HDL2b (116%) increased more significantly than those of small-sized preβ1-HDL (26%) which resulted in an elevation of the HDL2b/ preβ1-HDL ratio (2.0 vs. 3.5) in the high concentrations group (apoAI ≥ 1452.6 together with HDL-C > 1.55). It indicated that alteration of the number of large-sized HDL particles might be more obvious with the increase of apoAI and HDL-C levels.
The correlation analysis also showed that the concentrations of apoAI had a significant positive correlation with all HDL subclasses and multiple liner regression revealed that apoAI might be a more powerful factor influencing the distribution of HDL subclasses. HDL is known to serves as a reservoir for apoCs, apoE. ApoCII is the activator protein for LPL. In contrast, apoCIII could inhibit the LPL activity. Evidently, changes in concentrations of other apolipoproteins (including apoB100, apoCII, apoCIII, apoE) may affect HDL subclass distribution.
In summary, our results reported in this work showed that with the increase of plasma apoAI concentrations, the contents of all the HDL subclasses rose gradually and significantly, especially, an increase in large-sized HDL2b was very striking. Furthermore, when apoAI and HDL-C concentrations increased simultaneously, the trend toward larger HDL size was more obvious. Which, in turn indicated that the maturation of HDL might be enhanced and that RCT might be improved. In addition, Pearson correlation and multiple liner regression analysis revealed that apoAI levels revealed that apoAI levels might be a more powerful factor influencing the distributions of HDL subclasses.
References
Gordon T, Castelli WP, Hiortland MC, Kannel WB, Dawber TR (1977) High density lipoprotein as a protective factor against coronary heart disease: Framingham study. Am J Med 62707–62714
Watkins LO, Neaton JD, Kuller L H. (1986) Racial differences in high density lipoprotein cholesterol and coronary heart disease incidence in the usual care group of the multiple risk factor intervention trial. Am J Cardiol 57538–57545
Gordon DJ, Probstifield JL, Garrison RJ, Bangdiwala S, Tyroler HA (1989) High density lipoprotein cholesterol and cardiovascular disease. Four prospective American studies. Circulation 798–815
Atger V, Giral P, Simon A, Cambillau M, Levenson, Gariepy J, Megnien JL, Moatti N (1995) High-density lipoprotein subfractions as markers of early atherosclerosis. Am J Cardiol 75:127–131
Von Eckardstein A, Huang Y, Assmann G (1994) Physiological role and clinical relevance of high-density lipoprotein subclasses. Curr Opin Lipidol 15404–15416
Wu XW, Fu MD, Lin BW (1999) Study on the immunodetection method of HDL subclasses in human serum. Chin J Arterioscler 7:253–255
Xu Y, Fu MD (2003) Alterations of HDL subclasses in hyperlipidemia. Clinica Chimica Acta 332:95–102
Jonas A, Kezdy KE, Wald JH (1989) Defined apolipoprotein A-I conformations in reconstituted high density lipoprotein discs. J Biol Chem 264:4818–4824
Rye KA Clay MA, Barter PJ (1999) Remodelling of high density lipoproteins by plasma factors. Atherosclerosis 145:227–238
Kwiterovich Jr PO (1998) The antiatherogenic role of high-density lipoprotein cholesterol. Am J Cardiol 82:13Q–21Q
Yuye Yang, Bingyu Yan, Mingde Fu, Yanhua Xu, Ying Tian (2005) Relationship between plasma lipid concentrations and HDL subclasses. Clinica Chimica Acta 354:49–58
Lantu Gou, Mingde Fu, Yanhua Xu, Ying Tian, Bingyu Yan, Luchuan Yang (2005) Alteraions of HDL subclasses in endogenous hypertriglyceridemia. Am Heart J 150:1039–1045
Lianqun Jia, Shiyin Long, Mingde Fu, Bingyu Yan, Ying Tian, Yanhua Xu, Lantu Gou (2006) Relationship between total cholesterol/high-density lipoprotein cholesterol ratio, triglyceride/high-density lipoprotein cholesterol ratio, and high-density lipoprotein subclasses. Metabol Clin Exp (in press)
Li Tian, Lianqun Jia, Mingde Fu, Ying Tian, Yanhua Xu, Haoming Tian, Yuye Yang (2006) Alterations of high density lipoprotein subclasses in obese subjects. Lipids 41:789–796
Executive summary of the third report of NCEP (2001) Expert panel on detection, evaluation and treatment of high blood cholesterol in adults. Adult Treatment Panel III. JAMA 285:486–497
Warnick GR, Nguyen T, Albers AA (1985) Comparison of improved precipitation methods for quantification of high-density lipoprotein cholesterol. Clin Chem 31:217–222
Friedwald WF, Levy RI, Fredrickson DS (1972) Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin Chem 18:499–502
Labeur C, Shepherd J, Rosseneu M (1990) Immunological assays of apolipoproteins in plasma:methods and instrumentation. Clin Chem 36:591–597
Liu B (1995) Immunoassay of human plasma apolipoproteins and clinical applications. In: Wang KQ (ed) Lipoproteins and atherosclerosis. People’s Health Press, Beijing, pp 359–368
Gordon D, Rifking BM (1989) Current concepts:high density lipoproteins-the clinical implications of recent studies. N Engl J Med 321:1311–1315
Hirano K, Yamashita S (1995) Atherosclerotic disease in marked hyperalphalipoproteinemia: combined reduction of cholesteryl ester transfer protein and hepatic triglyceride lipase. Arterioscler Thromb Vasc Biol 15:1849–1856
Berard AM, Foger B (1997) High plasma HDL concentrations associated with enhanced atherosclerosis in transgenic mice overexpressing lecithin-cholesteryl acyltransferase. Nat Med 3:744–749
Hoeg JM, Santamarina-Fojo S (1996) Overexpression of lecithin:cholesterol acyltransferase in transgenic rabbits prevents diet-induced atherosclerosis. Proc Natl Acad Sci USA 93:11448–11453
Arnold Von Eckardstein (2001) High density lipoproteins and Arteriosclerosis. Arterioscler Thromb Vasc Biol 21:13
Edward M, Rubin Y, Ishida, Shirley M, Clift, Ronald M, Kranss (1991) Expression of human apolipoprotein A-I in transgenic mice results in reduced plasma levels of murine apolipoprotein A-I and the appearance of two new high density lipoprotein size subclasses. Biochemistry 88:434–438
Kunitake STm Ka La Sala KJ, Kane JP (1985) ApolipoproteinA-I-containing lipoproteins with pre-beta electrophoretic mobility. J Lipid Res 26:549–555
Asztalos BF, Sloop CH, Wong L (1993) Two-dimensional electrophoresis of plasma lipoproteins:recognition of new apo A-I-containing subpopulations. Biochim Biophys Acta 1169:291–300
Castro GR, Fielding CJ (1988) Early incorporation of cell derived cholesterol into preβ-migrating high-density lipoprotein. Biochemistry 27:25–29
Miida T, Kawano M, Fielding CJ (1992) Regulation of the concentration of preβ high-density lipoprotein in normal plasma by cell membranes and lecithin:cholesterol acyltransferase activity. Biochemistry 31:11112–11117
Miida T, Yamaguchi T, Tsuda T, Okada M (1998) High prebeta1-HDL levels in hypercholesterolemia are maintained by probucol but reduced by a low-cholesterlo diet. Atherosclerosis 138:128–134
Acknowledgments
We thank technician Yu Liu, master students Jia Yao and Xuemei Zhang for the collection of blood sample and technical support in the lipid and apolipoprotein assays.
Author information
Authors and Affiliations
Corresponding author
About this article
Cite this article
Tian, L., Fu, M., Jia, L. et al. Relationship Between Apolipoprotein Concentrations and HDL Subclasses Distribution. Lipids 42, 419–426 (2007). https://doi.org/10.1007/s11745-007-3031-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11745-007-3031-y