
Abstract
The da Vinci Xi robot has been introduced as the successor to the Si platform. The promise of the Xi is to open the door to new surgical procedures. For robotic-assisted radical prostatectomy (RARP)/pelvic surgery, the potential is better vision and longer instruments. How has the Xi impacted on operative and pathological parameters as indicators of surgical performance? This is a comparison of an initial series of 42 RARPs with the Xi system in 2015 with a series using the Si system immediately before Xi uptake in the same calendar year, and an Si series by the same surgeon synchronously as the Xi series using operative time, blood loss, and positive margins as surrogates of surgical performance. Subjectively and objectively, there is a learning curve to Xi uptake in longer operative times but no impact on T2 positive margins which are the most reflective single measure of RARP outcomes. Subjectively, the vision of the Xi is inferior to the Si system, and the integrated diathermy system and automated setup are quirky. All require experience to overcome. There is a learning curve to progress from the Si to Xi da Vinci surgical platforms, but this does not negatively impact the outcome.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The da Vinci robot has evolved, from S to Si and now Xi. The da Vinci Xi now provides 3D-camera developments and the addition of “force feedback,” articulated instruments. So how can we take best advantage of this to improve outcomes while taking into account our learning curve?
Through a better site recognition, 3D-stable view, magnification of the operation field with improved ergonomics, it is possible not only to learn and to teach laparoscopic surgical anatomy in a fascinating direct way, but also to perform advanced laparoscopic operations to a much larger extent in benign and oncological situations [1]. The da Vinci Xi robotic platform helps operating room personnel with smooth movement. In addition, easy patient access is achieved with a side docking facility with the help of the boom feature [2]. Side docking is also possible with the Si system. For the novice surgeon, arm collision can be a significant issue [2]. The patient clearance feature can be used to avoid this. Where access is difficult due to elevated BMI, modifications can be made through reassigning the camera to a different port with utilization of the retargeting feature of the da Vinci Xi [2].
Robotic radical nephroureterectomy is a procedure on the upper and lower tract. Single docking and single robotic port placement have evolved with the development of different generations of the robotic system [2]. These procedures can be performed safely and effectively using the da Vinci S, Si or Xi robotic platform [2]. The new da Vinci Xi robotic platform is intuitive for surgeons using its features and allows a single docking [2]. Due to the length of instruments, the urinary tract can be accessed anywhere along its length. Not only does this new model allow for improved access and approaches, but also has improved dexterity and haptic feedback. We review outcomes transitioning from the Si to Xi and review our learning curve.
Methods
This is a comparison of an initial series of 42 RARPs with the Xi system (2015) with a series using the Si system immediately before Xi uptake in the same calendar year and an Si series by the same surgeon in a single center. This was done synchronously as the Xi series using operative time, blood loss, and positive margins as surrogates of surgical performance.
Results
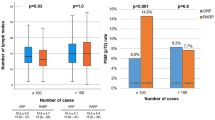
For results, please see Table 1. Subjectively and objectively, there is a learning curve to Xi uptake in longer operative times but no impact on T2 positive margins, which are the most reflective single measure of RARP outcomes. Subjectively, the vision of the Xi is inferior to the Si system, and the integrated diathermy system and automated setup are quirky. All require experience to overcome.
Discussion
The original S model, only had one setup joint, this was replaced by two setup joints in the Si. The boom feature in the Xi allows precision of movement, easier positioning and ergonomically it glides. The ‘plug and play’ feature of no white balance or calibration is also very attractive to a surgical team. It has an 80° field of view, compared with 60° in the Si, and with the Xi, the surgeon can change the angle automatically, with a 30° scope up or down. Both cameras have 1080 pixels. This further contributes to the robots’ versatility. The Xi 8-mm camera allows access down any port. This again allows for a greater versatility in the approach to the patient. However, in contrast to this, questions have arisen regarding optical quality. The Si has a 12-mm camera, compared with an 8-mm one. Can an 8-mm camera provide the same resolution or quality? In addition, the Xi has a chip in the camera tip and has a focal distance, similar to autofocus. In contrast to the Si, the autofocus may be more limited compared with manual focus. With increased versatility and wider angles of vision, this may compromise acuity. This is better than the da Vinci S but not as good as the Si. This has previously been found to be an issue; however, with a subsequent software upgrade, this resolved [2].
The side docking which can also be done with the Si allows for easy access to the pelvis. This makes examining the rectum very easy and thorough which can be very important in radical prostatectomy with wide local excision or any case where extra confidence is needed. Rectal injury is uncommon but when missed is a disaster, so anything that lessens this risk is a great asset. The improved access and versatility of the da Vinci Xi could be applied to the patients undergoing further robotic surgery [3]. The da Vinci Xi allows dissection from the renal hilum to the prostate without the need for redocking or additional port placement [3]. The da Vinci Xi facilitates difficult surgery, robotic RPLND without the need for redocking or additional ports [3].
Sentinel nodes and lymph channels can also be easily identified with da Vinci Xi system [4] as Firefly is automatically built in. With the Si, an upgrade is needed. Sentinel node mapping is an easy and acceptable method with da Vinci Xi in pelvic surgery [4]. This method has previously been conducted using isosulfan blue [4]. Robotic pelvic surgery has distinct advantages over laparoscopy. The latest da Vinci Xi system is enabled with newer features such as longer arms to enable this to be possible.
Conclusion
In conclusion, the Xi does allow the surgeon, a wider range of approach and maneuverability within patient care. There is a degree of compromise with the new optical system. There is a learning curve to progress from the Si to Xi da Vinci surgical platforms, but this does not negatively impact the outcome.
References
Mettler L (2015) Robotic assisted gynecological surgery for hysterectomy. Int J Gynecol Obstet. 131:E1–E2
Patel MN, Aboumohamed A, Hemal A (2015) Does transition from the da Vinci Si to Xi robotic platform impact single-docking technique for robot-assisted laparoscopic nephroureterectomy? BJU Int 116(6):990–994
Haddad A, Porter J (2015) Robotic RPLND using the Da Vinci. J Urol 1:e714
Simsek T, Dogan S, Aydin HA (2015) Sentinel lymph node mapping with Da Vinci Xi in early stage endometrial carcinoma. Int J Gynecol Cancer 1:1051
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
SS Goonewardene and D Cahill do not have any conflicts of interest.
Rights and permissions
About this article

Cite this article
Goonewardene, S.S., Cahill, D. The Da Vinci Xi and robotic radical prostatectomy—an evolution in learning and technique. J Robotic Surg 11, 111–113 (2017). https://doi.org/10.1007/s11701-016-0620-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-016-0620-x