
Abstract
We sought to examine the impact of baseline patient characteristics and perioperative outcomes on postoperative hospital length of stay (LOS), following the robot-assisted radical prostatectomy (RARP). We retrospectively reviewed consecutive patients receiving RARP at our institution by two surgeons between January 2012 and March 2014 (n = 274). Baseline patient characteristics were collected, including Charlson comorbidity index (CCI). Discharge criteria were identical for all patients and included: return of bowel function, pain controlled with oral medications, and ambulation without assistance. LOS was calculated as the number of midnights spent in the hospital following surgery. Postoperative hospital LOS was equal to 1 day for 225 patients and >1 day for 49 patients. Baseline patient and tumor characteristics, including age, race, body-mass index (BMI), pathologic stage, and Gleason score, were not significantly different. Mean operative time was shorter for patients with LOS > 1 day (155 vs. 173 min, p < 0.01) on univariate analysis. Patients with LOS > 1 day were more likely to have had a complication: 8/49 (17 %) vs. 14/225 (6 %), p < 0.01. However, multivariate logistic regression found baseline CCI > 2 as the only independent predictor of LOS > 1 day (OR = 3.2, p = 0.03), controlling for age, race, BMI, Gleason score, tumor stage, blood loss, operative time, and occurrence of complication. In our experience, baseline patient comorbidity, quantified by CCI, was the only independent predictor of hospital LOS greater than 1 day following RARP. Preoperative assessment of patient comorbidity should be used to better counsel patients on their anticipated postoperative course.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Over the last decade, a robot-assisted radical prostatectomy (RARP) for the treatment of prostate cancer has dramatically increased, with estimates from 8 % of prostatectomies in 2003 to 67 % in 2009 [1]. RARP is associated with improvements in perioperative outcomes and reduction in complications, while maintaining similar oncologic and quality of life outcomes, as compared with an open radical prostatectomy (ORP) [2, 3]. With recent scrutiny and debate regarding the benefits of prostatectomy in the management of prostate cancer [4, 5], improvements in surgical quality and reduction in treatment-associated harms have become increasingly important.
Due to rising pressure to reduce health care costs, hospital length of stay (LOS) has become a financial determinant, as well as a measure of care quality [6, 7]. When indicators of quality of care were examined specifically for the treatment of localized prostate cancer, hospital LOS was found to be a valid and feasible short-term metric for outcome quality [8]. Given the increasing attention on LOS, we sought to examine the relationship of baseline and tumor characteristics and perioperative outcomes on LOS after RARP at our institution.
Materials and methods
Study population
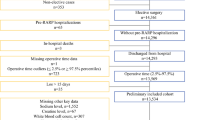
After Institutional Review Board approval, we retrospectively reviewed consecutive patients receiving RARP at our institution. The patients of two surgeons, who performed greater than 24 RARP per year, were included. We identified 274 patients, who received RARP between January 2012 and March 2014. This recent study period was selected as postoperative pathways, and discharge criteria were standardized during this time. Both surgeons had progressed past their learning curves prior to these dates. Baseline patient characteristics were collected and included: age, body mass index, and ethnicity. Charlson comorbidity index (CCI) was ascertained for all patients [9]. No patients were excluded from our analysis.
Our RARP postoperative pathway was standardized using an order set through our electronic medical record system. Acetaminophen and intravenous ketorolac (if renal function was normal) were given as standing orders. Oral and intravenous narcotic pain medications were available as needed, but their use was minimized. Patients began ambulation beginning the evening of the operative day. Diets were advanced from clear liquids to regular on the first postoperative morning.
Outcomes
Pathologic data from prostatectomy specimens and perioperative outcomes were recorded. Complications were classified by the Clavien–Dindo system [10]. The primary outcome measure was hospital LOS, which was calculated as the number of midnights spent in the hospital following surgery. Other outcomes included in analyses were operative time, estimated blood loss (EBL), and readmission within 30 days. Discharge criteria were identical for all patients and included evidence of return of bowel function, pain controlled with oral medications, and ambulation without assistance.
Statistical analysis
All analyses were performed with SAS statistical software version 9.3 and R version 2.15.1. Predictors of LOS were identified with multivariate logistic regression. LOS was considered a categorical variable for multivariate analysis, either less than or equal to 1 day or greater than 1 day. Due to the possible collinear relationship between CCI and complications, a second multivariate analysis was performed with similar covariates, but excluding CCI. Statistical significance was defined by a p value less than 0.05 (two-tailed).
Results
Univariate analyses of patient characteristics, prostatectomy pathology, and perioperative outcomes for patients with LOS equal to one midnight or greater than one midnight are summarized in Table 1. No baseline patient characteristics or prostate pathology data were significantly associated with increased LOS. Mean operative time was longer for those with LOS equal to one midnight (173 vs. 155 min, p < 0.01). Complication rates were higher for those with LOS greater than one midnight: 8/49 (17 %) vs. 14/225 (6 %), p < 0.01. EBL and readmission rates were not significantly different between patients with LOS equal to or greater than one midnight.
Major (Clavien III or greater) complications occurred in two patients, both with LOS greater than one midnight, and included: (1) fascial dehiscence with omental fat noticed at the extraction site requiring return to operating room for exploration and repair (Clavien IIIb) and (2) anterior bladder urine leak requiring percutaneous drain placement (Clavien IIIa).
Multivariate logistic regression analysis of preoperative predictors of LOS greater than one midnight is summarized in Table 2. Only CCI ≥ 2 was found to be an independent predictor of increased LOS (OR = 3.3, p = 0.02). Multivariate logistic regression analysis of both pre- and perioperative predictors of LOS greater than one midnight is summarized in Table 3. CCI ≥ 2 was found to be an independent predictor of increased LOS (OR = 3.2, p = 0.04). Individual components of CCI, such as chronic lung disease or cardiac disease (i.e., myocardial infarct or congestive heart failure), were not found to be significantly associated with LOS on univariate analysis (p = 1.00 and 0.11, respectively). In the first multivariate analysis of pre- and perioperative factors, occurrence of any complication trended toward significance for predicting increased LOS (OR = 2.80, p = 0.07). There was, however, a significant association between CCI ≥ 2 vs. CCI < 2 and the occurrence of a complication (19.2 vs. 7.0 %, p = 0.047). In the second multivariate analysis, which excluded CCI, complications were associated with a longer LOS (OR = 3.00, p = 0.043).
Discussion
Recent large-scale studies have demonstrated improved outcomes with RARP compared with ORP in regard to continence [11], blood loss and transfusion rates [12], potency [13], return to convalescence, complications, and LOS [14, 15]. Positive margin rates appear to be equivalent or improved with RARP [16, 17]. Although many patients are able to be discharged on postoperative day one, others require a lengthier stay [12, 14]. In the present cohort, 225/274 (82 %) of patients were discharged after one midnight. We sought to evaluate the factors that predict longer hospital stays after RARP. CCI ≥ 2 was the sole independent preoperative predictor of LOS > 1 day in our population.
A significant reduction in hospital LOS occurs with minimally invasive (laparoscopic or robot-assisted) over ORP [14, 15]. Hospital, as well as surgeon, volume is inversely proportional to hospital LOS, favoring higher volume and academic centers [18, 19]. In addition, decreasing operative time has been associated with earlier hospital discharge, in both RARP and other surgeries [20–22]. However, studies on the impact of patient-related factors on hospital LOS are limited. Monn et al. examined the United States’ National Surgical Quality Improvement Program (NSQIP) database for partial nephrectomy, radical prostatectomy, and adrenalectomy. Among 12,081 prostatectomies (82 % of which were performed with minimally invasive technique), age, non-white race, COPD, operative time, and the presence of a complication predicted an increased LOS. Congestive heart failure and diabetes were also assessed but not found to be significant. No association with a measure of overall comorbidity [e.g., American Society of Anesthesiologists (ASA) score or CCI] was evaluated [20]. In this study, CCI was used as a measure of preoperative comorbidity. On univariate analysis, a shorter operative time was associated with LOS > 1 day, which contradicts previous literature. This finding did not persist after multivariate analysis. The presence of a complication in those patients staying greater than 1 day [8/49 (17 %) vs. 14/225 (6 %), p < 0.01] is intuitive, and although not statistically significant in the initial multivariate analysis, and was significant in the second analysis, which excluded CCI. This is likely the result of the relationship between CCI ≥ 2 and the development of a complication (p = 0.047). When controlling for age, race, BMI, Gleason score, tumor stage, EBL, operative time, and occurrence of a complication, only CCI ≥ 2 was predictive of LOS > 1 day (OR = 3.2, p = 0.04). To the best of our knowledge, this is the first time that this relationship has been demonstrated in prostatectomy patients.
Pressure to reduce healthcare costs is growing. Bolenz et al. evaluated the costs of RARP and ORP, and found an estimated direct cost of $6752 for RARP vs. $4437 for ORP. The higher cost of RARP was attributed to surgical supply and operating room costs. Although the authors found a significantly shorter LOS for RARP, the cost of ~$500 per night did not mitigate the overall expenditure [23]. Kim et al. from the Mayo Clinic assessed a population-based cohort and demonstrated higher total hospitalization costs for RARP compared with ORP ($11,932 vs. $9390). Yet, within a single healthcare system, cost equivalence can be achieved between RARP and ORP if the operation is done in high enough volume (≥10 cases per week) [24]. Bolenz et al. also evaluated predictors of cost after RARP. Intuitively, LOS predicted higher costs. The authors assessed comorbidity status by ASA score, and not by CCI. They found no association with ASA and costs [25].
LOS has been a point of emphasis in the United States and elsewhere since the institution of the Medicare prospective payment system in 1983. Within this system, health care policies financially incentivize earlier hospital discharge based on payments for admissions, which are founded on a patient diagnosis-related group [26]. Poignant concern regarding the shortening of LOS and the possible effect on increasing readmissions has been articulated, although it does not seem to be true for prostatectomy. Jacobs et al. report that during a 14-year period, post-prostatectomy LOS was reduced by 55 %, while readmission rates remained similar: 4.9 % (95 % CI 4.3–5.4 %) in 1992–1993 and 4.6 % (95 % CI 3.9–5.3 %) in 2004–2005 [27]. Comparable rates of readmission were found in this study: 8/225 (4 %) for patients with LOS = 1 and 3/49 (6 %) for those with LOS > 1 (p = 0.42).
Quality improvement programs have been increasingly integrated into medical practice at all levels. They aim to improve patient safety and outcomes, as well as provider accountability and fiscal responsibility. Programs vary from the voluntary NSQIP, which has neither incentivizing nor punitive aspects [20], to the Medicare and Joint Commission quality tracking systems, which attach financial incentives and penalties to performance on certain quality measures. In the context of continued fiscal and sociopolitical pressure to document quality, measurable outcomes are speculated to expand beyond those already familiar to the urologic surgeon (e.g., preoperative antibiotic and venous thromboembolism prophylaxis as specified by the Surgical Care Improvement Project) [28] and to potentially include operative time [21]. It is also reasonable to project that LOS may become a tracked measure of quality. Although further expansion of bundled payment systems may reduce the pressure toward earlier discharge, longer LOS continues to carry a financial burden in most systems [23, 25]. The increased risk of hospital-acquired infection associated with longer LOS may also drive inclusion of this measure in quality improvement programs [29]. Within the evolving environment of quality measures and healthcare reform, the popular media has identified prostate cancer and its related outcomes as something of a “litmus test” [30]. Importantly, for hospital LOS to be an accurate measure of surgical quality for RARP, expected LOS should be appropriately adjusted for patient comorbidity.
This study is limited by the retrospective and single-institution experience. Biases inherent to a retrospective study are present, although many potentially confounding variables were controlled by multivariate analysis. The applicability of the findings to all practices may not be possible given that our data come from a tertiary referral center. In addition, the cohort of 274 is relatively small for the modern, high-volume surgeon. The time period assessed (January 2012–March 2014) was narrowed to obtain uniformity in the postoperative pathways, and discharge criteria currently employed. Consequently, generalization of the present analysis should be understood in the context of this sample size. Futuremore, multi-institutional studies will help validate the significance of CCI as a predictor of LOS.
Despite the limitations, this study offers further understanding of the relationship of preoperative patient variables that contribute to tangible outcomes. Elucidation of this relationship can provide for better preoperative counseling. In addition, as the political-economic climate of medicine changes, understanding predictors of outcomes will facilitate better communication of expected risks to patients, payers, and other providers.
Conclusion
In our experience, baseline patient comorbidity, quantified by CCI, was the only independent preoperative predictor of hospital LOS greater than 1 day following RARP. Preoperative assessment of patient comorbidity should be used to better counsel patients on their anticipated postoperative course. Furthermore, for hospital LOS to be an accurate measure of surgical quality for RARP, LOS must be appropriately adjusted for patient comorbidity.
References
Stitzenberg KB, Wong YN, Nielsen ME, Egleston BL, Uzzo RG (2012) Trends in radical prostatectomy: centralization, robotics, and access to urologic cancer care. Cancer 118(1):54–62. doi:10.1002/cncr.26274
Tewari A, Sooriakumaran P, Bloch DA, Seshadri-Kreaden U, Hebert AE, Wiklund P (2012) Positive surgical margin and perioperative complication rates of primary surgical treatments for prostate cancer: a systematic review and meta-analysis comparing retropubic, laparoscopic, and robotic prostatectomy. Eur Urol 62(1):1–15. doi:10.1016/j.eururo.2012.02.029
Alemozaffar M, Sanda M, Yecies D, Mucci LA, Stampfer MJ, Kenfield SA (2014) Benchmarks for operative outcomes of robotic and open radical prostatectomy: results from the health professionals follow-up study. Eur Urol. doi:10.1016/j.eururo.2014.01.039
Wilt TJ, Brawer MK, Jones KM, Barry MJ, Aronson WJ, Fox S, Gingrich JR, Wei JT, Gilhooly P, Grob BM, Nsouli I, Iyer P, Cartagena R, Snider G, Roehrborn C, Sharifi R, Blank W, Pandya P, Andriole GL, Culkin D, Wheeler T, Prostate Cancer Intervention versus Observation Trial Study G (2012) Radical prostatectomy versus observation for localized prostate cancer. N Engl J Med 367(3):203–213. doi:10.1056/NEJMoa1113162
Bill-Axelson A, Holmberg L, Ruutu M, Garmo H, Stark JR, Busch C, Nordling S, Haggman M, Andersson SO, Bratell S, Spangberg A, Palmgren J, Steineck G, Adami HO, Johansson JE, Investigators S- (2011) Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med 364(18):1708–1717. doi:10.1056/NEJMoa1011967
Polverejan E, Gardiner JC, Bradley CJ, Holmes-Rovner M, Rovner D (2003) Estimating mean hospital cost as a function of length of stay and patient characteristics. Health Econ 12(11):935–947. doi:10.1002/hec.774
Thomas JW, Guire KE, Horvat GG (1997) Is patient length of stay related to quality of care? Hosp Health Serv Adm 42(4):489–507
Spencer BA, Steinberg M, Malin J, Adams J, Litwin MS (2003) Quality-of-care indicators for early-stage prostate cancer. J Clin Oncol Off J Am Soc Clin Oncol 21(10):1928–1936. doi:10.1200/JCO.2003.05.157
Charlson M, Szatrowski TP, Peterson J, Gold J (1994) Validation of a combined comorbidity index. J Clin Epidemiol 47(11):1245–1251
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 240(2):205–213
Ficarra V, Novara G, Rosen RC, Artibani W, Carroll PR, Costello A, Menon M, Montorsi F, Patel VR, Stolzenburg JU, Van der Poel H, Wilson TG, Zattoni F, Mottrie A (2012) Systematic review and meta-analysis of studies reporting urinary continence recovery after robot-assisted radical prostatectomy. Eur Urol 62(3):405–417. doi:10.1016/j.eururo.2012.05.045
Novara G, Ficarra V, Rosen RC, Artibani W, Costello A, Eastham JA, Graefen M, Guazzoni G, Shariat SF, Stolzenburg JU, Van Poppel H, Zattoni F, Montorsi F, Mottrie A, Wilson TG (2012) Systematic review and meta-analysis of perioperative outcomes and complications after robot-assisted radical prostatectomy. Eur Urol 62(3):431–452. doi:10.1016/j.eururo.2012.05.044
Ficarra V, Novara G, Ahlering TE, Costello A, Eastham JA, Graefen M, Guazzoni G, Menon M, Mottrie A, Patel VR, Van der Poel H, Rosen RC, Tewari AK, Wilson TG, Zattoni F, Montorsi F (2012) Systematic review and meta-analysis of studies reporting potency rates after robot-assisted radical prostatectomy. Eur Urol 62(3):418–430. doi:10.1016/j.eururo.2012.05.046
Liu JJ, Maxwell BG, Panousis P, Chung BI (2013) Perioperative outcomes for laparoscopic and robotic compared with open prostatectomy using the National Surgical Quality Improvement Program (NSQIP) database. Urology 82(3):579–583. doi:10.1016/j.urology.2013.03.080
Trinh QD, Sammon J, Sun M, Ravi P, Ghani KR, Bianchi M, Jeong W, Shariat SF, Hansen J, Schmitges J, Jeldres C, Rogers CG, Peabody JO, Montorsi F, Menon M, Karakiewicz PI (2012) Perioperative outcomes of robot-assisted radical prostatectomy compared with open radical prostatectomy: results from the nationwide inpatient sample. Eur Urol 61(4):679–685. doi:10.1016/j.eururo.2011.12.027
Novara G, Ficarra V, Mocellin S, Ahlering TE, Carroll PR, Graefen M, Guazzoni G, Menon M, Patel VR, Shariat SF, Tewari AK, Van Poppel H, Zattoni F, Montorsi F, Mottrie A, Rosen RC, Wilson TG (2012) Systematic review and meta-analysis of studies reporting oncologic outcome after robot-assisted radical prostatectomy. Eur Urol 62(3):382–404. doi:10.1016/j.eururo.2012.05.047
Hu JC, Gandaglia G, Karakiewicz PI, Nguyen PL, Trinh QD, Shih YC, Abdollah F, Chamie K, Wright JL, Ganz PA, Sun M (2014) Comparative effectiveness of robot-assisted versus open radical prostatectomy cancer control. Eur Urol 66(4):666–672. doi:10.1016/j.eururo.2014.02.015
Barocas DA, Mitchell R, Chang SS, Cookson MS (2010) Impact of surgeon and hospital volume on outcomes of radical prostatectomy. Urol Oncol 28(3):243–250. doi:10.1016/j.urolonc.2009.03.001
Trinh QD, Schmitges J, Sun M, Shariat SF, Sukumar S, Bianchi M, Tian Z, Jeldres C, Sammon J, Perrotte P, Graefen M, Peabody JO, Menon M, Karakiewicz PI (2011) Radical prostatectomy at academic versus nonacademic institutions: a population based analysis. J Urol 186(5):1849–1854. doi:10.1016/j.juro.2011.06.068
Monn MF, Jain R, Kaimakliotis HZ, Flack CK, Koch MO, Boris RS (2014) Examining the relationship between operative time and hospitalization time in minimally invasive and open urologic procedures. J Endourol/Endourol Soc 28(9):1132–1137. doi:10.1089/end.2014.0259
Huang KH, Kaplan AL, Carter SC, Lipsitz SR, Hu JC (2014) The impact of radical prostatectomy operative time on outcomes and costs. Urology 83(6):1265–1271. doi:10.1016/j.urology.2014.01.047
Procter LD, Davenport DL, Bernard AC, Zwischenberger JB (2010) General surgical operative duration is associated with increased risk-adjusted infectious complication rates and length of hospital stay. J Am Coll Surg 210(1):60–65 e61–62. doi:10.1016/j.jamcollsurg.2009.09.034
Bolenz C, Gupta A, Hotze T, Ho R, Cadeddu JA, Roehrborn CG, Lotan Y (2010) Cost comparison of robotic, laparoscopic, and open radical prostatectomy for prostate cancer. Eur Urol 57(3):453–458. doi:10.1016/j.eururo.2009.11.008
Scales CD Jr, Jones PJ, Eisenstein EL, Preminger GM, Albala DM (2005) Local cost structures and the economics of robot assisted radical prostatectomy. J Urol 174(6):2323–2329. doi:10.1097/01.ju.0000181830.43340.e7
Bolenz C, Gupta A, Roehrborn CG, Lotan Y (2011) Predictors of costs for robotic-assisted laparoscopic radical prostatectomy. Urol Oncol 29(3):325–329. doi:10.1016/j.urolonc.2011.01.016
Epstein AM (2009) Revisiting readmissions–changing the incentives for shared accountability. N Engl J Med 360(14):1457–1459. doi:10.1056/NEJMe0901006
Jacobs BL, Zhang Y, Tan HJ, Ye Z, Skolarus TA, Hollenbeck BK (2013) Hospitalization trends after prostate and bladder surgery: implications of potential payment reforms. J Urol 189(1):59–65. doi:10.1016/j.juro.2012.08.182
Specifications Manual for National Hospital Inpatient Quality Measures (2014). http://www.jointcommission.org/specifications_manual_for_national_hospital_inpatient_quality_measures.aspx. Accessed 3 Feb 2015
Tess BH, Glenister HM, Rodrigues LC, Wagner MB (1993) Incidence of hospital-acquired infection and length of hospital stay. Eur J Clin Microbiol Infect Dis Off Publ Eur Soc Clin Microbiol 12(2):81–86
Leonhardt D (2009) In health reform, a cancer offers and acid test. http://www.nytimes.com/2009/07/08/business/economy/08leonhardt.html?_r=0. Accessed 27 Jan 2015
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
There were no sources of funding for this study.
Conflict of interest
Aaron Potretzke, Eric Kim, Brent Knight, Barrett Anderson, Alyssa Park, Robert Figenshau, and Sam Bhayani declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
Rights and permissions
About this article

Cite this article
Potretzke, A.M., Kim, E.H., Knight, B.A. et al. Patient comorbidity predicts hospital length of stay after robot-assisted prostatectomy. J Robotic Surg 10, 151–156 (2016). https://doi.org/10.1007/s11701-016-0588-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-016-0588-6