
Abstract
To provide perioperative benchmark data for surgeons entering practice from formal robotic training and performing robotic-assisted laparoscopic partial nephrectomy (RAPN). Perioperative outcomes of the first 100 RAPN from a surgeon entering into practice directly from robotic fellowship training were analyzed. Postoperative complications were categorized by Clavien-Dindo grade. Surgical “trifecta scores” and Margin, Ischemia, and Complication (MIC) scoring were utilized to assess surgical outcomes. Statistical analyses were performed using SAS (version 9.2; SAS Institute, Inc., Cary, North Carolina). Median age of the cohort was 63 years (22–81 years), and 34 (34.3 %) patients were over age 65. Forty-one (41.4 %) patients had a BMI > 30. Thirteen (13.1 %) had RENAL 10–12 tumors, 22 of which (22.2 %) were >4 cm in size. Median warm ischemia time was 17 min, and 13 patients had resection without warm ischemia. Five patients were converted to open partial nephrectomy, and 1 patient was converted to laparoscopic nephrectomy. Twenty-one patients (21.2 %) experienced a complication, 6 of whom had a major (Clavien grade 3 or higher) complication with one grade 5 complication. Operating room time decreased with experience, but surgical complications and hospital stay did not change with experience. MIC score of renal cell carcinoma (RCC) patients was 74.7 %, while the surgical trifecta was reached in 71.3 % of RCC patients. Surgeons may enter practice directly from formal robotic training and perform RAPN with perioperative outcomes, surgical complications, surgical trifecta scores, and MIC scoring in line with those the most experienced robotic partial nephrectomists.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Despite the well-established advantages of nephron sparing surgery (NSS), partial nephrectomy (PN) has been traditionally underutilized in the treatment of small renal masses (SRM) [1]. However, the use of PN has steadily increased since 2002 [2]. This may be secondary to diffusion of robotic technology for use in PN. Robotic technology continues to propagate throughout the Urology community with a wider range of urologists incorporating robotic surgery into their practice. As robotic surgery continues to increase in utilization, the training background of these urologists is becoming more varied and diverse. Currently, the benchmark data for robotic-assisted partial nephrectomy (RAPN) is based on large numbers of cases from experienced robotic and laparoscopic surgeons [3–5]. There is currently an absence of benchmark data in the literature for trainees entering practice directly from residency or fellowship training regarding RAPN.
Motivated by this, we completed a prospective evaluation of the first 100 RAPN from a fellowship-trained robotic surgeon entering practice to examine perioperative safety and outcomes. Our primary objective was to provide initial insight regarding fellowship training in RAPN and to provide the first benchmark data for other trainees entering practice either out of fellowship training or residency.
Materials and methods
Following Institutional Review Board approval, we prospectively analyzed the first 100 RAPN performed by one surgeon (DDT) immediately following fellowship training. The surgeries were performed at a tertiary care institution that conducts a residency training program. During fellowship training, the surgeon was directly involved in 58 robotic prostatectomies, over 100 laparoscopic renal surgeries, and 12 RAPN under the supervision of one experienced mentor, performing a portion of each of the operations and assisting during the remaining portions of the operation. This one-year fellowship program was credentialed by the Endourological Society and recognized by the American Urologic Association.
Surgical technique
Patients were placed on an inflatable bean bag in the lateral decubitus position with the ipsilateral arm secured on an arm board above the patient’s head. Pneumoperitoneum was established with the Veress needle technique. All robotic partial nephrectomies were performed with the da Vinci Si surgical system (Intuitive Surgical Corp., Sunnyvale, CA) using a three robotic arm transperitoneal route [2]. An assistant 12 mm port was placed in the supraumbilical midline, and a 5 mm assistant port was placed in the subxhiphoid midline. Dissection was completed with right-hand monopolar scissors and left-hand Maryland bipolar forceps. The third robotic arm utilized Prograsp® forceps for retraction. Renal hilar vessels were isolated, and perirenal fat was removed from the surface of the kidney. In all but 13 cases, the renal artery and vein were clamped with laparoscopic vascular bulldog clamps, and the tumor was excised. Tumor excision was completed athermally with collecting system closure completed when necessary with absorbable suture. Rennoraphy was completed with the sliding-clip technique described previously [6]. A surgical drain was placed and removed when output was low.
Patient analysis
Renal morphometry scoring (RENAL) [7] was completed by one reviewer (DDT). Estimated blood loss and intraoperative blood transfusions were recorded. Operative time was calculated as the time from Veress needle insertion until the last port site was closed. Warm ischemia time was calculated as the time from renal artery clamping until all clamps were removed.
Perioperative outcomes
Postoperative complications were categorized by Clavien-Dindo grade [8]. Prolonged hospital stay was defined as a stay of over 3 days. Prolonged urinary drainage was defined as any patient who went home with a surgical drain in place. “Trifecta” outcomes were defined as negative margins, absence of grade 3 or higher complications, and no change in renal function [9]. Margin, ischemia, and complication (MIC) scoring was utilized and defined as negative surgical margins, ischemia time under 20 min, and absence of complications grade 3 or higher [10].
Statistical analysis
The numeric variables were summarized with the sample median (range) and categorical variables were summarized with number (percentage). The change in preoperative vs. postoperative laboratory measures was assessed by using either Wilcoxon singed rank test or McNemar’s test for paired samples. The Spearman correlation was used to assess an association between total operative time and a RENAL score range. All two-sided P values ≤0.05 were considered statistically significant. Statistical analyses were performed using SAS (version 9.2; SAS Institute, Inc., Cary, North Carolina) and R Statistical Software (version 2.11.0; R Foundation for Statistical Computing, Vienna, Austria).
Results
One patient was eliminated from analysis secondary to incomplete operative and postoperative record. Table 1 represents the preoperative characteristics of the cohort. Table 2 represents the intraoperative and postoperative data collected. All surgical resection margins were negative. Two patients went home with surgical drains in place secondary to urinary leakage, and these drains were removed at 7 days and 13 days, postoperatively and respectively. The one patient with 5,000 mL of estimated blood loss had a renal vein injury intraoperatively, which was repaired, and partial nephrectomy was completed robotically. One patient was converted to radical nephrectomy and had a RENAL 10 h lesion that was incompletely resected and converted to laparoscopic nephrectomy. Twenty-one (21.2 %) patients suffered a postoperative complication (Clavien grade 1–5). Six (6.06 %) patients suffered a major complication (Clavien grade 3–5). Of the five grade 3 and 4 complications, three patients required interventional radiology coiling of a pseudoaneurysm. One patient had an active myocardial infarction during surgery, and one patient required surgical intervention to remove a migrated surgical drain. There was one Clavien grade 5 complication in which the patient suffered a fatal myocardial infarction 2 weeks following surgery. Two patients developed port-site hernias requiring repair numerous months following surgery. MIC scoring was not statistically associated with age, BMI, or RENAL score (all, P > 0.25). Trifecta scoring was not related to any of the noted variables except age >65 (P = 0.007).
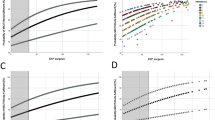
Table 3 is the distribution of total operating time, postoperative complications, and intraoperative conversion according to different RENAL scoring range (RENAL scores 4–6 vs. 4–9 vs. 10–12). Spearman correlation to assess the association of total operative time with different ranges of RENAL score, assuming that RENAL scores are ordinal measures, found a significant association of RENAL score and operative time (Spearman correlation = 0.34, P = 0.001) for RENAL scores ranging 4–9 and a marginally significant association (Spearman correlation = 0.32, P = 0.051) for RENAL score range of 4–6. If RENAL scores 10–12 (n = 13) are compared to the rest of the cohort with regard to operating room time and complications, there is no difference in major or minor complications between the 2 groups, but operative time was significantly longer in the RENAL 10–12 patients (232 min vs. 200 min, P = 0.021). There were no major complications in the RENAL 10–12 patients.
When tumor size over 4 cm (n = 22) is analyzed, there does not appear to be a relationship with complications or conversions to open surgery (P = 1.00). However, resection of tumors over 4 cm is associated with increased operating room time (229 vs. 177 min, P = 0.016). When patients were grouped into BMI categories of <25 (n = 21), 25–30 (n = 37), and >30 (n = 41), there was no association with increased operating room time, hospital stay, or complications (any or major complications). Similarly, when patients over the age of 65 were compared to those under the age of 65, there was no association with operating room time, hospital stay, or complications (any or major).
Table 4 compares patients who had warm ischemia time secondary to hilar clamping for tumor resection (n = 86) versus those that had no warm ischemia time (n = 13). The only statistically significant difference was serum creatinine level on postoperative day one (P = 0.006).
Table 5 analyses patients broken into quintiles by surgery date to assess the effect of operative experience on operative time and complications. Operating room time decreases with experience but the incidence of overall complications and major complications does not appear to be related to operative experience. However, it can be noted that the highest complication rate (any or major) was in the 2nd quintile of patients.
Discussion
Currently, the benchmark data for RAPN is from large volume robotic surgery centers or early adopters of the technology [3–5]. The number of cases required to overcome the “learning curve” and reach “expert” status for RAPN remains unclear. Unlike robotic prostatectomy, there is no consensus definition of the “learning curve” with RAPN. There is a paucity of benchmark data for surgeons entering practice directly from residency or fellowship training. Mottrie et al. [11] noted that it takes 3040 RAPN cases to master the procedure in the hands of an experienced robotic prostatectomist. They defined the “learning curve” as the ability to complete tumor resection with warm ischemia time (WIT) under 20 min accompanied by robotic console time approaching the 90 min range. Haseebuddin et al. [12] noted the RAPN learning curve for an experienced laparoscopic renal surgeon to be about 16 cases. A multicenter analysis of RAPN performed in France noted that complications seemed to decrease after 20 RAPN, thereby setting the “learning curve” at roughly 20 cases [13].
The data presented in this manuscript does not necessarily clarify a “learning curve” however, when the surgical experience is broken into blocks of 20 cases, there was an association with decreased operating room time with experience. We did not note an improvement in complications with surgical experience. However, it can be noted that our highest incidence of complications (any and major) occurred in the 2nd quintile grouping.
The overall complication rate in this series was 21.2 % with 6 major complications. A recent French study examining 240 RAPN over a 3-year period reported a 30 % risk of postoperative complications associated with the procedure [13]. They noted that limited surgeon experience, blood loss, and opening of the collecting system were the three main predictors of postoperative complications. RENAL scoring was not associated with postoperative complications in their experience. Similar to the above experience, increasing RENAL score was associated with higher OR times but not surgical complications in our sample. Our analysis demonstrated no relation between complications and larger tumor size, increasing BMI, or age over 65 years. Bleeding complications in the French study were more common in patients who were on anticoagulants [13]. Bleeding is the most common postoperative complication following RAPN with blood transfusion required in approximately 4 % of cases [14]. Increased RENAL score, longer operative time, and operative blood loss >250 ml are all associated with an increased risk of postoperative hemorrhagic complications [15]. There was one death noted in our initial 100 patients as the result of a postoperative myocardial infarction 14 days following surgery. Kim et al. [14] reviewed the largest RAPN series and noted that cardiovascular events including arrhythmias and myocardial infarctions are rare following RAPN between 0.1 and 0.5 % of patients. This low rate of cardiovascular complications likely reflects alternative options for SRMs elected in patients with elevated cardiovascular risk including watchful waiting and percutaneous ablation.
Most investigators agree that maximal preservation of renal function is achieved with WIT under 30 min and preferably limited to under 20 min [16]. WIT is noted to be under 30 min in most large RAPN series [11]. The WIT in our experience was 17 min in the 86 patients who had resection with renal hilar clamping. Unclamped partial nephrectomies were completed in 13 selected patients. Unclamped partial nephrectomies in those selected patients were associated with an improved postoperative day number 1 creatinine compared to the 86 patients in the WIT group. Unclamped partial nephrectomy was not associated with an increased rate of complications or increased hospital stay.
The surgical “trifecta” of RAPN has been proposed to be negative surgical margins, no complications, and no renal function change [9]. The trifecta rate of our RCC cases was 71.3 %, which is well in line with those of the most experienced laparoscopic/robotic partial nephrectomist in the world [9]. One problem with the surgical “trifecta” as it is originally proposed is that their lack of standardization of when to define a patient as having no change in GFR. The authors also define complications that are “urologic related.” Trifecta scoring in our sample was not related to any surgical variable except age >65. In contrast to “trifecta” scoring, the surgical MIC score is proposed to standardize terminology of RAPN and is defined as negative surgical margins, WIT <20 min, and no major complications (grade 3 or higher) [10]. The original description of the MIC score was accompanied by the author’s score of 75.8 % in his last 99 RAPN [10]. The MIC score of our RCC cases was 74.7 %. Since all of our surgical resection margins were negative, complications and ischemia time over 20 min were the limiting factors in the MIC analysis. MIC scoring was not statistically associated with age, BMI, or RENAL score in our sample.
A recent study utilizing the nationwide inpatient sample noted that robotic utilization was increasing for partial nephrectomy and that RAPN was associated with higher hospital charges but less complications and less prolonged hospitalizations than open or laparoscopic partial nephrectomy [17]. Ellison et al. [18] compared outcomes of multiple surgeons performing RAPN compared to LPN performed by an experienced surgeon and noted that after a rapid learning curve, the RAPN outcomes were similar to those of the single experienced laparoscopic surgeon. It is possible that robotic technology may be making minimally invasive partial nephrectomy more feasible for a greater number of surgeons and thereby playing a role in the increased utilization of minimally invasive partial nephrectomy seen currently. It can be argued that robotic technology played a role in this series, allowing a novice surgeon to complete 13 RENAL 10–12 tumors in a minimally invasive fashion. There is currently no literature documenting a case volume of complex RENAL 10–12 performed by a novice surgeon that rivals the number seen in this series that has not been performed robotically.
One could argue that the benchmark data of a single surgeon provided in this manuscript is not secondary to fellowship training. As with most manuscripts pertaining to surgical experience, it is difficult to delineate out training from technology and inherent surgical skill level. It is also possible that the small number of patients did not allow for analysis of certain differences that may have been statistically present. One strength of this analysis is its strict definitions of hospital stay, age, BMI, “trifecta,” and MIC scoring. This allowed for a conservative measure of perioperative outcomes.
Conclusions
Surgeons may enter practice directly from training and perform RAPN with perioperative safety, surgical complications, surgical trifecta scores, and MIC scoring in line with early adopters and most experienced robotic partial nephrectomists. This experience may serve as benchmark data for surgeons entering practice directly from fellowship or residency training.
References
Hollenbeck BK, Taub DA, Miller DC, Dunn RL, Wei JT (2006) National utilization trends of partial nephrectomy for renal cell carcinoma: a case of underutilization? Urology 67:254–259. doi:10.1016/j.urology.2005.08.050
Poon SA, Silberstein JL, Chen LY, Ehdaie B, Kim PH, Russo P (2013) Trends in partial and radical nephrectomy: an analysis of case logs from certifying urologists. J Urol 190:464–469. doi:10.1016/j.juro.2013.02.094
Tanagho YS, Kaouk JH, Allaf ME, Rogers CG, Stifelman MD, Kaczmarek BF, Hillyer SP, Mullins JK, Chiu Y, Bhayani SB (2013) Perioperative complications of robot-assisted partial nephrectomy: analysis of 886 patients at 5 United States centers. Urology 81:573–580. doi:10.1016/j.urology.2012.10.067
Spana G, Haber GP, Dulabon LM, Petros F, Rogers CG, Bhayani SB, Stifelman MD, Kaouk JH (2011) Complications after robotic partial nephrectomy at centers of excellence: multi-institutional analysis of 450 cases. J Urology 186:417–422. doi:10.1016/j.juro.2011.03.127
Ficarra V, Bhayani S, Porter J, Buffi N, Lee R, Cestari A, Mottrie A (2012) Predictors of warm ishcemia time and peri-operative complications in a multicenter, international series of robot-assisted partial nephrectomy. Euro Urol 61:395–402. doi:10.1016/j.eururo.2011.10.046
Bhayani SB, Figenshau RS (2008) The Washington University Rennorrhaphy for robotic parital nephrectomy: a detailed description of the technique displayed at the 2008 World Robotic Urologic Symposium. J Robot Surg 2:139–140
Simmons MN (2011) Morphometric characterization of kidney tumors. Curr Opin Urol 21:99–103. doi:10.1097/MOU.0b013e32834208d6
Dindo D, Demartines N, Clavien PA (2004) Classification of surgical complications. Ann Surg 240:205–213
Hung HJ, Cai J, Simmons MN, Gill IS (2013) “Trifecta” in partial nephrectomy. J Urol 189:36–42. doi:10.1016/j.juro.2012.09.042
Buffi N, Lista G, Larcher A, Lughessani G, Ficarra V, Cestari A, Lazzeri M, Guazzoni G (2012) Margin, ischemia, and complications (MIC) score in partial nephrectomy: a new system for evaluating achievement of optimal outcomes in nephron-sparing surgery. Euro Urol 62:617–619. doi:10.1016/j.eururo.2012.06.001
Mottire A, Naeyer GD, Schatteman P, Carpentier P, Sangalli M, Ficarra V (2010) Impact of the learning curve on perioperative outcomes in patients who underwent robotic partial nephrectomy fo parenchymal renal tumours. Euro Urol 58:127–133. doi:10.1016/j.eururo.2010.03.045
Haseebuddin M, Benway BM, Cabello JM, Bhayani SB (2010) Robot-assisted partial nephrectomy: evaluation of learning curve for an experienced renal surgeon. J Endourol 24(1):57–61. doi:10.1089/end.2008.0601
Mathieu R, Werhoest G, Droupy S, de la Taille A, Bruyere F, Doumerc N, Rischmann P, Vaessen C, Roupret M, Bensalah K (2013) Predictive facors of complications after robot-assisted laparoscopic partial nephrectomy: a retrospective multicentre study. BJU Int 112:283–289. doi:10.1111/bju.12222
Kim EH, Larson JA, Fienshau M, Figenshau RS (2014) Perioperative complications of robot-assisted partial nephrectomy. Curr Urol Rep 15:377. doi:10.1007/s11934-013-0377-y
Fardoun T, Chaste D, Oger E, Mathieu R, Peyronnet B, Rioux-Leclercq N, Verhoest G, Patard JJ, Bensalah K (2014) Predictive factors of hemorrhagic complications after partial nephrectomy. Eur J Surg Oncol 40:85–89. doi:10.1016/j.ejso.2013.11.006
Becker F, Van Poppel H, Hakenberg OW, Steif C, Gill I, Guazzoni G, Montorsi F, Russo P, Stockle M (2009) Assessing the impact of ischemia time during partial nephrectomy. Eur Urol 56:625. doi:10.1016/j.eururo.2009.07.016
Ghani KR, Sukumar S, Sammon JD, Rogers CG, Trinh QD, Menon M (2014) Practice patterns and outcomes of open and minimally invasive partial nephrectomy since the introduction of robotic partial nephrectomy: results from the nationwide inpatient sample. J Urol 191(4):907–913. doi:10.1016/j.juro.2013.10.099
Ellison JS, Montogmery JS, Wolf JS, Hafez KS, Miller DC, Weizer AZ (2012) A matched comparison of perioperative outcomes of a single laparoscopic surgeon versus a multisurgeon robot-assited cohort for partial nephrecotmy. J Urol 188:45–50. doi:10.1016/j.juro.2012.02.2570
Conflict of interest
AST, BL, and BR have nothing to disclose. DDT is a consultant for Cooper Surgical Corporation.
Ethical standard
This review was approved by the Mayo Clinic Institutional Review Board. All procedures performed were in accordance with the ethical standards of the above review board and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this retrospective review of prospectively collected de-identified data, formal individual patient consent was not required.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Taylor, A.S., Lee, B., Rawal, B. et al. Impact of fellowship training on robotic-assisted laparoscopic partial nephrectomy: benchmarking perioperative safety and outcomes. J Robotic Surg 9, 125–130 (2015). https://doi.org/10.1007/s11701-015-0498-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11701-015-0498-z