
Abstract
Background
We hypothesize that non-alcoholic fatty liver disease (NAFLD) may be significantly associated with waist circumference (WC), neck circumference (NC), hip circumference (HC), and waist-to-hip ratio (WHR).
Objectives
To analyze correlations between anthropometric parameters and the occurrence and intensity of NAFLD aspects assessed by histopathological examination in individuals undergoing bariatric surgery.
Methods
This is a cross-sectional study carried out in a tertiary university hospital. Demographic, clinical, anthropometric, laboratory, and histopathological variables were analyzed; uni- and multivariate analyses were performed. Histopathological variables analyzed were findings of liver biopsies collected during surgical procedures.
Results
Of 119 individuals, 105 (88.2%) were female. The mean age was 38.8 ± 9.3 years and the mean BMI was 37.6 ± 3.1 kg/m2. The prevalence of NAFLD histopathological aspects was: steatosis (76.5%), steatohepatitis (49.6%), and fibrosis (51.3%). WC was significantly higher in individuals with steatosis (103.5 ± 9.9 vs. 99.4 ± 8.4; p = 0.03). Individuals with steatohepatitis presented significantly higher BMI (38.2 ± 3.2 vs. 36.7 ± 2.8; p = 0.01), WC (105.3 ± 10.4 vs. 99.6 ± 8.8; p = 0.002), and WHR (1 ± 0.1 vs. 0.9 ± 0.1; p = 0.02). Age (40.6 ± 9.7 vs. 37 ± 8.5; p = 0.03) and hemoglobin A1c (6.5 ± 0.5 vs. 5.6 ± 0.5; p = 0.004) were significantly higher among individuals with fibrosis. A positive correlation was observed between the steatosis intensity and WHR (R = 0.2; p = 0.04). BMI (R = 0.2; p = 0.02) and glucose (R = 0.2; p = 0.009) were independently correlated with the steatohepatitis intensity. Age (R = 0.3; p = 0.04) was independently correlated with the fibrosis intensity.
Conclusion
There were significant associations between anthropometric parameters and NAFLD aspects. WC and WHR were associated with steatosis; BMI, WC, and WHR were associated with steatohepatitis. WHR independently correlated with steatosis intensity.
Graphical abstract

Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Non-alcoholic fatty liver disease (NAFLD) is an abnormal deposition of fat in the liver without alcohol consumption or other specific causes. It is the most prevalent liver disease worldwide. NAFLD is strongly associated with obesity, hypertension, dyslipidemia, cardiovascular disease, impaired glucose tolerance, and type 2 diabetes (T2D). In addition, other factors, such as genetic and environmental, are also associated with disease progression [1].
Individuals with a BMI within normal clinical standards may have increased levels of visceral adiposity, which is a predictor for developing metabolic syndrome (MetS), characterized by a set of factors that increase cardiometabolic risk [2,3,4,5,6,7,8]. Visceral adipose tissue releases pro-inflammatory and pro-fibrogenic mediators associated with oxidative stress. Body fat compartments have differential effects on metabolic regulation, which may be related either to organ damage or to mitigation of harmful effects. In 1947, Vague firstly described the notion that certain patterns of fat distribution, in particular “central” obesity, predisposed to diabetes, atherosclerosis, gout, and urinary stones and that such fat distribution varied according to gender. Vague coined the terms “android obesity” (predominantly male, fat accumulated mostly in the trunk) and “gynecoid obesity” (predominantly female, whose sites of accumulation in hips and thighs) [9].
Thus, BMI is a useful but incomplete form of assessing nutritional status, since it cannot detect less generalized fat distribution patterns. Anthropometric measures that assess the distribution of body fat seem to better predict cardiovascular risk [10, 11]. Current evidence indicates that waist circumference (WC) more efficiently detects central adiposity and its association with co-morbidities [12,13,14,15]. Neck circumference (NC) is also used as an anthropometric marker of overweight and obesity, in addition to an association with central adiposity [13, 16, 17]. Hip circumference (HC) seems to be associated with better cardiometabolic outcomes because it is linked with the muscle mass of gluteus and quadriceps and favors insulin sensitivity [5, 6, 18]. Waist-to-hip ratio (WHR) is also a measurement that assesses central obesity and its association with co-morbidities. WHR is calculated by the simple division of WC by HC [16, 19].
The hypothesis of this study is that NAFLD in individuals with obesity may be significantly associated with WC, NC, HC, and WHR. This study aims at analyzing the existence of correlations between these anthropometric parameters and the occurrence and intensity of liver steatosis, steatohepatitis, and fibrosis assessed by histopathological examination in individuals with obesity.
Methods
Study Design
This is a cross-sectional study carried out in a tertiary university hospital in 2019. The research protocol was evaluated and approved by the local institutional review board under the opinion: 3.512.406/UNICAMP (CAAE 16562219.0.0000.5404).
Study Population and Sampling Calculation
This study included individuals of any gender, aged 18 to 70 years old, with BMI ≥ 35 kg/m2, which underwent bariatric surgery. Exclusion criteria were previous or current liver disease of other cause, serology abnormalities for viral hepatitis, previous or current use of alcohol, current or recent use of hepatotoxic medications, and previous biliary obstruction.
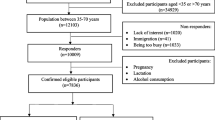
A sample calculation for cross-sectional studies was carried out considering the following parameters: total population of 150 individuals (standardized volume of individuals undergoing bariatric surgery in the current facility each year), 70% proportion of NAFLD patients, precision of 5%, and 95% confidence interval. A minimum sample of 103 participants was estimated.
After applying the inclusion and exclusion criteria, from a total population of 132 individuals, 119 participants were selected. All individuals included in this research underwent open Roux-en-Y gastric bypass surgery. Fig. 1 shows the flowchart of the study population.

Flowchart of the study population
Liver Biopsy
Wedge liver biopsy was performed in all individuals included in the study, through the extraction of a 2-cm fragment from segment III or IV.
Study Variables
Demographic, clinical, anthropometric, laboratory, and histopathological variables were analyzed. The demographic and clinical variables analyzed were: age (expressed in years); gender (male or female), and presence of co-morbidities (hypertension, T2D, and dyslipidemias).
The anthropometric variables analyzed were: BMI (kg/m2); WC (cm); HC (cm); NC (cm), and WHR. Circumferences were measured by members of the research team the day before surgery using a standardized technique and the same measuring tape.
Histopathological variables were classified according to the Brazilian Society of Hepatology criteria, which analyzes the parameters from a semi-quantitative and topological basis, using the criteria of Kleiner and collaborators [20, 21]. Histological parameters were classified as follows: macrovesicular and/or microvesicular steatosis (classified ordinally as absent (0), mild (1), moderate (2), and severe (3) and dichotomously as absent or present); steatohepatitis analyzed through the presence of acinar and/or portal inflammation (ordinally classified as absent (0), mild (1), moderate (2), and severe (3) and dichotomously classified as absent or present), and perisinusoidal and/or periportal fibrosis (classified ordinally as absent (0), mild (1), moderate (2), and severe (3) and dichotomously as absent or present).
Statistical Analysis
For the comparison of proportions, the chi-square test or Fisher’s exact test was used, when necessary. To compare continuous variables, the Mann-Whitney test was used. The analyses of correlations between continuous and/or ordinal variables were performed through simple and multiple linear regressions. Considering the disproportionately higher number of females in the current sample, subset analyses excluding male individuals were also performed. The level of significance used for the statistical tests will be 5% (p < 0.05). To perform the analyses, the computer program SAS System for Windows (Statistical Analysis System), version 9.2; SAS Institute Inc., 2002–2008, Cary, NC, USA, was used.
Results
Of the 119 individuals included, 105 (88.2%) were female. The mean age was 38.8 ± 9.3 years and the mean BMI was 37.6 ± 3.1 kg/m2. The prevalence of NAFLD histopathological aspects was: steatosis (91 individuals; 76.5%); steatohepatitis (59; 49.6%), and liver fibrosis (61; 51.3%). In regard to co-morbidities, it was observed that 55 individuals (46.2%) had hypertension, 18 (15.1%) presented T2D, and 27 (22.7%) had dyslipidemia.
Comparing individuals with or without steatosis, WC was significantly higher in individuals with steatosis (103.5 ± 9.9 vs. 99.4 ± 8.4; p = 0.03). Excluding males, individuals with steatosis had significantly higher WC (102.2 ± 9.6 vs. 98.3 ± 8; p = 0.04), triglycerides (117 ± 52.6 vs. 90 ± 47.5; p = 0.04), and total cholesterol (179.2 ± 43.7 vs. 153.6 ± 46.5; p = 0.03). There were no statistically significant differences regarding other variables (Table 1).
It was observed that individuals with steatohepatitis presented significantly higher BMI (38.2 ± 3.2 vs. 36.7 ± 2.8; p = 0.01), WC (105.3 ± 10.4 vs. 99.6 ± 8.8; p = 0.002), and WHR (1 ± 0.1 vs. 0.9 ± 0.1; p = 0.02) than individuals without steatohepatitis. Excluding males, BMI (38.2 ± 3.4 vs. 36.5 ± 2.8; p = 0.007) and WC (102.9 ± 9.6 vs. 98.7 ± 8.7; p = 0.02) were significantly higher in individuals with steatohepatitis. There were no significant differences in regard to other variables (Table 2).
As for liver fibrosis, it was observed that age (40.6 ± 9.7 vs. 37 ± 8.5; p = 0.03) and levels of hemoglobin A1c (6.5 ± 0.5 vs. 5.6 ± 0.5; p = 0.004) were significantly higher among individuals with fibrosis, with no significant differences in regard to other variables. Excluding males, ALT levels were significantly higher in individuals with fibrosis (24.3 ± 24.8 vs. 18.8 ± 8.9; p = 0.03) (Table 3).
Univariate correlation analysis was performed between the intensity of liver steatosis (outcome) and the study variables, and a statistically significant positive correlation was observed with WHR (R = 0.2; p = 0.04). Excluding males, WC was significantly and positively correlated with the intensity of steatosis (R = 0.2; p = 0.02); there was also a marginally significant and positive correlation between WHR and the intensity of steatosis (R = 0.2; p = 0.05). Table 4 presents the complete correlation analysis. After a multivariate analysis including significant or marginally significant variables associated with the intensity of steatosis in females, WC was independently associated with this outcome (R = 0.02; p = 0.02) (Table 5). Univariate correlation analysis between steatohepatitis intensity (outcome) and study variables revealed significant positive correlations between BMI (R = 0.2; p = 0.02), NC (R = 0.2; p = 0.03), WC (R = 0.2; p = 0.006), and blood glucose (R = 0.3; p = 0.005). Excluding males, BMI was independently associated with the intensity of steatohepatitis (R = 0.3; p = 0.006). Table 6 shows the complete univariate simple regression analysis for the outcome of steatohepatitis intensity. After identifying the significant variables in the univariate analysis, multivariate analysis was performed using multiple regression considering the entire study population, where it was observed that BMI (R = 0.2; p = 0.02) and blood glucose (R = 0.2; p = 0.009) were independently correlated with steatohepatitis intensity (Table 7). Upon univariate correlation analysis between the intensity of liver fibrosis (outcome) and the study variables, significant correlations were observed with age (R = 0.3; p = 0.004), blood glucose (R = 0.2; p = 0.03), and hemoglobin A1c (R = 0.2; p = 0.04). Excluding males, no significant variable was identified. Table 8 shows the complete univariate simple regression analysis for the outcome of fibrosis intensity. After identifying the significant variables in the univariate analysis considering the entire study population, multivariate analysis was performed using multiple regression, where it was observed that age (R = 0.3; p = 0.04) was independently correlated with the intensity of fibrosis (Table 9).
Discussion
Among the main findings of the present study, the significance of both WC and WHR as markers of steatosis stands out. Both are indirect anthropometric markers of body fat distribution usually correlated with the volume of visceral fat [17, 22]. BMI, the most widely used anthropometric marker in daily clinical practice, was significant only among individuals with steatohepatitis. Among individuals with hepatic fibrosis, there were no anthropometric markers that differed significantly; age and hemoglobin A1c were significantly higher among these individuals, indicating that the duration of the disease and the degree of insulin resistance are more important than the anthropometric parameters at this stage of the disease. The present findings confirm the precedence of WC and WHR as reliable markers of visceral adiposity, and this is also true in the assessment of liver disease [23]. In addition, there was a significant and independent positive correlation between WHR and steatosis intensity, indicating that the higher the WHR, the greater the severity of steatosis. Likewise, BMI and glucose showed positive and independent correlations with the intensity of the steatohepatitis, indicating that the higher both parameters, the greater the severity of the steatohepatitis. Fibrosis, on the other hand, showed a significantly positive and independent correlation with age, indicating that in this population, the older the individual, the greater the degree of liver fibrosis. NC was not significantly associated or independently correlated with any of the histopathological aspects of NAFLD analyzed in the study population.
According to studies carried out by Atri et al. [24] in a population of 106 Indian women with morbid obesity, in which 73.6% had NAFLD diagnosed by ultrasound, WC, BMI, and waist-to-height ratio were significantly associated with steatosis. Another relevant finding of the present study was that HC did not prove to be an isolated significant anthropometric protective factor for steatosis, steatohepatitis, or fibrosis. Katz et al. [25] previously observed that, among 1776 Chinese women, HC had an inverse and strong relationship with high levels of triglycerides and low levels of HDL. Similarly, Snijder et al. [26] observed, in a study which enrolled 11,247 participants, that HC had an inverse and independent relationship with the presence of diabetes, hypertension, and dyslipidemia. On the other hand, the current study did not demonstrate negative correlations, that is, protection between HC and aspects of the NAFLD spectrum. It is likely that the results presented by the aforementioned authors may be reproducible in more heterogeneous populations, composed of individuals with or without obesity, whereas in the current study, whose population only comprised individuals with severe obesity, this association could not be observed. Another hypothesis is that the metabolic protection provided by HC in such studies does not extend to NAFLD, being limited to other components of cardiometabolic risk. Further research is needed to reach more comprehensive conclusions in this regard.
NC, defended by some researchers as so significant as WC as an anthropometric marker of metabolic disease [27, 28], did not show associations with NAFLD in the current study. In a study by Borel et al. [22] which enrolled 305 French adult women with severe obesity, it was observed that NC was a clinically relevant anthropometric predictor of central obesity. In another study by Huang et al. [27], in an adult Chinese population composed of 4053 individuals, NC was associated with a higher prevalence of NAFLD diagnosed by ultrasound scan, being considered by the authors as a valuable predictor of NAFLD, especially when analyzed in conjunction with other anthropometric measurements, such as WC and HC. For Li et al. [28], NC was an independent predictor of NAFLD diagnosed by ultrasound scan in lean men in a population of 2668 adults in Shanghai in Eastern China. According to the study by Jian et al. [29] in a sample of 1698 Chinese adults, it was observed that NC is an effective supplementary parameter for screening NAFLD assessed by ultrasound scan; there was a significant and positive correlation between NC and liver fat content. The findings of the present study do not corroborate these results. It must be considered that such results refer to studies carried out in populations of varying ethnicities, so that they are likely not entirely reproducible in the Brazilian population. Furthermore, the current study used histopathological examinations for the diagnosis of NAFLD and its aspects, while the aforementioned studies mostly used imaging methods for this purpose.
In multivariate analyses, it was shown that BMI and hemoglobin A1c were markers independently correlated with the intensity of steatohepatitis, i.e., the greater their values, the more intense the inflammation, emphasizing the importance of glucose metabolism on steatohepatitis. In a literature review carried out by Wattacheril et al. [30] and in the study carried out by Pappachan et al. [31], the various pathophysiological pathways that are involved in the progression and pathogenesis of steatohepatitis are shown, among them, the pathway of abnormal glucose metabolism and insulin [32].
Currently, there is no consensus on the use of anthropometric parameters for screening and diagnosis of NAFLD. These divergences have a multifactorial origin in relation to these parameters, which may be related to factors such as ethnicity, age, gender, genetic, and socioeconomic aspects, as well as varying samples and methodology issues [27,28,29, 31, 33, 34]. Despite these controversies, it is possible, through the findings of the present study, to postulate that the measurement of WC and WHR are simple and easily reproducible ways of screening individuals with risk factors for NAFLD and NAFLD. The adoption of this measurement as a routine in daily outpatient care of the bariatric population could be used as an instrument to indicate the need for further laboratory and imaging tests in order to diagnose and perform the risk gradation of severe forms for NAFLD. In addition, it could establish criteria for greater metabolic risk during the discussion on treatment options for these individuals, particularly with regard to the indication of bariatric/metabolic surgery, especially a greater emphasis on the importance of WC and WHR over BMI alone [3, 6, 18, 35, 36]. Considering the difficulty to detect NAFLD by visual inspection during surgical procedures, these parameters may also help to select individuals with more necessity of intraoperative liver biopsy during bariatric surgery [37,38,39].
The present study has limitations that must be considered. The population was exclusively composed of individuals with obesity undergoing bariatric surgery, thus it is considerably homogeneous and does not allow a prompt extrapolation of the findings to more heterogeneous groups. Nevertheless, the histopathological assessment of NAFLD is an extremely relevant strength of this research, providing a nuanced analysis of the disease spectrum, which is not possible and neither so accurate in studies based on imaging methods.
Conclusions
Anthropometric parameters were significantly associated with the occurrence of NAFLD histopathological aspects in individuals undergoing bariatric surgery. WC and WHR were associated with the occurrence of steatosis; BMI, WC, and WHR were associated with the occurrence of steatohepatitis. A significant positive correlation was identified between WHR and steatosis intensity.
References
Moore JB. Non-alcoholic fatty liver disease: the hepatic consequence of obesity and the metabolic syndrome. Proc Nutr Soc. 2010;69(2):211–20. https://doi.org/10.1017/S0029665110000030.
Lodh M, Debnath N, Mazumdar D, et al. Anthropometric and biochemical characteristics of adult patients with non-alcoholic fatty liver disease anthropometric and biochemical characteristics of adult patients with non-alcoholic fatty liver disease. Asian J Pharm Clin Res. 2019;12:501–5. https://doi.org/10.22159/ajpcr.2019.v12i1.29278.
Lonardo A, Mantovani A, Lugari S, et al. Epidemiology and pathophysiology of the association between NAFLD and metabolically healthy or metabolically unhealthy obesity. Ann Hepatol. 2020;19(4):359–66. https://doi.org/10.1016/j.aohep.2020.03.001.
Iacobini C, Pugliese G, Blasetti Fantauzzi C, et al. Metabolically healthy versus metabolically unhealthy obesity. Metabolism. 2019;92:51–60. https://doi.org/10.1016/j.metabol.2018.11.009.
Després JP. Body fat distribution and risk of cardiovascular disease: an update. Circulation. 2012;126(10):1301–13. https://doi.org/10.1161/CIRCULATIONAHA.111.067264.
Younossi ZM. Non-alcoholic fatty liver disease—a global public health perspective. J Hepatol. 2019;70(3):531–44. https://doi.org/10.1016/j.jhep.2018.10.033.
Webb VL, Wadden TA. Intensive lifestyle intervention for obesity: principles, practices, and results. Gastroenterology. 2017;152(7):1752–64. https://doi.org/10.1053/j.gastro.2017.01.045.
Fumagalli C, Maurizi N, Day SM, et al. SHARE Investigators. Association of obesity with adverse long-term outcomes in hypertrophic cardiomyopathy. JAMA Cardiol. 2020;5(1):65–72. https://doi.org/10.1001/jamacardio.2019.4268.
Lau DC. Metabolic syndrome: perception or reality? Curr Atheroscler Rep. 2009;11(4):264–71. https://doi.org/10.1007/s11883-009-0041-7.
Romero-Corral A, Somers VK, Sierra-Johnson J, et al. Normal weight obesity: a risk factor for cardiometabolic dysregulation and cardiovascular mortality. Eur Heart J. 2010;31(6):737–46. https://doi.org/10.1093/eurheartj/ehp487.
Wahab A, Dey AK, Bandyopadhyay D, et al. Obesity, systemic hypertension, and pulmonary hypertension: a tale of three diseases. Curr Probl Cardiol. 2021;46(3):100599. https://doi.org/10.1016/j.cpcardiol.2020.100599.
Goossens GH. The metabolic phenotype in obesity: fat mass, body fat distribution, and adipose tissue function. Obes Facts. 2017;10(3):207–15. https://doi.org/10.1159/000471488.
Cazzo E, Callejas-Neto F, Pareja JC, et al. Correlation between post over preoperative surrogate insulin resistance indexes’ ratios and reversal of metabolic syndrome after Roux-en-Y gastric bypass. Obes Surg. 2014;24(6):971–3. https://doi.org/10.1007/s11695-014-1246-6.
Alberti KG, Zimmet P, Shaw J. Metabolic syndrome—a new world-wide definition. A consensus statement from the international diabetes federation. Diabet Med. 2006;23(5):469–80. https://doi.org/10.1111/j.1464-5491.2006.01858.x.
Expert panel on detection, evaluation, and treatment of high blood cholesterol in adults. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III). JAMA. 2001;285(19):2486-97. https://doi.org/10.1001/jama.285.19.2486.
Sánchez M, Sánchez E, Bermúdez-López M, et al. On Behalf Of The Ilervas Project Collaborators. Clinical usefulness of anthropometric indices to predict the presence of prediabetes. Data from the ILERVAS Cohort. Nutrients. 2021;13(3):1002. https://doi.org/10.3390/nu13031002.
Joshipura K, Muñoz-Torres F, Vergara J, et al. Neck circumference may be a better alternative to standard anthropometric measures. J Diabetes Res. 2016;2016:6058916–8. https://doi.org/10.1155/2016/6058916.
Balhareth A, Meertens R, Kremers S, et al. Overweight and obesity among adults in the Gulf States: a systematic literature review of correlates of weight, weight-related behaviours, and interventions. Obes Rev. 2019;20(5):763–93. https://doi.org/10.1111/obr.12826.
Pouliot MC, Després JP, Lemieux S, et al. Waist circumference and abdominal sagittal diameter: best simple anthropometric indexes of abdominal visceral adipose tissue accumulation and related cardiovascular risk in men and women. Am J Cardiol. 1994;73(7):460–8. https://doi.org/10.1016/0002-9149(94)90676-9.
Cotrim HP, Parise ER, Oliveira CP, et al. Nonalcoholic fatty liver disease in Brazil. Clinical and histological profile. Ann Hepatol. 2011;10(1):33–7.
Kleiner DE, Brunt EM, Van Natta M, et al. Design and validation of a histological scoring system for nonalcoholic fatty liver disease. Hepatology. 2005;41(6):1313–21. https://doi.org/10.1002/hep.20701.
Borel AL, Coumes S, Reche F, et al. Waist, neck circumferences, waist-to-hip ratio: which is the best cardiometabolic risk marker in women with severe obesity? The SOON cohort. PLoS One. 2018;13(11):1–15. https://doi.org/10.1371/journal.pone.0206617.
Cazzo E, Jimenez LS, Gallo Fde F, et al. Influence of type 2 diabetes mellitus on liver histology among morbidly obese individuals. A cross-sectional study. Sao Paulo Med J. 2016;134(1):79–83. https://doi.org/10.1590/1516-3180.2015.01652409.
Atri A, Jiwanmall SA, Nandyal MB, et al. The prevalence and predictors of non-alcoholic fatty liver disease in morbidly obese women—a cross-sectional study from Southern India. Eur Endocrinol. 2020;16(2):152–5. https://doi.org/10.17925/EE.2020.16.2.152.
Katz EG, Stevens J, Truesdale KP, et al. Hip circumference and incident metabolic risk factors in Chinese men and women: the People’s Republic of China study. Metab Syndr Relat Disord. 2011;9(1):55–62. https://doi.org/10.1089/met.2010.0045.
Snijder MB, Zimmet PZ, Visser M, et al. Independent and opposite associations of waist and hip circumferences with diabetes, hypertension and dyslipidemia: the AusDiab Study. Int J Obes Relat Metab Disord. 2004;28(3):402–9. https://doi.org/10.1038/sj.ijo.0802567.
Huang BX, Zhu MF, Wu T, et al. Neck circumference, along with other anthropometric indices, has an independent and additional contribution in predicting fatty liver disease. PLoS One. 2015;10(2):e0118071. https://doi.org/10.1371/journal.pone.0118071.
Li Q, Wang N, Han B, et al. Neck circumference as an independent indicator to non-alcoholic fatty liver disease in non-obese men. Nutr Metab (Lond). 2015;12:63. https://doi.org/10.1186/s12986-015-0060-z.
Jian C, Xu Y, Ma X, et al. Neck circumference is an effective supplement for nonalcoholic fatty liver disease screening in a community-based population. Int J Endocrinol. 2020;2020:7982107–6. https://doi.org/10.1155/2020/7982107.
Wattacheril J, Issa D, Sanyal A. Nonalcoholic steatohepatitis (NASH) and hepatic fibrosis: emerging therapies. Annu Rev Pharmacol Toxicol. 2018;58:649–62. https://doi.org/10.1146/annurev-pharmtox-010617-052545.
Pappachan JM, Babu S, Krishnan B, et al. Non-alcoholic fatty liver disease: a clinical update. J Clin Transl Hepatol. 2017;5(4):384–93. https://doi.org/10.14218/JCTH.2017.00013.
Cazzo E, Jimenez LS, Gestic MA, et al. Type 2 diabetes mellitus and simple glucose metabolism parameters may reliably predict nonalcoholic fatty liver disease features. Obes Surg. 2018;28(1):187–94. https://doi.org/10.1007/s11695-017-2829-9.
Ballestri S, Nascimbeni F, Romagnoli D, et al. The independent predictors of non-alcoholic steatohepatitis and its individual histological features: insulin resistance, serum uric acid, metabolic syndrome, alanine aminotransferase and serum total cholesterol are a clue to pathogenesis and candidate t. Hepatol Res. 2016;46(11):1074–87. https://doi.org/10.1111/hepr.12656.
Onat A, Hergenç G, Yüksel H, et al. Neck circumference as a measure of central obesity: associations with metabolic syndrome and obstructive sleep apnea syndrome beyond waist circumference. Clin Nutr. 2009;28(1):46–51. https://doi.org/10.1016/j.clnu.2008.10.006.
Pineda E, Sanchez-Romero LM, Brown M, et al. Forecasting future trends in obesity across Europe: the value of improving surveillance. Obes Facts. 2018;11(5):360–71. https://doi.org/10.1159/000492115.
Jimenez LS, Marques RA, Gestic MA, et al. Non-invasive markers in non-alcoholic fatty liver disease: reliability is variable according to BMI status. Obes Surg. 2021; https://doi.org/10.1007/s11695-021-05429-3.
Tota-Maharaj R, Blaha MJ, Zeb I, et al. Ethnic and sex differences in fatty liver on cardiac computed tomography: the multi-ethnic study of atherosclerosis. Mayo Clin Proc. 2014;89(4):493–503. https://doi.org/10.1016/j.mayocp.2013.12.015.
Petrick A, Benotti P, Wood GC, et al. Utility of ultrasound, transaminases, and visual inspection to assess nonalcoholic fatty liver disease in bariatric surgery patients. Obes Surg. 2015;25(12):2368–75.
Sousa-Filho PHF, Jimenez LS, Callejas GH, et al. Bilobar hepatic histological variability in obese individuals undergoing bariatric surgery: an analysis of paired wedge biopsies. Obes Surg. 2020;30(12):5125–8. https://doi.org/10.1007/s11695-020-04991-6.
Funding
Rodolfo A. Marques was funded by the Institutional Scientific Initiation Scholarship Program–Universidade de Campinas (PIBIC–UNICAMP).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Statement of Human and Animal Rights
The study was approved by the local committee of ethics in research under the opinion 3.512.406/UNICAMP (CAAE 16562219.0.0000.5404) and all participants signed an informed consent form. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Statement of Informed Consent
Informed consent was obtained from all individual participants included in the study.
Conflict of Interest
The authors declare no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Work developed at: Dept. of Surgery-Faculty of Medical Sciences, State University of Campinas (UNICAMP), Campinas (SP), Brazil.
Key Points:
• Waist circumference and waist-to-hip ratio were associated with steatosis.
• Body mass index, waist circumference, and waist-to-hip ratio were associated with steatohepatitis.
• Waist-to-hip ratio independently correlated with steatosis intensity.
Rights and permissions
About this article

Cite this article
Reis, S.S., Callejas, G.H., Marques, R.A. et al. Correlation Between Anthropometric Measurements and Non-alcoholic Fatty Liver Disease in Individuals With Obesity Undergoing Bariatric Surgery: Cross-Sectional Study. OBES SURG 31, 3675–3685 (2021). https://doi.org/10.1007/s11695-021-05470-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-021-05470-2