
Abstract
Background
Many respectable guidelines recommend lifelong vitamin B12 injections for Roux-en-Y gastric bypass (RYGB) patients in the absence of lack of consensus on the efficacy of oral route of prophylaxis and the appropriate doses needed for this purpose. The purpose of this review was to examine the published English language scientific literature in accordance with PRISMA principles to find out if orally given vitamin B12 is adequate for prophylactic purposes in RYGB patients and the appropriate dosages needed for this purpose if it is.
Methods
We examined the PubMed database for all English language articles examining various doses of oral vitamin B12 supplementation after proximal RYGB in adult patients. The search revealed 19 such articles.
Results
The data suggest that oral vitamin B12 supplementation doses of ≤ 15 μg daily are insufficient to prevent deficiency in RYGB patients. Higher supplementation doses show better results and it appears that a dose of 600.0 μg vitamin B12 daily is superior to 350.0 μg daily suggesting an incremental dose-response curve. It further appears that supplementation doses of 1000.0 μg vitamin B12 daily lead to an increase in B12 levels and are sufficient for the prevention of its deficiency in most RYGB patients.
Conclusion
The review finds that oral supplementation doses of ≤ 15 μg vitamin B12 daily are inadequate for prophylaxis of vitamin B12 deficiency in adult RYGB patients but doses of 1000 μg vitamin B12 daily might be adequate. Future studies need to examine this and even higher oral doses for vitamin B12 supplementation for patients undergoing RYGB.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Vitamin B12 is an essential micronutrient. Its deficiency can lead to anemia and neurological dysfunction, which could be irreversible if untreated. Approximately 5.0–6.0% of patients considering bariatric surgery are deficient in vitamin B12 [1, 2] and Roux-en-Y gastric bypass (RYGB) further aggravates it [3] through a combination of decreased intake [4], lack of intrinsic factor, reduced gastric acid, and impaired absorption due to bypass of proximal small intestine. It is widely recognized that RYGB patients need additional vitamin B12 supplementation [5]. In the UK, the British Obesity and Metabolic Surgery Society (BOMSS) nutritional guidelines [5] recommend 3-month intramuscular injection for these patients and there is evidence to suggest that this is sufficient to prevent vitamin B12 deficiency in RYGB patients [6]. At the same time, regular lifelong injections pose an additional demand on already constrained healthcare resources and may put some patients off having a gastric bypass. It would hence be useful to understand if the same can be achieved through oral vitamin B12 supplementation and the dose needed for that purpose.
It is widely recognized that a 3-month injection of 1 mg vitamin B12 subcutaneously is sufficient to prevent vitamin B12 deficiency in RYGB patients [6] but it is unclear if the same can also be achieved through oral supplementation and the oral dosages needed if that is the case. Recent guidelines by the American Society for Metabolic and Bariatric Surgery (ASMBS) suggest an oral dose of 350–500 μg vitamin B12 daily for all bariatric surgery patients [7]. The guidelines do not make any distinction between different procedures and it is unclear if these doses are sufficient for all RYGB patients.
The purpose of this review was to identify the appropriate dose of oral vitamin B12 supplementation after RYGB. We investigated the entire English language scientific literature on oral vitamin B12 supplementation and deficiency after RYGB in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Methods
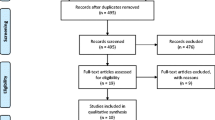
An online search of PubMed was carried out using keywords like “bariatric surgery,” “gastric bypass,” “Roux en Y Gastric Bypass,” and “B12,” and to identify all English language articles specifically examining doses of oral vitamin B12 supplementation after proximal RYGB in adult patients. Articles were also identified from references of relevant articles. Last of these searches was carried out on 22 September 2017. Review articles were excluded as were those that pooled results with different procedures together [8, 9]. Articles on distal RYGB [10] and banded RYGB [11] were also excluded. Articles that reported on vitamin B12 deficiency without clearly mentioning the supplementation dosages had to be excluded as these would not allow us to determine the appropriate supplementation dose for oral vitamin B12 supplementation after RYGB. Case reports were also excluded. Finally, we excluded articles where authors had evaluated non-oral routes for supplementing vitamin B12 as the purpose of this review was to ascertain the effectiveness of oral route for supplementation of vitamin B12. A total of 19 articles were included. Figure 1 gives a PRISMA flow chart for article selection.

PRISMA flow chart for article selection
Results
Studies on Oral Vitamin B12 Supplementation in Doses up to 15.0 μg Daily
Table 1 [12,13,14,15,16,17,18,19,20,21] summarizes studies that examined oral vitamin B12 in supplementation doses of up to 15.0 μg daily. It would appear from these studies that even in the early period after RYGB when the body reserves of vitamin B12 are unlikely to have been exhausted, these oral doses of vitamin B12 are insufficient for the prevention of vitamin B12 deficiency. The data suggest that standard multivitamins do not contain dosages of vitamin B12 sufficient enough to prevent deficiency in RYGB patients.
Studies on Oral Vitamin B12 Supplementation in Doses from 16.0 to 999.0 μg Daily
Table 2 [1, 4, 19, 22,23,24] summarizes studies that examined oral vitamin B12 in supplementation doses from 16.0 to 999.0 μg daily and shows better results than studies in Table 1. Results also appear better with a dose of 600.0 μg vitamin B12 daily [22] in comparison with 350.0 μg daily [1, 19, 23] suggesting an incremental dose-response curve in this dose range.
Studies on Oral Vitamin B12 Supplementation in Doses of 1000.0 μg Daily or More
Table 3 [25,26,27] summarizes studies that examined oral vitamin B12 in supplementation doses of 1000.0 μg daily. It appears that these doses lead to an increase in vitamin B12 levels and are sufficient for the prevention of deficiency in most patients. There is no study in the scientific literature examining prophylactic doses of > 1000.0 μg daily in these patients.
Discussion
There is little doubt that RYGB patients need vitamin B12 supplementation to prevent subclinical and clinical deficiency as many patients are already deficient in vitamin B12 at the time of surgery and RYGB leads to further reduction in intake and absorption of vitamin B12. Though there is no doubt that vitamin B12 injections at regular intervals, as recommended by the BOMSS guidelines [5], are sufficient to prevent deficiency in these patients, it does involve regular visits to primary care and it is possible that some patients would prefer to avoid regular lifelong injections if possible.
It is worth mentioning in this context that recent ASMBS guidelines [7] recommend routine preoperative screening for vitamin B12 levels because “2–18% patients with obesity suffer from vitamin B12 deficiency and the prevalence increases to 6–30% in those taking proton-pump inhibitors.” Preoperative screening seems logical for those patients who are not going to be routinely supplemented after surgery; however, there is likely to be a minimal benefit for those who would receive routine supplementation after surgery.
This review shows that dosages of vitamin B12 contained in a standard over-the-counter preparation (Table 1) are insufficient following RYGB. When very low supplementation doses are used [20], a progressively increasing number of patients become deficient in vitamin B12 with an increasing duration of follow-up as their body stores get depleted. Since the vitamin B12 stores are expected to be even lower in bariatric surgery patients than the normal population, they may become deficient soon after surgery [20].
It is further evident that even doses many times higher than that contained in a standard multivitamin are also inadequate. In the randomized study by Dogan et al. [1] and their 3-year follow-up study [23], even when 350 μg of vitamin B12 daily supplementation was given following RYGB, a large number of patients become vitamin B12 deficient and needed further supplementation. At the same time, authors demonstrated a higher level and lower incidence of deficiency in the group given a higher dosage of 350 μg daily compared to the standard dose of 12.5 μg daily. Given these findings, it would be useful to examine even higher dosages. This is exactly what Boyce et al. [22] did and they reported a 0.6% deficiency rate at 12 months amongst patients recommended with 600 μg vitamin B12 daily.
Though the deficiency rate was very low with 600 μg daily [22], it would only be natural to examine if even higher dosages were more effective. The study by van der Beek et al. [28] can be useful to understand the effect of higher dosages of oral vitamin B12 in these patients. The authors [28] found that the oral dose of 1000 μg a day can successfully treat post-RYGB patient vitamin B12 deficiency in 86.0% of patients. This is slightly higher than 80.0% correction of vitamin B12 deficiency with an oral dose of 500 μg/day as observed by Brolin et al. [29].
If a dose of 1000 μg daily is successful for the treatment in the majority of patients, one can naturally infer that it would also be effective for prophylaxis. This is indeed what other authors have also suggested [25, 27]. But deficiency rates of nearly 6.0% seen by del Villar Madrigal et al. [26] in patients advised with 1000 μg vitamin B12 daily seem to contradict the assumption that a daily oral dose of 1000 μg is adequate for all post-RYGB patients for prophylaxis of vitamin B12 deficiency. However, these authors did not report compliance and it cannot hence be ruled out as a potential explanation of these observed discrepancies. At the same time, we cannot assume lack of compliance to be the reason for these observed findings. It is hence important to prospectively examine the adequacy of 1000 μg vitamin B12 daily given orally in these patients.
It has been suggested that though intrinsic factor-dependent absorption of vitamin B12 is reduced after RYGB, absorption of oral crystalline vitamin B12 can also take place through diffusion. But this route probably requires much higher dosages to be completely effective for prophylactic purposes [9]. It has been shown [30] that though absorption of food-bound vitamin B12 was severely impaired after RYGB, absorption of free vitamin B12 largely remained unchanged. On the basis of these data, authors suggested that daily supplementation using oral crystalline vitamin B12 was an acceptable route for supplementation for RYGB patients.
The studies in this review confirm that though proportionately very small, some absorption of vitamin B12 does take place in RYGB patients. Moreover, there is little doubt that intestinal adaptation takes place [31] after RYGB to maximize orally consumed vitamin B12 absorption.
It should hence follow that if we give a high enough dose of vitamin B12, we should be able to use the oral route of supplementation in these patients. Since there are practically no side effects of an excess of vitamin B12 [32], we can trial even higher dosages that will not only prevent deficiency in all patients but also be permissive towards intermittent non-compliance. We probably over-supplement with parenteral injection too as we routinely see higher than normal levels of vitamin B12 in our practice with 3-month 1-mg intramuscular vitamin B12 injections.
Conclusion
Some absorption of orally administered vitamin B12 does take place in post-RYGB patients but the dosages needed are much larger than that contained in most standard over-the-counter multivitamin formulations. A dose of 1000 μg vitamin B12 daily seems adequate for prophylaxis in most RYGB patients but needs to be examined in prospective studies over longer periods of time. It is possible that even higher oral dosages may deliver better outcomes.
Abbreviations
- RYGB:
-
Roux-en-Y gastric bypass
- BOMSS:
-
British Obesity and Metabolic Surgery Society
- ASMBS:
-
American Society for Metabolic and Bariatric Surgery
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
References
Dogan K, Aarts EO, Koehestanie P, et al. Optimization of vitamin suppletion after Roux-en-Y gastric bypass surgery can lower postoperative deficiencies: a randomized controlled trial. Medicine (Baltimore). 2014;93(25):e169. https://doi.org/10.1097/MD.0000000000000169.
Peterson LA, Cheskin LJ, Furtado M, et al. Malnutrition in bariatric surgery candidates: multiple micronutrient deficiencies prior to surgery. Obes Surg. 2016;26(4):833–8. https://doi.org/10.1007/s11695-015-1844-y.
Weng TC, Chang CH, Dong YH, et al. Anaemia and related nutrient deficiencies after Roux-en-Y gastric bypass surgery: a systematic review and meta-analysis. BMJ Open. 2015;5(7):e006964. https://doi.org/10.1136/bmjopen-2014-006964.
Gesquiere I, Foulon V, Augustijns P, et al. Micronutrient intake, from diet and supplements, and association with status markers in pre- and post-RYGB patients. Br J Clin Pharmacol. 2016;82(5):1325–32. https://doi.org/10.1111/bcp.13054.
O’Kane M, Pinkney J, Aasheim E, Barth J, Batterham R, Welbourn R. BOMSS Guidelines on perioperative and postoperative biochemical monitoring and micronutrient replacement for patients undergoing bariatric surgery. Adopted by BOMSS Council September 2014. http://www.bomss.org.uk/wp-content/uploads/2014/09/BOMSS-guidelines-Final-version1Oct14.pdf. Last Accessed on 7 Oct 2017
Worm D, Madsbad S, Kristiansen VB, et al. Changes in hematology and calcium metabolism after gastric bypass surgery—a 2-year follow-up study. Obes Surg. 2015;25(9):1647–52. https://doi.org/10.1007/s11695-014-1568-4.
Parrott J, Frank L, Rabena R, et al. American Society for Metabolic and Bariatric Surgery integrated health nutritional guidelines for the surgical weight loss patient 2016 update: micronutrients. Surg Obes Relat Dis. 2017;13(5):727–41. https://doi.org/10.1016/j.soard.2016.12.018.
Bergeat D, Lechaux D, Ghaina A, et al. Postoperative outcomes of laparoscopic bariatric surgery in older obese patients: a matched case-control study. Obes Surg. 2017;27(6):1414–22. https://doi.org/10.1007/s11695-016-2517-1.
Rhode BM, Tamin H, Gilfix BM, et al. Treatment of vitamin B12 deficiency after gastric surgery for severe obesity. Obes Surg. 1995;5(2):154–8. https://doi.org/10.1381/096089295765557953.
Srikanth MS, Oh KH, Fox SR. Revision to malabsorptive Roux-en-Y gastric bypass (MRNYGBP) provides long-term (10 years) durable weight loss in patients with failed anatomically intact gastric restrictive operations: long-term effectiveness of a malabsorptive Roux-en-Y gastric bypass in salvaging patients with poor weight loss or complications following gastroplasty and adjustable gastric bands. Obes Surg. 2011;21(7):825–31. https://doi.org/10.1007/s11695-010-0280-2.
Pajecki D, Dalcanalle L, Souza de Oliveira CP, et al. Follow-up of Roux-en-Y gastric bypass patients at 5 or more years postoperatively. Obes Surg. 2007;17(5):601–7. https://doi.org/10.1007/s11695-007-9104-4.
Coupaye M, Rivière P, Breuil MC, et al. Comparison of nutritional status during the first year after sleeve gastrectomy and Roux-en-Y gastric bypass. Obes Surg. 2014;24(2):276–83. https://doi.org/10.1007/s11695-013-1089-6.
Coupaye M, Puchaux K, Bogard C, et al. Nutritional consequences of adjustable gastric banding and gastric bypass: a 1-year prospective study. Obes Surg. 2009;19(1):56–65. https://doi.org/10.1007/s11695-008-9571-2.
Dalcanale L, Oliveira CP, Faintuch J, et al. Long-term nutritional outcome after gastric bypass. Obes Surg. 2010;20(2):181–7. https://doi.org/10.1007/s11695-009-9916-5.
Donadelli SP, Junqueira-Franco MV, de Mattos Donadelli CA, et al. Daily vitamin supplementation and hypovitaminosis after obesity surgery. Nutrition. 2012;28(4):391–6. https://doi.org/10.1016/j.nut.2011.07.012.
Gasteyger C, Suter M, Gaillard RC, et al. Nutritional deficiencies after Roux-en-Y gastric bypass for morbid obesity often cannot be prevented by standard multivitamin supplementation. Am J Clin Nutr. 2008;87(5):1128–33.
Gehrer S, Kern B, Peters T, et al. Fewer nutrient deficiencies after laparoscopic sleeve gastrectomy (LSG) than after laparoscopic Roux-Y-gastric bypass (LRYGB)—a prospective study. Obes Surg. 2010;20(4):447–53. https://doi.org/10.1007/s11695-009-0068-4.
Provenzale D, Reinhold RB, Golner B, et al. Evidence for diminished B12 absorption after gastric bypass: oral supplementation does not prevent low plasma B12 levels in bypass patients. J Am Coll Nutr. 1992;11(1):29–35. https://doi.org/10.1080/07315724.1992.10718193.
Rhode BM, Arseneau P, Cooper BA, et al. Vitamin B-12 deficiency after gastric surgery for obesity. Am J Clin Nutr. 1996;63(1):103–9.
Aarts EO, van Wageningen B, Janssen IM, et al. Prevalence of anemia and related deficiencies in the first year following laparoscopic gastric bypass for morbid obesity. J Obes. 2012;2012:193705.
Vargas-Ruiz AG, Hernández-Rivera G, Herrera MF. Prevalence of iron, folate, and vitamin B12 deficiency anemia after laparoscopic Roux-en-Y gastric bypass. Obes Surg. 2008;18(3):288–93. https://doi.org/10.1007/s11695-007-9310-0.
Boyce SG, Goriparthi R, Clark J, et al. Can composite nutritional supplement based on the current guidelines prevent vitamin and mineral deficiency after weight loss surgery? Obes Surg. 2016;26(5):966–71. https://doi.org/10.1007/s11695-015-1853-x.
Homan J, Schijns W, Aarts EO, et al. An optimized multivitamin supplement lowers the number of vitamin and mineral deficiencies three years after Roux-en-Y gastric bypass: a cohort study. Surg Obes Relat Dis. 2016;12(3):659–67. https://doi.org/10.1016/j.soard.2015.12.010.
Moore CE, Sherman V. Effectiveness of B vitamin supplementation following bariatric surgery: rapid increases of serum vitamin B12. Obes Surg. 2015;25(4):694–9. https://doi.org/10.1007/s11695-014-1441-5.
Aasheim ET, Björkman S, Søvik TT, et al. Vitamin status after bariatric surgery: a randomized study of gastric bypass and duodenal switch. Am J Clin Nutr. 2009;90(1):15–22. https://doi.org/10.3945/ajcn.2009.27583.
Del Villar ME, Neme-Yunes Y, Clavellina-Gaytan D, et al. Anemia after Roux-en-Y gastric bypass. How feasible to eliminate the risk by proper supplementation? Obes Surg. 2015;25(1):80–4.
von Drygalski A, Andris DA, Nuttleman PR, et al. Anemia after bariatric surgery cannot be explained by iron deficiency alone: results of a large cohort study. Surg Obes Relat Dis. 2011;7(2):151–6. https://doi.org/10.1016/j.soard.2010.04.008.
van der Beek ES, Monpellier VM, Eland I, et al. Nutritional deficiencies in gastric bypass patients; incidence, time of occurrence and implications for post-operative surveillance. Obes Surg. 2015;25(5):818–23. https://doi.org/10.1007/s11695-014-1456-y.
Brolin RE, Gorman JH, Gorman RC, et al. Are vitamin B12 and folate deficiency clinically important after roux-en-Y gastric bypass? J Gastrointest Surg. 1998;2(5):436–42. https://doi.org/10.1016/S1091-255X(98)80034-6.
Smith CD, Herkes SB, Behrns KE, et al. Gastric acid secretion and vitamin B12 absorption after vertical Roux-en-Y gastric bypass for morbid obesity. Ann Surg. 1993;218(1):91–6. https://doi.org/10.1097/00000658-199307000-00014.
Sala P, Belarmino G, Torrinhas RS, et al. Gastrointestinal transcriptomic response of metabolic vitamin B12 pathways in Roux-en-Y gastric bypass. Clin Transl Gastroenterol. 2017;8(1):e212. https://doi.org/10.1038/ctg.2016.67.
Vitamin B12. Linus Pauling Institute. http://lpi.oregonstate.edu/mic/vitamins/vitamin-B12. Last Accessed on 1 Oct 2017.
Author information
Authors and Affiliations
Contributions
KM conceived the idea for the topic, performed the review, and wrote most of the manuscript. KM and AR independently searched for all the relevant articles. All other authors critically reviewed the manuscript and participated in the departmental discussions on the topic. All authors have seen the final version and approve of it.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Statement of Human and Animal Rights
Not applicable.
Statement of Informed Consent
Not applicable.
Rights and permissions
About this article

Cite this article
Mahawar, K.K., Reid, A., Graham, Y. et al. Oral Vitamin B12 Supplementation After Roux-en-Y Gastric Bypass: a Systematic Review. OBES SURG 28, 1916–1923 (2018). https://doi.org/10.1007/s11695-017-3102-y
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-017-3102-y