
Abstract
Background
Bile acids (BA) modulate lipid and glucose metabolism in a feedback loop through production of fibroblast growth factor (FGF) 19 in the terminal ileum. Changes in BA after bariatric surgery may lead to improvements in the metabolic syndrome, including fatty liver disease. This study investigated the relationship between BA and metabolic and inflammatory profiles after laparoscopic sleeve gastrectomy (LSG).
Methods
Patients undergoing LSG had fasting blood samples taken pre-operatively and 6 months post-surgery. Liver injury was measured using cytokeratin (CK) 18 fragments. BA were measured using liquid chromatography tandem-mass spectrometry. FGF-19 was measured using enzyme-linked immunosorbent assay.
Results
The study included 18 patients (12 females), with mean age 46.3 years (SEM ± 2.9) and BMI 60.1 kg/m2 (±2.6). After 6 months, patients lost 39.8 kg (±3.1; p < 0.001). Fourteen patients (78 %) had steatosis. FGF-19 increased from median 128.1 (IQR 89.4–210.1) to 177.1 (121.8–288.9, p = 0.045) at 6 months. Although total BA did not change, primary glycine- and taurine-conjugated BA, cholic acid decreased, and secondary BA, glycine-conjugated urodeoxycholic acid increased over the study period. These changes are associated with reduction in insulin resistance, pro-inflammatory cytokines and CK-18 levels.
Conclusions
The profile of individual BA is altered after LSG. These changes occur in the presence of reductions in inflammatory cytokines and markers of liver injury. This study supports evidence from recent animal models that LSG may have an effect on fatty liver through changes in BA metabolism.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Elevations in pro-inflammatory cytokines, including C-reactive protein (CRP), interleukin (IL)-6 and tumour necrosis factor (TNF) α, and oxidative stress are a causative link between obesity, increased adipose tissue, hyperlipidaemia and atherosclerotic cardiovascular disease [1].
Non-alcoholic fatty liver disease (NAFLD), with or without steatohepatitis (NASH), is found in up to 86 % of patients undergoing bariatric surgery and is the fastest growing cause of liver disease in the Western Hemisphere [2]. Accumulation of intracellular lipid and the pro-inflammatory cytokine milieu leads to reduced capacity in fat-laden hepatocytes to tolerate any insult, leading to increased hepatocellular injury and death [3]. Cytokeratin (CK)-18 is a marker of hepatocyte apoptosis. CK-18 M30 fragment levels are increased in NASH compared with obese NAFLD controls and correlate with fibrosis scores [4, 5]. NASH/NAFLD improves after bariatric surgery [6].
Bile acids (BA) are end products of cholesterol metabolism and are also signalling molecules, stimulating production of fibroblast growth factor (FGF) 19 in the terminal ileum. FGF-19 acts in the liver in a negative feedback loop by regulating cholesterol 7α-hydroxylase (CYP7A1) activity via the nuclear RXR farnesoid X receptor-α (FXR) [7]. BA also act via transmembrane G-protein coupled receptor (TGR5) [8]. Both FXR and TGR5 are involved in regulating lipid metabolism and modulating inflammatory cytokines production by liver macrophages, monocytes and Kuppfer cells [9]. Insulin regulates BA composition, in part by regulating the BA 12α-hydroxylase (CYP8B1), and it has been shown that the ratio of 12α-hydroxylated/non-12α-hydroxylated BAs is associated with key features of insulin resistance [10].
Roux-en-Y gastric bypass (RYGB) increases FGF-19 and BA (fasting and postprandial) [11–14]. The effect of laparoscopic sleeve gastrectomy (LSG) on enterohepatic circulation in humans is less certain. Steinert et al. report no difference in the total BA over the first year after LSG, compared with the increases seen in the RYGB group [15]. Haluzikova et al. noted an increase in FGF-19 after 6 months of LSG without a change in the total BA [16].
Bechmann et al. investigated BA profiles in obese patients with NAFLD/NASH and found that serum BA was higher in NASH than that in the simple steatosis, as was CK-18 M30 [17]. Recently, Myronovych et al. have shown that sleeve gastrectomy (SG) in a high-fat diet mouse model leads to reduction in hepatic steatosis, independent of weight loss, associated with changes in cholic acid (CA) and glycine-conjugated ursodeoxycholic acid (GUDCA) [18]. The same group have demonstrated that the beneficial metabolic effects of increased BA after SG are not seen in FXR knockout mice which have elevated plasma TG levels, hepatic steatosis and elevated levels of TNFα and other pro-inflammatory cytokines [19]. These studies suggest that SG has a weight-independent metabolic effect on hepatic lipid metabolism and glycaemic control, mediated by BA through FXR.
Clinical studies have demonstrated that the FXR-FGF-BA axis is important in humans [20, 21]. Ursodeoxycholic acid (UDCA) is a secondary BA that exerts an anti-apoptotic effect on hepatocytes, reducing circulating TNFα levels and improving hepatic insulin sensitivity [22]. A systematic review of 12 studies of UDCA in 1160 patients has shown that treatment with oral UDCA leads to reduction in alanine aminotransferase (ALT) and reduced fibrosis and steatosis [23].
The aim of this study was to investigate whether changes in BA profile after LSG were associated with reduction in inflammation, insulin resistance, circulating lipids and markers of liver injury.
Methods
Participants
Patients undergoing LSG were recruited prospectively. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Inclusion criteria were age 18 to 75 years, meeting the National Institute of Health and Care Excellence (NICE) 2006 guidelines for bariatric surgery, that is BMI >40 kg/m2 or >35 kg/m2 with obesity-related complications [24]. Exclusions were known alcohol intake of over 20 g per day, any known chronic pre-existing liver disease (including alcoholic liver disease, autoimmune liver disease, metabolic storage diseases such as haemochromatosis), elevated transaminases, abnormal hepatitis serology or autoantibody screen, previous liver surgery, active psychiatric illness, bleeding tendency or prescribed anticoagulant medications. Informed consent was obtained from all individual participants included in the study.
Fasting venous blood samples were taken before surgery and 6 months after surgery. Samples underwent routine biochemistry and haematology analysis using an automated multi-analyser, The remaining samples were stored in aliquots at −80 °C for batch analysis of other markers. Liver tissue samples were taken using a 16 gauge Tru-Cut® spring-loaded biopsy needle (UK Medical Limited, Sheffield, UK) at the beginning of surgery for histopathological analysis.
All LSG were performed by a single surgeon (AGP), according to a previously described technique using a 38 French bougie [25].
Assays
Routine assays
The following were measured on the Advia 2400 (Siemens Healthcare, Frimley, UK): ALT, aspartate transaminase (AST), CRP, full lipid profile [(total cholesterol, TG, low-density lipoprotein (LDL), HDL], glucose and non-esterified fatty acids (NEFA). Insulin was measured using Advia Centaur (Siemens Healthcare, Frimley, UK) and glycated haemoglobin (HbA1c) by Menarini 9210 (A.Menarini Diagnostics Ltd., Berkshire, UK).
Insulin resistance was measured by calculating HOMA-IR as \( \frac{\mathrm{Fasting}\ \mathrm{glucose}\ \left(\mathrm{mmol}/\mathrm{l}\right)\times \mathrm{fasting}\ \mathrm{insulin}\left(\mathrm{mU}/\mathrm{l}\right)}{22.5} \) [26].
Biomarkers
The following assays were performed according to the manufacturer’s instructions: cytokines IL-6 and IL-10, TNFα and markers of liver injury, cytokeratin M30 and M65. TNFα, IL-6, IL-10 and leptin were measured using a bead-based multiplex array (Fluorokine® MultiAnalyte Profiling Kit, R&D Systems Europe Ltd, Abingdon, UK), and the results were read on a Luminex® Analyzer (Luminex B.V., Oosterhout, The Netherlands). Enzyme-linked immunosorbent assay (ELISA) were used for CK-18 M65 and M30 (M65® Classic and M30 Apoptosense®, PEVIVA AB, Bromma, Sweden, supplied through BIOAXXESS® UK, Malvern, UK), TRAIL and FasL (Quantikine ELISA, R&D Systems Europe Ltd., Abingdon, UK).
FGF-19 was measured using Quantikine Human FGF-19 Immunoassay (R&D Systems Europe Ltd., Abingdon, UK).
Bile Acids
Plasma unconjugated and glycine- or taurine-conjugated primary and secondary BA (15 fractions) were analysed using a high-performance liquid chromatography (JascoTM, USA) coupled to tandem mass spectrometry (Applied Biosystems, Cheshire, UK), with a modified and extended methodology initially described by Tagliacozzi et al. [27]. The 12α-hydroxylated BA [CA, deoxycholic acid (DCA) and their conjugated forms] and non-12α-hydroxylated BA (chenodeoxycholic acid (CDCA), lithocholic acid (LCA), UDCA and their-conjugated forms) were calculated.
Statistical Analysis
Statistical analyses were performed using SPSS 20 (SPSS, USA). Before comparative statistical tests were performed, outliers were sought visually using boxplots. The assumption of normality was tested for each parameter, using values of the difference between paired samples before and 6 months after surgery using Shapiro-Wilk’s test (p > 0.05). Only BMI, ALT and AST met the criteria of having minimal numbers of outliers and normally distributed paired differences. These data are therefore presented as mean with 95 % confidence intervals, and paired t tests were performed to compare the two time points. All other parameters are presented median ± interquartile range (IQR) unless otherwise stated and Mann-Whitney U tests were performed to compare time points.
For parameters whose values changed significantly between time points, a fold change ratio was calculated as [6-month value]/[Baseline value]. These values were log2 transformed. The assumption of normality was tested using Shapiro-Wilk’s test (p > 0.05). Linearity was checked visually using scatter plots. Pearson’s correlation was performed between these parameters to look for any significant associations. Clinical significance was determined if p < 0.05.
Results
Clinical Parameters and Biomarkers
The study included 18 patients (12 females), with mean age 46.3 years (SEM ± 2.9) and mean BMI 60.1 kg/m2 (±2.6). Liver biopsies showed that 14 patients (78 %) had steatosis, with a median NAFLD activity score of 5 (IQR 2.5–5), where a score of 5 or more is indicative of NASH [28]. After 6 months, patients lost mean 39.8 kg (±3.1) which represents mean total body weight loss of 23.6 % (±1.5). Liver transaminase levels were all within the normal range at outset and both ALT and AST decreased. Markers of glycaemic control and insulin resistance improved (Table 1). Seven patients had impaired fasting glycaemia pre-operatively, but at 6 months, six had normalised.
Pre-operative lipid profiles were all in the normal range, presumably as all patients with dyslipidemia were being treated with lipid-lowering medications (n = 11). All patients had discontinued statin therapy before the 6-month follow-up. Fasting NEFA levels decreased after 6 months (see Table 1). Pro-inflammatory markers, IL-6, leptin and CRP decreased. Furthermore, CK-18 fragments decreased.
FGF-19 and Bile Acids
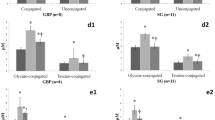
FGF-19 levels rose significantly over the study period, from a baseline median 128.1 (89.4–210.1) to 177.1(121.8–288.9, p = 0.045). This was not accompanied by a change in total BA concentration. More detailed analysis of specific constituent BA showed rises in secondary conjugated BA, glycoursodeoxycholic acid (GUDCA) and reductions in primary conjugated BA, glycocholic acid (GCA), and taurocholic acid (TCA) as well as secondary BA and DCA (Table 2).
Correlations
These results are summarised in Table 3. Pre-operatively, BMI correlated with CRP (Spearman’s rho = 0.596, p = 0.007) and post-operative BMI correlated with IL-6 (rho = 0.554, p = 0.04).
The reduction in GCA correlated with M30 (p = 0.003). The decrease in TCA correlated with the decrease in leptin (p = 0.04), and the reduction in DCA was associated with a decrease in fasting insulin (p = 0.019). There was no correlation between the increase in FGF-19 and BA concentrations, nor with HOMA-IR or inflammatory markers. The reduction in GCA and decrease in M30 levels also correlated (after log2 transformation, Pearson’s r = 0.700, p = 0.003).
Discussion
This is the first study to report significant changes in levels of individual primary and secondary BA and corroborates the findings of Haluzikova et al., who also showed an increase in FGF-19 after 6 months of LSG, with no change in total BA [16]. Of particular interest is the rise in UDCA following LSG and the associations between GCA, DCA and TCA with the expected post-LSG metabolic improvements, including lower insulin resistance and circulating CK-18 fragments.
Although lipid profiles did not change over the 6 months, this study shows for the first time that LSG leads to a decrease in circulating NEFA, associated with improved glycaemic control. NEFA levels are higher in obese and diabetic subjects [29]. The fall in NEFA may reflect a change in lipid processing and supports the hypothesis that LSG could lead to improvements in NAFLD through mechanisms other than weight loss or improved glycaemic control alone. RYGB has been shown to impact lipid profiles, and this effect may be independent of weight loss [30]. Further studies are required to confirm this effect in patients undergoing LSG.
Cytokines
LSG had a measurable impact on inflammatory markers, reducing CRP and IL-6 [31]. Leptin levels reduced by >50 % over the 6 months [32]. Consistent with multiple other studies, TNFα levels did not change significantly in this study [31]. IL-10 levels were also unchanged. Although it has anti-inflammatory effects in animal models and in vitro, the relationship between IL-10, obesity and NAFLD/NASH is not clearly elucidated [33]. Levels of pro-inflammatory cytokines correlate with BMI and confirm the relationship between increasing obesity and inflammation [34].
Liver Injury and Apoptosis
Improvement in NAFLD/NASH after bariatric surgery has been demonstrated using serial liver biopsies [6]. CK-18 levels fell after 6 months, and this study adds to the growing weight of evidence for its usefulness as a marker of fatty liver disease [4, 5]. Only two other studies have serially measured CK-18 levels after bariatric surgery. Diab et al. reported a median M30 level of 226U/L (IQR 177–298), which reduced by 44 % after 6 months [35], and Kahraman et al. report a reduction in both M30 and M65 after various types of bariatric surgery [36]. M30 also correlates with NAS, confirming its utility as a marker of NAFLD severity [35].
Bile Acids and Their Potential Effects on Fatty Liver and Metabolism
Total BA concentration did not change after LSG whilst FGF-19 levels increased by 51 % after 6 months, as shown previously [16].
One proposed mechanism for the increase in FGF-19 is through increased delivery of unmixed BA to the terminal ileum due to faster gastric emptying and intestinal transit post-LSG [37]. The increase in FGF-19 is accompanied by an increase in incretin release. This has also been postulated as a mechanism for improvement in T2DM post-RYGB [38] and confirmed in small animal models [39].
In this study, two primary conjugated BA, TCA and GCA levels decrease along with secondary BA DCA. The secondary BA GUDCA increased. Taken together, these changes may be due to altered BA conjugation/deconjugation metabolism by gut microbiota. The variety of species of gut microbiota changes after RYGB and is associated with altered expression of inflammation-associated genes in adipose tissue and alterations in BA profile [40]. These microbiota-induced changes may be due to alterations in circulating bacterial endotoxins, lipopolysaccharides (LPS), which produce an immune response [41]. Monte et al. have found that circulating LPS reduced after RYGB, with associated decrease in insulin resistance [42]. Although LSG has been shown to alter gut microbiota in a pilot study, no data regarding the effect on LPS are available at present [43]. Furthermore, the decrease in 12α-hydroxylated BA to non-12α-hydroxylated BA ratio 6 months post-LSG also reflects improvements in insulin sensitivity [10].
Given the interest and substantial experimental evidence that UDCA may be a potential treatment for NASH, it is pertinent to consider the importance of this finding, as GUDCA is the active metabolite of UDCA after glycine conjugation. In a mouse hepatocyte model, UDCA administration was associated with a hepato-protective effect, inhibiting apoptosis [22]. In both high-fat diet steatotic mice and a NASH mouse model, Pathil et al. showed that intraperitoneal injections of UDCA ameliorated signs of liver injury and altered lipid metabolism [44]. Similarly, Buko et al. found that UDCA reduced liver steatosis and inflammatory markers in a rat model of NASH [45]. In a rat model of SG, Myronovich et al. found that taurine-UDCA (the rat homolog of GUDCA) was increased. They also demonstrated that these changes were associated with altered hepatic gene expression and reduction in hepatic steatosis [18].
The fall in GCA correlates with a reduction in post-operative CK-18 M30 levels. Although there is little other supporting evidence for a direct role of GCA in inducing NASH from either in vitro or animal studies, there are studies suggesting that GCA is involved in liver injury. Luo et al. looked at patterns of BA fractions in various mouse models of drug-induced liver injury and found differentially altered CA, GCA and TCA levels associated with particular patterns of injury [46]. In NASH, CA, DCA and CDCA were found in elevated concentrations compared with controls and CA levels correlated with histological grading of inflammation [47].
This is the first study in humans to show that individual BA may have a role in reducing obesity-related inflammation, with reductions in both leptin and other pro-inflammatory cytokines also occurring over the study period. Changes in BA are associated with alterations in gut microbiota, LPS and, consequently, inflammation [19]. In another recent study in a rat model of VSG, Myronovich et al. have shown that small heterodimer partner (SHP), another orphan nuclear receptor downstream of FXR, is involved in the inflammatory response and in hepatic steatosis [48]. This supports the hypothesis that the BA-FXR pathway is key to understanding how LSG is associated with reduction in pro-inflammatory cytokines and improvements in NAFLD/NASH.
Limitations
This study was limited by only having 6-month post-operative follow-up with more profound changes possibly happening later. Others have reported that the total BA concentration peaked at 1 year after both LSG and RYGB [15], with IL-6 lowest at 12 months after bariatric surgery, with significant changes between 6 and 12 months [49]. Although this is the largest study of BA in patients undergoing LSG to date, the study sample size was relatively small [15, 16]. Future large-scale studies can be designed, with stratification based on severity of NAFLD, and to control the effect of pre-existing T2DM and concomitant medication usage, especially statins.
Further exploration is required of the relationships between individual BA, changes in gut microbiota and improved markers of NAFLD/NASH. These studies will benefit from measurement of circulating LPS, as a marker of gut bacterial load, and 7alpha-hydroxy-4-cholesten-3-one (C4), which is an indirect measure of BA synthesis via the action of the rate-limiting enzyme CYP7A1 [50]. Measurement of faecal BA levels would aid the understanding of changes in BA absorption after LSG [43, 51]. Finally, dynamic measurement of BA in the pre- and postprandial period may be a more accurate reflection of BA production and physiology [52].
Conclusions
The profile of individual BA and enterohepatic circulation is altered after LSG. These changes occur in the presence of reductions in inflammatory cytokines and markers of liver injury. This study supports evidence from recent reports from animal models that sleeve gastrectomy may have an effect on NAFLD/NASH through changes in BA metabolism, probably through the FXR pathway.
References
Das UN. Obesity, metabolic syndrome X, and inflammation. Nutrition. 2002;18(5):430–2.
Caiazzo R et al. Roux-en-Y gastric bypass versus adjustable gastric banding to reduce nonalcoholic fatty liver disease: a 5-year controlled longitudinal study. Ann Surg. 2014;260(5):893–8. discussion 898–9.
Tran A, Gual P. Non-alcoholic steatohepatitis in morbidly obese patients. Clin Res Hepatol Gastroenterol. 2013;37(1):17–29.
Wieckowska A et al. In vivo assessment of liver cell apoptosis as a novel biomarker of disease severity in nonalcoholic fatty liver disease. Hepatology. 2006;44(1):27–33.
Feldstein AE et al. Cytokeratin-18 fragment levels as noninvasive biomarkers for nonalcoholic steatohepatitis: a multicenter validation study. Hepatology. 2009;50(4):1072–8.
Hafeez S, Ahmed MH. Bariatric surgery as potential treatment for nonalcoholic fatty liver disease: a future treatment by choice or by chance? J Obes. 2013;2013:839275.
Modica S, Gadaleta RM, Moschetta A. Deciphering the nuclear bile acid receptor FXR paradigm. Nucl Recept Signal. 2010;8:e005.
Chen X et al. TGR5: a novel target for weight maintenance and glucose metabolism. Exp Diabetes Res. 2011;2011:853501.
Li Y, Jadhav K, Zhang Y. Bile acid receptors in non-alcoholic fatty liver disease. Biochem Pharmacol. 2013;86(11):1517–24.
Haeusler RA et al. Human insulin resistance is associated with increased plasma levels of 12alpha-hydroxylated bile acids. Diabetes. 2013;62(12):4184–91.
Gerhard GS et al. A role for fibroblast growth factor 19 and bile acids in diabetes remission after Roux-en-Y gastric bypass. Diabetes Care. 2013;36(7):1859–64.
Jansen PL et al. Alterations of hormonally active fibroblast growth factors after Roux-en-Y gastric bypass surgery. Dig Dis. 2011;29(1):48–51.
Patti ME et al. Serum bile acids are higher in humans with prior gastric bypass: potential contribution to improved glucose and lipid metabolism. Obesity (Silver Spring). 2009;17(9):1671–7.
Pournaras DJ et al. The role of bile after Roux-en-Y gastric bypass in promoting weight loss and improving glycaemic control. Endocrinology. 2012;153(8):3613–9.
Steinert RE, et al. Bile acids and gut peptide secretion after bariatric surgery: a 1-year prospective randomized pilot trial. Obesity (Silver Spring). 2013.
Haluzikova D et al. Laparoscopic sleeve gastrectomy differentially affects serum concentrations of FGF-19 and FGF-21 in morbidly obese subjects. Obesity (Silver Spring). 2013;21(7):1335–42.
Bechmann LP et al. Free fatty acids repress small heterodimer partner (SHP) activation and adiponectin counteracts bile acid-induced liver injury in superobese patients with nonalcoholic steatohepatitis. Hepatology. 2013;57(4):1394–406.
Myronovych A et al. Vertical sleeve gastrectomy reduces hepatic steatosis while increasing serum bile acids in a weight-loss-independent manner. Obesity (Silver Spring). 2014;22(2):390–400.
Ryan KK et al. FXR is a molecular target for the effects of vertical sleeve gastrectomy. Nature. 2014;509(7499):183–8.
Ooi CP, Loke SC. Colesevelam for type 2 diabetes mellitus. Cochrane Database Syst Rev. 2012;12:CD009361.
Beysen C et al. Effect of bile acid sequestrants on glucose metabolism, hepatic de novo lipogenesis, and cholesterol and bile acid kinetics in type 2 diabetes: a randomised controlled study. Diabetologia. 2012;55(2):432–42.
Chamulitrat W et al. Ursodeoxycholyl lysophosphatidylethanolamide inhibits lipoapoptosis by shifting fatty acid pools toward monosaturated and polyunsaturated fatty acids in mouse hepatocytes. Mol Pharmacol. 2013;84(5):696–709.
Xiang Z et al. The role of ursodeoxycholic acid in non-alcoholic steatohepatitis: a systematic review. BMC Gastroenterol. 2013;13:140.
Owen-Smith A et al. A NICE example? Variation in provision of bariatric surgery in England. BMJ. 2013;346:f2453.
MacLaughlin HL et al. Laparoscopic sleeve gastrectomy is a novel and effective treatment for obesity in patients with chronic kidney disease. Obes Surg. 2012;22(1):119–23.
Wallace TM, Levy JC, Matthews DR. Use and abuse of HOMA modeling. Diabetes Care. 2004;27(6):1487–95.
Tagliacozzi D et al. Quantitative analysis of bile acids in human plasma by liquid chromatography-electrospray tandem mass spectrometry: a simple and rapid one-step method. Clin Chem Lab Med. 2003;41(12):1633–41.
Brunt EM et al. Nonalcoholic fatty liver disease (NAFLD) activity score and the histopathologic diagnosis in NAFLD: distinct clinicopathologic meanings. Hepatology. 2011;53(3):810–20.
Boden G. Obesity and free fatty acids. Endocrinol Metab Clin North Am. 2008;37(3):635–46. viii-ix.
Carswell KA, et al. A systematic review and meta-analysis of the effect of gastric bypass surgery on plasma lipid levels. Obes Surg, 2015.
Rao SR. Inflammatory markers and bariatric surgery: a meta-analysis. Inflamm Res. 2012;61(8):789–807.
Terra X et al. Long-term changes in leptin, chemerin and ghrelin levels following different bariatric surgery procedures: Roux-en-Y gastric bypass and sleeve gastrectomy. Obes Surg. 2013;23(11):1790–8.
Dali-Youcef N et al. Metabolic inflammation: connecting obesity and insulin resistance. Ann Med. 2013;45(3):242–53.
Xu XJ et al. What distinguishes adipose tissue of severely obese humans who are insulin sensitive and resistant? Curr Opin Lipidol. 2013;24(1):49–56.
Diab DL et al. Cytokeratin 18 fragment levels as a noninvasive biomarker for nonalcoholic steatohepatitis in bariatric surgery patients. Clin Gastroenterol Hepatol. 2008;6(11):1249–54.
Kahraman A et al. Fetuin-A mRNA expression is elevated in NASH compared with NAFL patients. Clin Sci (Lond). 2013;125(8):391–400.
Melissas J et al. Alterations of global gastrointestinal motility after sleeve gastrectomy: a prospective study. Ann Surg. 2013;258(6):976–82.
Pournaras DJ, le Roux CW. Are bile acids the new gut hormones? Lessons from weight loss surgery models. Endocrinology. 2013;154(7):2255–6.
Kohli R et al. A surgical model in male obese rats uncovers protective effects of bile acids post-bariatric surgery. Endocrinology. 2013;154(7):2341–51.
Kong LC et al. Gut microbiota after gastric bypass in human obesity: increased richness and associations of bacterial genera with adipose tissue genes. Am J Clin Nutr. 2013;98(1):16–24.
Esteve E, Ricart W, Fernandez-Real JM. Gut microbiota interactions with obesity, insulin resistance and type 2 diabetes: did gut microbiote co-evolve with insulin resistance? Curr Opin Clin Nutr Metab Care. 2011;14(5):483–90.
Monte SV et al. Reduction in endotoxemia, oxidative and inflammatory stress, and insulin resistance after Roux-en-Y gastric bypass surgery in patients with morbid obesity and type 2 diabetes mellitus. Surgery. 2012;151(4):587–93.
Damms-Machado A et al. Effects of surgical and dietary weight loss therapy for obesity on gut microbiota composition and nutrient absorption. Biomed Res Int. 2015;2015:806248.
Pathil A et al. Ursodeoxycholyl lysophosphatidylethanolamide improves steatosis and inflammation in murine models of nonalcoholic fatty liver disease. Hepatology. 2012;55(5):1369–78.
Buko VU et al. Ursodeoxycholic acid dose-dependently improves liver injury in rats fed a methionine- and choline-deficient diet. Hepatol Res. 2011;41(7):647–59.
Luo L et al. Evaluation of serum bile acid profiles as biomarkers of liver injury in rodents. Toxicol Sci. 2014;137(1):12–25.
Aranha MM et al. Bile acid levels are increased in the liver of patients with steatohepatitis. Eur J Gastroenterol Hepatol. 2008;20(6):519–25.
Myronovych A et al. The role of small heterodimer partner in nonalcoholic fatty liver disease improvement after sleeve gastrectomy in mice. Obesity (Silver Spring). 2014;22(11):2301–11.
Illan-Gomez F et al. Obesity and inflammation: change in adiponectin, C-reactive protein, tumour necrosis factor-alpha and interleukin-6 after bariatric surgery. Obes Surg. 2012;22(6):950–5.
Mudaliar S et al. Efficacy and safety of the farnesoid X receptor agonist obeticholic acid in patients with type 2 diabetes and nonalcoholic fatty liver disease. Gastroenterology. 2013;145(3):574–82 e1.
Li JV et al. Metabolic surgery profoundly influences gut microbial-host metabolic cross-talk. Gut. 2011;60(9):1214–23.
Werling M et al. Enhanced fasting and post-prandial plasma bile acid responses after Roux-en-Y gastric bypass surgery. Scand J Gastroenterol. 2013;48(11):1257–64.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Compliance with Ethical Standards
Informed consent was obtained from all individual participants included in the study. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Conflict of Interest
The authors declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Belgaumkar, A.P., Vincent, R.P., Carswell, K.A. et al. Changes in Bile Acid Profile After Laparoscopic Sleeve Gastrectomy are Associated with Improvements in Metabolic Profile and Fatty Liver Disease. OBES SURG 26, 1195–1202 (2016). https://doi.org/10.1007/s11695-015-1878-1
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-015-1878-1