
Abstract
Though primary bariatric surgery is now firmly established as the first-line treatment for morbid obesity, this is not the case with revisional bariatric surgery. Despite proven benefits and patient demand, revisional bariatric surgery continues to attract controversy. Even though it is widely believed to be riskier and less effective than primary bariatric surgery, there is currently no systematic review in literature addressing this point. This review aims to establish outcomes after revisional bariatric surgery in comparison with those after primary bariatric surgery. Since Roux-en-Y gastric bypass or sleeve gastrectomy is currently the commonest anatomy achieved after revisional bariatric surgery, this review focuses on the outcome of revisional Roux-en-Y gastric bypass and revisional sleeve gastrectomy in comparison with respective primary procedures.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
A number of studies have now confirmed safety and efficacy of revisional bariatric surgery (RBS) [1]. Though some studies have shown inferior weight loss with RBS [2–4], others have not. At the same time, some authors [5, 6] have shown that inferior weight loss with RBS does not come at the cost of inferior comorbidity resolution. Similarly, while many studies have shown higher complication rates with RBS compared to primary bariatric surgery (PBS) [2, 7], our group [8] and others have performed RBS with exceptional safety and reported complication rates similar to PBS. Risks as well as the benefits with RBS depend on the nature of primary [2, 6] as well as the secondary procedure. For example, revisions of adjustable gastric banding (AGB) and sleeve gastrectomy (SG) carry fewer risks than revisions from vertical banded gastroplasty (VBG), horizontal gastroplasty, and Roux-en-Y gastric bypass (RYGB) [2, 3, 6, 7, 9, 10]. Similarly, a revision to RYGB carries lower risks than revision to duodenal switch (DS) and higher risks than revision to SG [10]. A number of cases that need conversion from VBG and horizontal gastroplasty are decreasing worldwide as these procedures are no longer carried out. Moreover, these revisions are often carried out for strong clinical reasons other than poor weight loss. Furthermore, it has been shown [10] that careful patient selection, attention to technical details, and systematic approach can remarkably improve safety of revisional procedures. Success of any bariatric surgery, primary or revisional, largely rests on patient’s ability to make long-term behavioural changes. Any attempt at RBS must hence be accompanied by correction of any persistent adverse underlying dietetic, psychological, and behavioural factors.
There is no randomised controlled trial in scientific literature comparing RBS with “no” RBS in patients deemed suitable for RBS. Indeed, such a trial may even be considered unethical. Given these difficulties, surgeons are left with no choice but to compare RBS with PBS to understand its safety and efficacy. It is important to understand that the choice these patients face is not whether they can get RBS or PBS; the choice lies between RBS or nothing, and in this context, even lower gains at higher risks may be considered acceptable as long as patients are fully aware of the altered risk versus benefit ratio. There are other practical problems with such comparison. These patients may already have lost some weight with the PBS, and indeed, sum total of weight loss with their original operation and RBS in these patients is often similar to that would be achieved with a PBS [9, 11, 12]. Finally, patients undergoing RBS may have a different starting body mass index (BMI) and a more advanced “disease” [9].
Despite these obvious academic issues, it is not too difficult to comprehend the reason behind studies comparing RBS with PBS. Given the difficulties in carrying out randomised studies, and limited value of case series and cohort studies, these studies provide us with the closest study design to study the comparative usefulness of RBS. This article aims to systematically review a variety of nonrandomised studies comparing safety and efficacy of RBS in comparison with PBS in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Since Roux-en-Y gastric bypass and sleeve gastrectomy are the commonest revisional procedures performed currently, we focus on these two procedures.
Methods
An online search of PubMed, Medline, Embase, and Google Scholar was independently carried out by two researchers using keywords “revisional bariatric surgery”, “revisional sleeve gastrectomy”, “revisional gastric bypass”, “band-to-bypass conversion”, and “band-to-sleeve conversion” to identify all articles written on the topics of RBS. Articles were also identified from references of relevant articles. The last of these searches was carried out on 17 January 2015.
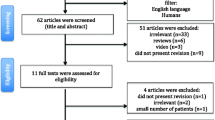
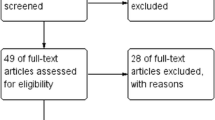
A total of 290 articles were finally identified after excluding duplicates. Initial search revealed 26 articles comparing revisional and primary bariatric surgery. Articles published in other languages [13] were excluded, as well as those that dealt with a mixture of primary and revisional surgeries [10, 14], making comparison difficult or those that analysed variations of procedures (resectional gastric bypass) not currently popular [15]. An earlier study [16], which compared PBS with revisions mainly from jejuno-ileal bypass, was also excluded, as most bariatric surgeons are unlikely to encounter patients needing revisions from jejuno-ileal bypass in their routine practice. Articles (21 in total) comparing primary and revisional SG (n = 7) and primary and revisional RYGB (n = 14) were systematically reviewed. The article by Germanova et al. [17] was excluded from cumulative quantitative analysis, as authors did not detail basic demographics, complication rates, and weight loss separately for primary and revisional sleeve gastrectomy patients. While using data for quantitative analysis from two papers by the same group of Thereaux et al. [18, 19] comparing results with primary and revisional RYGB, care was taken to avoid duplicate entry of overlapping data and only one set of data was used. Median values were not included in cumulative analysis. Values of all the parameters were not available for every study. This was taken into account when calculating cumulative percentages. We did not use any statistical comparison of data between primary and revisional group, as there will be significant risks of error in absence of raw data for any of these studies and their heterogeneous nature. Figure 1 shows a PRISMA flow chart for article selection.

PRISMA flow chart for article selection
Results
This review identified a total of 21 studies comparing primary and revisional Roux-en-Y gastric bypass (n = 14) and primary and revisional sleeve gastrectomy (n = 7). Studies were separated into two groups: those that compared outcomes of primary and revisional RYGB and those that compared outcomes of primary and revisional SG. Table 1 [2–5, 7–9, 11, 12, 17–28] lists qualitative characteristics of these studies.
Revisional RYGB Versus Primary RYGB
Nine of the 14 studies comparing primary and revisional RYGB did not find any significant difference in complication rates between two groups. There was no difference in mortality between two groups in any of these studies.
Similarly, though 9 out of 14 studies found inferior weight loss outcomes in revisional RYGB group, it is worth noting that all of these studies used pre-revisional surgery weight as the reference point.
Cumulative Comparative Results of Revisional and Primary RYGB
Table 2 lists comparative cumulative data for primary and revisional RYGB. Fourteen studies compared outcomes of revisional RYGB with those seen after primary RYGB. A total of 986 patients undergoing revisional RYGB were compared with 4,067 primary RYGB patients. The mean age of patients was 45.3 and 43.5 years in revisional and primary group, respectively. Females accounted for 87 % patients in revisional group as compared to 79.6 % in primary group. The mean preoperative BMI was 47.8 and 49.8 kg/m2, respectively, in revisional and primary groups. Mean operative time was 201.6 min in revisional group compared to 127 min in primary group. Mean hospital stay in revisional and primary group was 5.8 and 4.5 days, respectively.
The complication rate was 29.5 % in revisional group compared to 13.9 % in primary group, and the respective reoperation rates were 8.4 and 8.6 %. A mortality rate of 1.3 % (n = 7/541) was observed in revisional group compared with 0.2 % (n = 8/4067) in primary group. Most (six out of seven) mortality in revisional group were reported by Zhang et al. [2]. Leak rate was 5.8 % in revisional group compared to 1.0 % in primary group.
Weight loss was not analysed cumulatively due to significant heterogeneity amongst studies. Weight loss data were available in 13 out of the 14 studies. Out of these, ten studies reported inferior weight loss with revisional RYGB, whereas two of them did not find any significant difference. A further two reported no significant difference in weight loss if pre-banding weight was used as the index point.
Revisional Sleeve Gastrectomy Versus Primary Sleeve Gastrectomy
Two of the seven studies comparing primary and revisional SG showed higher complication rates with revisional sleeve gastrectomy. There was no difference in mortality in any study. Weight loss outcomes were not available in two studies, not significantly different in three, and inferior in revisional group in two.
Cumulative Comparative Results of Revisional and Primary SG
Table 3 lists comparative cumulative data for primary and revisional SG. Seven studies compared outcomes of revisional SG with those seen after primary SG. A total of 541 patients undergoing revisional SG were compared with 1,861 primary SG patients. The mean age of patients was 42.1 and 42.7 years in revisional and primary group, respectively. There were 90.1 % females in revisional group compared to 74.9 % in primary group. The mean preoperative BMI was 42.7 and 48.6 kg/m2, respectively, in revisional and primary groups. Mean operative time was 133.2 min in revisional group compared to 106 min in primary group. Mean hospital stay in revisional and primary group was 3.8 and 3.6 days, respectively.
The complication rate was 10.5 % in revisional group compared to 5.2 % in primary group, and the respective reoperation rates were 4.8 and 1.6 %. Zero mortality (n = 0/541) was observed in revisional group compared with 0.1 % (n = 2/1861) in primary group, but there is clearly potential for type II error due to small dataset. Leak rate was 1.9 % in revisional group compared to 1.5 % in primary group.
Weight loss was not analysed cumulatively due to significant heterogeneity amongst studies. Weight loss data were available in five out of the seven studies. Out of these, two studies reported inferior weight loss with revisional SG, whereas the other three did not find any significant difference.
Discussion
Obesity is a chronic disease [29], and like many other chronic diseases, there is no treatment available which will cure all patients at various stages of their disease. Different patients will need different treatment, and any patient will not respond to the same treatment at different stages of their disease. Moreover, it is now widely recognised that identification and correction of contributory dietetic, psychological, and behavioural factors must go hand in hand with any surgical intervention for obesity. Treatment strategies for many chronic diseases contain well-established algorithms with escalation of treatment strategy, a natural back up for failures with first-line treatments. Viewed in this way, RBS is simply an escalation of treatment strategy, not vastly dissimilar to what insulin treatment is for those who do not respond to or have side effects with first-line antidiabetic medications. The only justification that one should hence need for RBS is whether the risks of RBS are outweighed by the benefits. This question has not yet been and perhaps cannot be answered with level 1 evidence given the sheer number of studies now reporting on the safety and efficacy of RBS [10, 29–32].
Revisional bariatric surgery is increasingly becoming more and more popular all over the world and poses significant questions for policy makers and funders all over the world. This is the first systematic review of studies comparing primary and revisional bariatric surgery in scientific literature. Since RYGB and SG account for the majority of RBS final anatomy, we concentrated our efforts on these procedures. The authors acknowledge that there are other successful forms of RBS.
Two almost contrasting trends emerge from our study from qualitative examination of studies and quantitative comparison of data within them. Our qualitative analysis found that most studies comparing primary and revisional Roux-en-Y gastric bypass and sleeve gastrectomy did not show any significant difference in complication rates, reoperations, and mortality between the two groups. It is entirely possible that this simply reflects type II error as most of these studies are based on small sample sizes. Similarly, though many studies showed inferior weight loss with revisional Roux-en-Y gastric bypass and two have also shown inferior weight loss with revisional sleeves, this must partly be due to the fact that studies have used pre-revisional bariatric surgery weight as the index weight. Furthermore, many patients undergo revisional surgery because of their inability to maintain or achieve a satisfactory oral intake. Many of these patients indeed end up gaining weight after revisional bariatric surgery.
At the same time, quantitative cumulative data comparison in our study suggests that RBS is technically more challenging to carry out, takes more time, is associated with longer hospital stay, and is associated with higher risk of complications and reoperations. Revisional RYGB group also had higher mortality, but this was not the case with revisional SG. Weight loss data is more complex to understand because of varying start points, but generally, it would be fair to assume that revisional RYGB and SG result in slightly poorer weight loss compared to primary RYGB and SG, respectively. It is not entirely clear whether this translates into a significantly inferior comorbidity resolution rates.
Exact risk associated with RBS will obviously depend on the patient characteristics, primary procedure, reason for RBS, the nature of revisional procedure, and experience of the surgical team. Though any well-trained bariatric surgeon can safely carry out procedures at lower end of complexity, it is only logical that complex, high risk, and revisional work is carried out by high-volume experts in dedicated centres. There needs to be some thinking around provision of RBS within every geographical area to allow for development, concentration, and maintenance of expertise. It is worth noting in this context that National Institute of Health and Care Excellence (NICE) guidelines in UK recommend that revisional bariatric surgery “should be undertaken only in specialist centres by surgeons with extensive experience because of the high rate of complications and increased mortality”.
Many patients need RBS when they would not have met commonly accepted BMI criteria for primary bariatric intervention. Usually, these are patients where primary procedure has resulted in a complication but has been successful from the point of view of weight loss and improvement in comorbidities. In some of these patients, correction of complication (for example, troublesome acid reflux after SG) will need a different bariatric procedure, but in other cases, it may be possible to treat complication by simply removing the causative factor but at the risk of recurrence of obesity or its associated comorbidities (for example, removal of a slipped band). Aarts et al. [33] have shown that patients who had their gastric band removed without any RBS were “guaranteed” to regain weight. Whether RBS can be safely offered to these patients with lower weight and BMI is not a matter of dispute anymore [34]. Applying criteria used for primary bariatric surgery to these patients will only mean that most of them will come back with a more advanced disease and lose the previous gains. This is something policy makers and funders will have to factor into their decision-making.
There is another subgroup of patients. These are the people who have obtained some weight loss from their PBS and have now fallen below the qualifying criteria. Such patients often seek RBS, as they have not reached their own perceived “ideal” body weight. In this context, it is important to understand that criteria for primary bariatric intervention have been agreed after a thorough risk versus benefit analysis of bariatric/metabolic surgery at a given BMI. If anything, the risk versus benefit ratio is likely to be higher for RBS for these patients, making RBS even less justified on clinical grounds. It would hence seem reasonable to apply the existing primary bariatric surgery criteria to those who have achieved some weight loss with their PBS and have now fallen below the qualifying BMI.
There is a third group of patients who have achieved satisfactory results from a PBS but have still not achieved BMI or a state of health that will put them beyond the qualifying criteria for primary intervention. We feel the decision-making for such patients should be left to the individual MDT. If these patients can benefit from a further surgical procedure and if it can be justified on clinical grounds, RBS may be a valid clinical choice for these patients. Indeed, such thinking has formed the basis of many “staged” treatment approaches bariatric surgeons routinely use.
Some surgeons [1, 9] have suggested that a restrictive procedure needing conversion for inadequate weight loss should preferably be converted to one that also provides a degree of malabsorption. Elnahas et al. [1] demonstrated superior outcome with revisional RYGB and bilio-pancreatic diversion (BPD)/DS for converting a gastric band in their systematic review of revisional surgery after failed AGB; weight loss was not sustained in the SG group. In their systematic review of 106, 514, and 71 conversions of AGB to SG, RYGB, and BPD/DS, respectively, they reported an excess weight loss (EWL) of 60, 22, and 35.3 % at 6–12, 12–24, and 24–48 months, respectively. The EWL for RYGB at the same follow-up period were 46.3, 57.8, and 48.2 %, respectively, and corresponding numbers for the BPD/DS group were 18, 47.1, and 78.4 %. Others have also advocated adding malabsorptive element to failures after purely revisional procedures. However, this approach may not hold for those needing conversions for reasons other than inadequate weight loss. Moreover, procedures like BPD/DS do carry higher risks even as primary procedures, and significant malabsorption associated with these procedures has its own problems. This review is not qualified to comment on the safety and efficacy of BPD/DS for revisions from other procedures.
As discussed earlier, comparison between revisional and primary bariatric surgery is somewhat arbitrary and can even be considered unfair as the choice these patients face is not between revisional and primary procedure but between revisional surgery or “no” surgery. For patients suffering with complication of primary bariatric surgery, revisional surgery is practically the only available option that will allow them to maintain and/or further the weight loss achieved with their primary procedure. Revisional bariatric surgery is being driven by patient demand and is perhaps a reflection of the fact that an ideal bariatric intervention still eludes us. Many of these patients have undergone procedures that are now considered obsolete.
Conclusion
Revisional RYGB and SG appear to carry a higher but acceptable complication and reoperation rates in comparison with respective primary procedures. Weight loss achieved is inferior but still significant. Bariatric surgeons should treat revisional procedures with caution.
Abbreviations
- RBS:
-
Revisional bariatric surgery
- PBS:
-
Primary bariatric surgery
- AGB:
-
Adjustable gastric banding
- SG:
-
Sleeve gastrectomy
- VBG:
-
Vertical banded gastroplasty
- RYGB:
-
Roux-en-Y gastric bypass
- DS:
-
Duodenal switch
- PRISMA:
-
Preferred Reporting Items for Systematic Reviews and Meta-Analyses
- EWL:
-
Excess weight loss
- NICE:
-
National Institute for Health and Care Excellence
- BPD:
-
Bilio-pancreatic diversion
References
Elnahas A, Graybiel K, Farrokhyar F, et al. Revisional surgery after failed laparoscopic adjustable gastric banding: a systematic review. Surg Endosc. 2013;27(3):740–5.
Zhang L, Tan WH, Chang R, et al. Perioperative risk and complications of revisional bariatric surgery compared to primary Roux-en-Y gastric bypass. Surg Endosc. 2014.
Mor A, Keenan E, Portenier D, et al. Case-matched analysis comparing outcomes of revisional versus primary laparoscopic Roux-en-Y gastric bypass. Surg Endosc. 2013;27(2):548–52.
Delko T, Köstler T, Peev M, et al. Revisional versus primary Roux-en-Y gastric bypass: a case-matched analysis. Surg Endosc. 2014;28(2):552–8.
Slegtenhorst BR, van der Harst E, Demirkiran A, et al. Effect of primary versus revisional Roux-en-Y gastric bypass: inferior weight loss of revisional surgery after gastric banding. Surg Obes Relat Dis. 2013;9(2):253–8.
McKenna D, Selzer D, Burchett M, et al. Revisional bariatric surgery is more effective for improving obesity-related co-morbidities than it is for reinducing major weight loss. Surg Obes Relat Dis. 2014;10(4):654–9.
Radtka 3rd JF, Puleo FJ, Wang L, et al. Revisional bariatric surgery: who, what, where, and when? Surg Obes Relat Dis. 2010;6(6):635–42.
Jennings NA, Boyle M, Mahawar K, et al. Revisional laparoscopic Roux-en-Y gastric bypass following failed laparoscopic adjustable gastric banding. Obes Surg. 2013;23(7):947–52.
Mohos E, Jánó Z, Richter D, et al. Quality of life, weight loss and improvement of co-morbidities after primary and revisional laparoscopic roux y gastric bypass procedure-comparative match pair study. Obes Surg 2014.
Stefanidis D, Malireddy K, Kuwada T, et al. Revisional bariatric surgery: perioperative morbidity is determined by type of procedure. Surg Endosc. 2013;27(12):4504–10.
Barrett AM, Vu KT, Sandhu KK, et al. Primary sleeve gastrectomy compared to sleeve gastrectomy as revisional surgery: weight loss and complications at intermediate follow-up. J Gastrointest Surg. 2014;18(10):1737–43.
te Riele WW, Sze YK, Wiezer MJ, et al. Conversion of failed laparoscopic gastric banding to gastric bypass as safe and effective as primary gastric bypass in morbidly obese patients. Surg Obes Relat Dis. 2008;4(6):735–9.
Stroh C, Weiner R, Wolff S, et al. Arbeitsgruppe Adipositaschirurgie, Kompetenznetz Adipositas. [Revisional surgery and reoperations in obesity and metabolic surgery: data analysis of the German bariatric surgery registry 2005–2012.] [Article in German] Chirurg. 2014.
Inabnet 3rd WB, Belle SH, Bessler M, et al. Comparison of 30-day outcomes after non-LapBand primary and revisional bariatric surgical procedures from the longitudinal assessment of bariatric surgery study. Surg Obes Relat Dis. 2010;6(1):22–30.
Martin MJ, Mullenix PS, Steele SR, et al. A case-match analysis of failed prior bariatric procedures converted to resectional gastric bypass. Am J Surg. 2004;187(5):666–70.
Owens BM, Owens ML, Hill CW. Effect of revisional bariatric surgery on weight loss and frequency of complications. Obes Surg. 1996;6(6):479–84.
Germanova D, Loi P, van Vyve E, et al. Previous bariatric surgery increases postoperative morbidity after sleeve gastrectomy for morbid obesity. Acta Chir Belg. 2013;113(4):254–7.
Thereaux J, Veyrie N, Barsamian C, et al. Similar postoperative safety between primary and revisional gastric bypass for failed gastric banding. JAMA Surg. 2014;149(8):780–6.
Thereaux J, Corigliano N, Poitou C, et al. Five-year weight loss in primary gastric bypass and revisional gastric bypass for failed adjustable gastric banding: results of a case-matched study. Surg Obes Relat Dis. 2014. doi:10.1016/j.soard.2014.04.031.
Silecchia G, Rizzello M, De Angelis F, et al. Laparoscopic sleeve gastrectomy as a revisional procedure for failed laparoscopic gastric banding with a “2-step approach”: a multicenter study. Surg Obes Relat Dis. 2014;10(4):626–31.
Noel P, Schneck AS, Nedelcu M, et al. Laparoscopic sleeve gastrectomy as a revisional procedure for failed gastric banding: lessons from 300 consecutive cases. Surg Obes Relat Dis. 2014. doi:10.1016/j.soard.2014.02.045.
Alqahtani AR, Elahmedi M, Alamri H, et al. Laparoscopic removal of poor outcome gastric banding with concomitant sleeve gastrectomy. Obes Surg. 2013;23(6):782–7.
Rebibo L, Mensah E, Verhaeghe P, et al. Simultaneous gastric band removal and sleeve gastrectomy: a comparison with front-line sleeve gastrectomy. Obes Surg. 2012;22(9):1420–6.
Gagnière J, Slim K, Launay-Savary MV, et al. Previous gastric banding increases morbidity and gastric leaks after laparoscopic sleeve gastrectomy for obesity. J Visc Surg. 2011;148(3):e205–9.
Topart P, Becouarn G, Ritz P. One-year weight loss after primary or revisional Roux-en-Y gastric bypass for failed adjustable gastric banding. Surg Obes Relat Dis. 2009;5(4):459–62.
Zingg U, McQuinn A, DiValentino D, et al. Revisional vs. primary Roux-en-Y gastric bypass—a case-matched analysis: less weight loss in revisions. Obes Surg. 2010;20(12):1627–32.
Deylgat B, D’Hondt M, Pottel H, et al. Indications, safety, and feasibility of conversion of failed bariatric surgery to Roux-en-Y gastric bypass: a retrospective comparative study with primary laparoscopic Roux-en-Y gastric bypass. Surg Endosc. 2012;26(7):1997–2002.
Navez J, Dardamanis D, Thissen JP, et al. Laparoscopic Roux-en-Y gastric bypass for morbid obesity: comparison of primary versus revisional bypass by using the BAROS score. Obes Surg. 2014.
Shimizu H, Annaberdyev S, Motamarry I, et al. Revisional bariatric surgery for unsuccessful weight loss and complications. Obes Surg. 2013;23(11):1766–73.
Brethauer SA, Kothari S, Sudan R, et al. Systematic review on reoperative bariatric surgery: American Society for Metabolic and Bariatric Surgery Revision Task Force. Surg Obes Relat Dis. 2014. doi:10.1016/j.soard.2014.02.014.
Cheung D, Switzer NJ, Gill RS, et al. Revisional bariatric surgery following failed primary laparoscopic sleeve gastrectomy: a systematic review. Obes Surg. 2014;24(10):1757–63.
Coblijn UK, Verveld CJ, van Wagensveld BA, et al. Laparoscopic Roux-en-Y gastric bypass or laparoscopic sleeve gastrectomy as revisional procedure after adjustable gastric band—a systematic review. Obes Surg. 2013;23(11):1899–914.
Aarts EO, Dogan K, Koehestanie P, et al. What happens after gastric band removal without additional bariatric surgery? Surg Obes Relat Dis. 2013. doi:10.1016/j.soard.2013.10.014.
Walker DM, Hii MW, Skinner CE, et al. Roux-en-Y gastric bypass after successful weight loss with a laparoscopic adjustable gastric band: rationales and early outcomes in patients of body mass index <35 kg/m2. Surg Obes Relat Dis. 2014.
Conflict of Interest
The authors declare that they have no conflict of interest.
Author Contribution
KM conceived the idea for the topic. KM and YG independently collected information and analysed it. All authors participated in departmental discussion on the topic and manuscript writing. All authors have seen the final version and approve it.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Mahawar, K.K., Graham, Y., Carr, W.R.J. et al. Revisional Roux-en-Y Gastric Bypass and Sleeve Gastrectomy: a Systematic Review of Comparative Outcomes with Respective Primary Procedures. OBES SURG 25, 1271–1280 (2015). https://doi.org/10.1007/s11695-015-1670-2
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-015-1670-2